Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Selective sebaceous gland electrothermolysis as a treatment
Jin W. Lee1, MD, Beom J. Kim1, MD, PhD, Myeung N. Kim1, MD, PhD, and
Although many therapeutic options exist for acne, relapse often occurs after treatment is
stopped. Some preliminary evidence suggests that selective electrothermolysis of the seba-
ceous glands may represent a novel therapeutic intervention. This trial was conducted to
evaluate the efficacy and tolerability of selective sebaceous gland electrothermolysis for the
treatment of facial acne. Twelve patients with facial acne were enrolled, all of whom under-
went three sessions of therapy. During each session, a 1.5-mm-long needle with 0.45-mm
of base insulation was inserted into pores of acne lesions. Upon insertion, a high-frequency
electrical current was applied for 0.25–0.50 s, for a total output of 40 W. Each treatment
session took approximately 30–60 min. Subject response to therapy was evaluated at
1 month and 12 months after the final treatment. All the enrolled subjects completed the
study and all reported satisfaction with treatment results. In all cases, a reduction in inflam-
matory and non-inflammatory lesion counts was observed after three sessions of selective
electrothermolysis, although a few small papules and comedones persisted in several
areas of untreated facial skin. Mean lesion reduction at 1 month after the final treatment
was 98.14% for inflammatory lesions and 83.09% for non-inflammatory lesions. Clinical
success was achieved in the majority of patients (seven of 12 patients) at 1 month after
the second treatment, and in all patients at 1 month after the final treatment. All patients
reported transient post-treatment erythema, which faded after a few days. Clinically evident
relapse occurred in two of 12 patients (16.7%) 1 year after the final treatment session.
Selective sebaceous gland electrothermolysis can be a safe and effective method of
achieving consistent remission in acne.
therapeutic options for acne vulgaris, relapse is common
after treatments are stopped, although relapse rates after
Acne vulgaris is a chronic inflammatory disease of the
isotretinoin treatment are relatively low if the drug is
pilosebaceous units, which is characterized by comedones,
administered at the correct dose for the correct period.
papules, pustules and nodules, and often results in signifi-
However, because of side-effects such as mild cheilitis
cant facial scarring. Epidemiologic studies estimate that
(dryness of lips), mild xerosis, epistaxis, as well as eleva-
as many as 80% of individuals between the ages of
tion of serum glutamic oxaloacetic transaminase (SGOT),
11 years and 30 years are affected by this common condi-
serum glutamic pyruvic transaminase (SGPT), cholesterol
tion. The pathogenesis of acne is deceptively complex:
and triglycerides, some patients have difficulty in comply-
seborrhea, abnormal pilosebaceous duct cornification,
ductal colonization with Propionibacterium acnes and
Preliminary evidence suggests that selective electro-
secondary inflammatory processes are all implicated in
thermolysis of the sebaceous glands using the method
the underlying etiology. As well as the obvious facial dis-
proposed by Kobayashi and Tamada3 may represent an
figurement, acne is also associated with significant psy-
additional therapeutic option for facial acne. We under-
chological morbidity, including emotional debilitation,
took this study to evaluate the efficacy and tolerability of
embarrassment, poor self-esteem and social isolation.
this modality. In a 1-year follow-up evaluation, we also
Accordingly, an ongoing need for quality medical
attempted to quantify the rate of recurrence in treated
resources and treatments exists.1 Although there are many
ª 2011 The International Society of Dermatology
International Journal of Dermatology 2011
Sebaceous gland electrothermolysis in acne
those used in the preceding session. Complete lesion counts
and subject response rates were assessed 1 month after the
final treatment. Subjects were also evaluated for remission
This was a prospective pilot study. Twelve Korean patients with
rates 1 year after the final treatment. All subjects were
moderate to severe facial acne [according to Investigator’s
prohibited from using any anti-acne treatment (except for
2 Global Assessment (IGA) scores] (Table 1) were enrolled. All
standard washing and moisturizing procedures) while enrolled
subjects had Fitzpatrick skin types III–V. Exclusion criteria
included any use of oral antibiotics or isotretinoin for the
treatment of acne within the previous 6 months, use of topical
or systemic antibiotics within the previous 2 weeks, and
The patients were photographed at each visit. On each
pregnancy or lactation in female subjects. Additionally, women
occasion, subjects were photographed by the same
using hormonal forms of contraception with anti-androgenic
photographer in the same position, using identical camera and
properties for <12 weeks were precluded from enrolling. The
lighting settings. To evaluate efficacy, two variables were used:
mean age of the subjects was 24.6 ± 3.4 years (range: 20–
overall success rate (defined as the percentage of patients
32 years). The group consisted of six women and six men.
rated as ‘‘clear’’ or ‘‘almost clear’’ on the IGA), and net change
Table 2 summarizes participant demographics. The study was
in the number of facial acne lesions. All lesion counts included
approved by the Institutional Review Board of Chung-Ang
both inflammatory (papules, pustules, nodules) and non-
University Hospital. Written informed consent was obtained
inflammatory (open and closed comedones) lesions. Lesions
from all patients prior to treatment.
were assessed on the face only. At each visit, a blinded
physician counted the number of facial acne lesions on each
subject’s face. This same blinded physician also assessed the
Before treatment, each subject’s face was gently cleansed with
overall success rate before each treatment and 1 month after
a mild cleanser prior to the application of a topical anesthetic
the final session and documented any side-effects. At the end
3 cream (EMLAÒ; AstraZeneca Pharmaceuticals LP, Wilmington,
of the study, subjects were asked to rate their level of
DE, USA). After 30 min, the anesthetic was removed and the
satisfaction with the final results of the treatment on a 4-point
subject was asked to adopt a supine position prior to the
scale (4 = very satisfied, 3 = satisfied, 2 = slightly satisfied,
initiation of treatment. Throughout the duration of the
1 = unsatisfied). One year after the last session, all subjects
procedure, ·2 to ·3 magnifying lenses were used by study
returned for a final follow-up evaluation at which treatment-
personnel. Acne lesions (comedonal acne lesions and
specific recurrence was assessed. Specifically, any treated
inflammatory acne lesions) were identified, the surrounding skin
patient in whom acne was rated as ‘‘mild,’’ ‘‘moderate,’’
was stretched and a 1.5-mm-long needle with a 0.45-mm base
‘‘severe’’ or ‘‘very severe’’ on the IGA was considered to have
insulation was inserted into the center of the lesional follicular
suffered a relapse. Treatment effects were determined based
pore at an angle of 60–70° (Fig. 1). Using an electrosurgical
on statistical analysis using the Wilcoxon signed rank test to
apparatus (IME-HR 5000; IME Co. Ltd., Tokyo, Japan), a high-
compare lesion counts at each follow-up visit with baseline
frequency current was then applied for 0.25–0.50 s at an
counts. A P-value of <0.05 was considered to indicate statistical
intensity of approximately 40 W. Treatment duration was about
10 min per 10 lesions treated. The day after the procedure, the
contents of the comedo or inflammatory lesion (e.g. pus) were
expressed by applying gentle pressure. All subjects underwent
a total of three treatment sessions at 1-month intervals. During
All subjects completed the study and all showed a reduc-
the second and last treatments, the operator deliberately
tion in inflammatory and non-inflammatory acne lesions
inserted the needles in directions that differed slightly from
after three selective electrothermolysis treatments. Clinical
Table 1 Investigator’s global assessment
Residual hyperpigmentation and erythema may be present
A few scattered comedones and a few (<5) small papules
Easily recognizable; less than half the face is involved. Many comedones and many papules and pustules
More than half of the face is involved. Numerous comedones, papules and pustules
Entire face is involved. Covered with comedones, numerous papules and pustules and few nodules and cysts
Highly inflammatory acne covering the face; nodules and cysts are present
International Journal of Dermatology 2011
ª 2011 The International Society of Dermatology
Sebaceous gland electrothermolysis in acne
side-effect was transient erythema at the sites of treated
lesions. The inflammatory content (pus) released by gentle
pressure spread to the surrounding tissue, inducing ery-
thema and further inflammation. Although this occurred
in all subjects, the redness typically faded within several
days and seldom persisted for a week. Other severe
adverse events – such as pigmentary alterations, scarring
and infections – were not reported. One year after the final
treatment, two of 12 patients (16.7%) were found to have
relapsed. However, in both cases, the acne was rated as
Lloyd and Mirkov4 first reported selective sebaceous
gland photothermolysis as an effective treatment for acne.
These authors employed a long-pulse diode laser with a
Figure 1 In selective electrothermolysis in the treatment of
wavelength of 810 nm to destroy enlarged sebaceous
acne, a fine needle with an insulated coating is inserted into
glands preloaded with indocyanine green chromophore.4
the center of the follicular orifice and used to deliver an
electrical current, after which an extractor is used to remove
Kobayashi and Tamada3 demonstrated that selective seba-
ceous gland electrothermolysis is a safe and effective ther-
apeutic option for facial seborrhea. They also showed
that a decreased number of sebaceous glands and the for-
examples are shown in Figs 2 and 3. One month after the
mation of fibrosis were observed after selective sebaceous
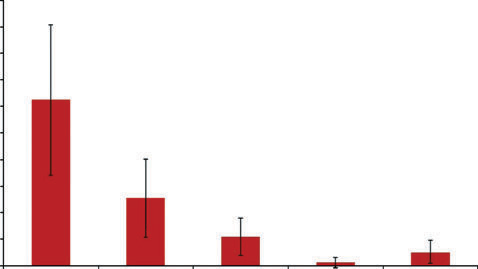
first treatment, the mean reduction in acne lesions was
gland electrothermolysis in a preliminary histologic
59.20% for inflammatory-type lesions (P < 0.01) and
study.3 Together, the results from these studies suggest
48.64% for non-inflammatory lesions (P < 0.01). One
that this technique may represent a new therapeutic
month after the second treatment, the mean reduction in
acne lesions was 82.96% for inflammatory lesions
Here, we show that selective sebaceous gland electro-
(P < 0.01) and 69.79% for non-inflammatory lesions
thermolysis effectively treats acne; all our subjects
(P < 0.01). One month after the final treatment, the mean
reported satisfaction with the treatment in their self-
reduction in acne lesions was 98.14% for inflammatory
assessment surveys. Other than transient erythema and
lesions (P < 0.01) and 83.09% for non-inflammatory
mild dryness, no adverse events were observed in any of
lesions (P < 0.01). In terms of the overall success rate,
the subjects. Our data also indicate a low relapse rate
clinical success was achieved in the majority of patients
after this specific therapy: only a few tiny papules or com-
(seven of 12 patients) 1 month after the second treatment
edones were observed in untreated areas of skin in a few
and in all cases at 1 month after the final session.
patients. We also presume that more than three treatment
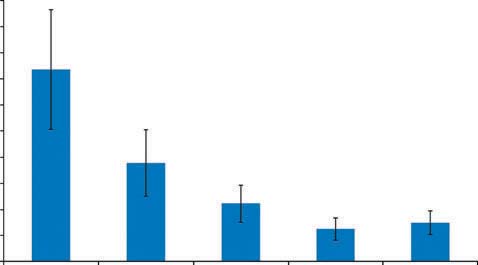
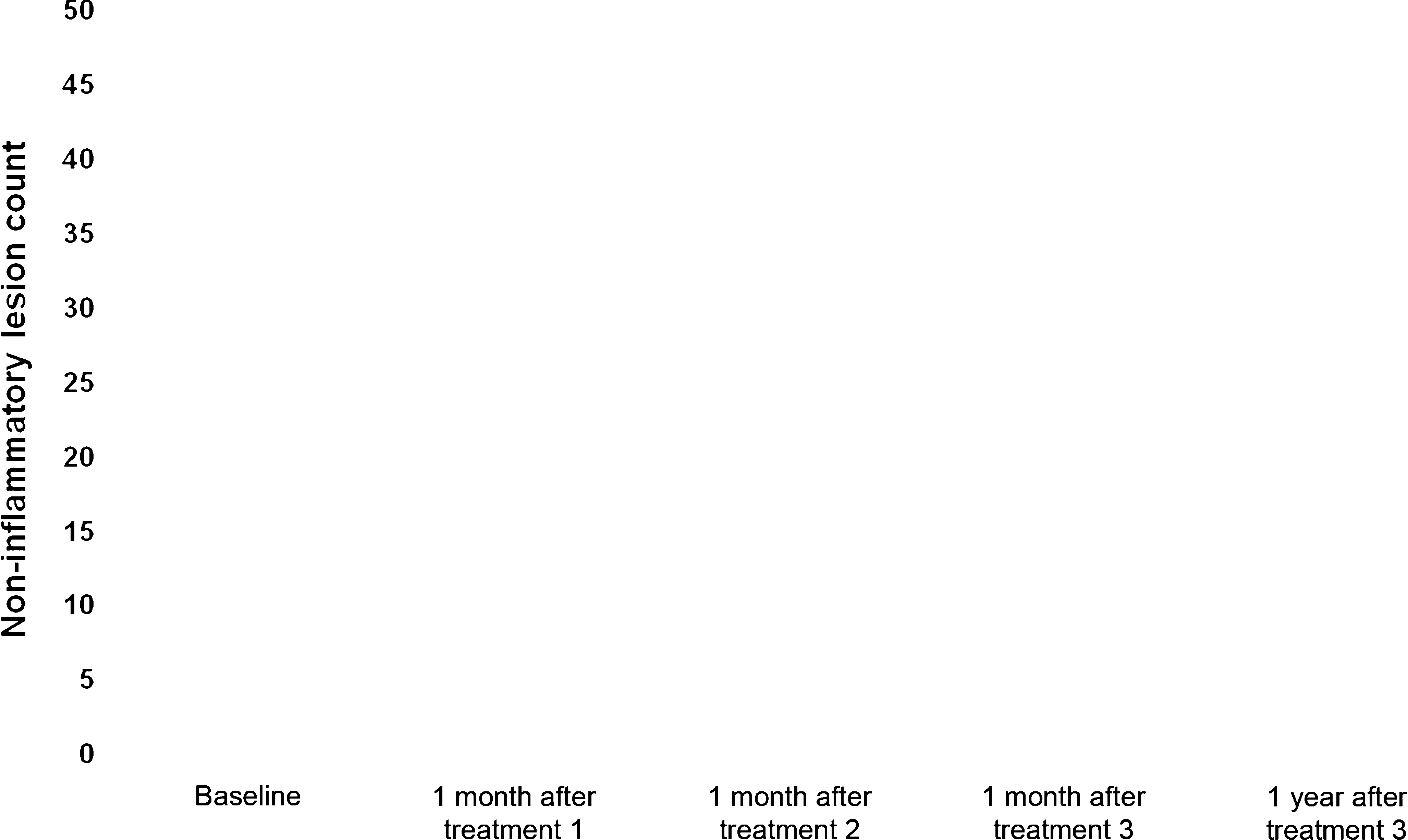
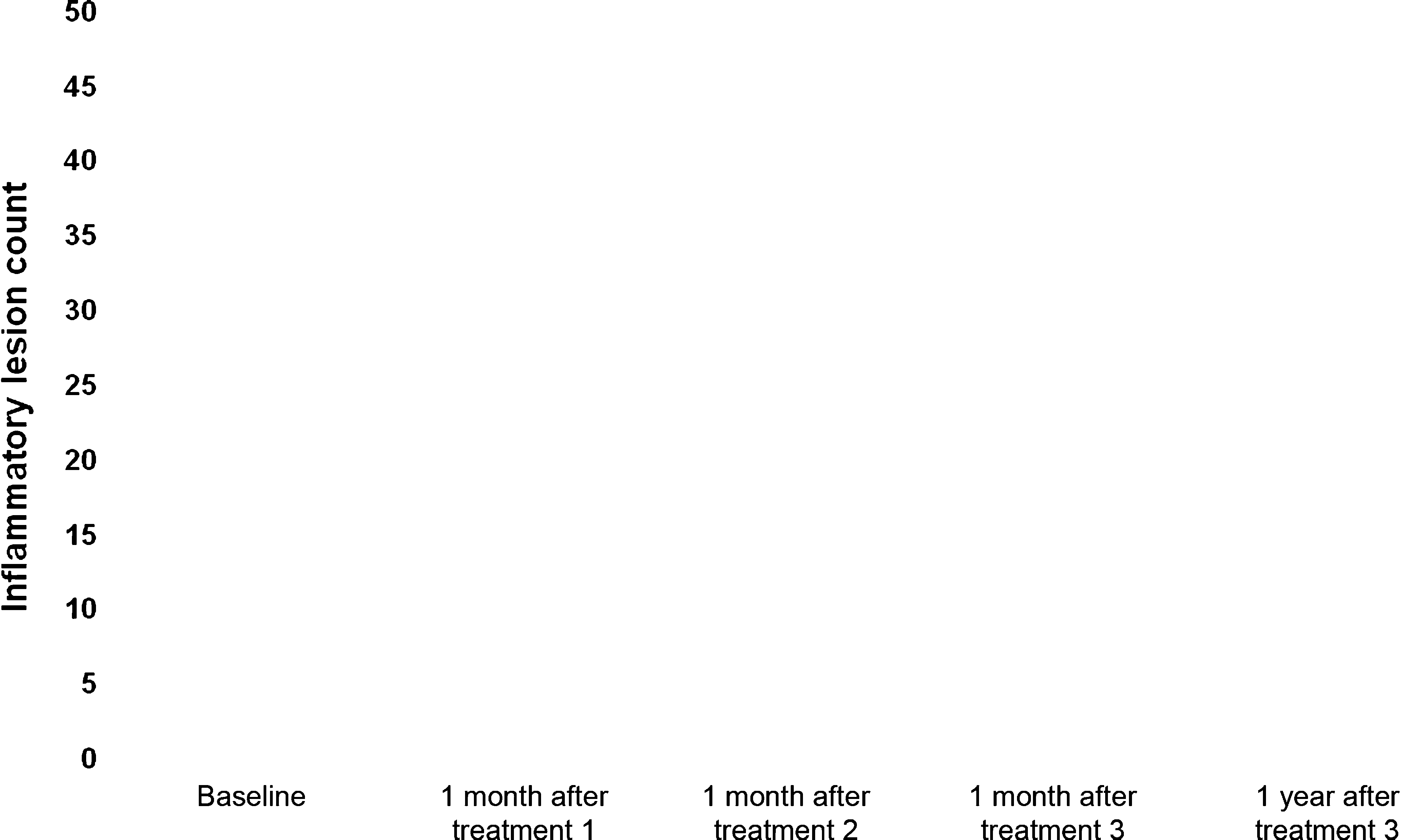
Figures 4 and 5 illustrate progressive changes in numbers
sessions (probably at least four or five sessions) will be
of inflammatory and non-inflammatory lesions from base-
required in very large cystic lesions to completely destroy
line. Of the 12 patients, one (8%) reported being ‘‘slightly
all associated sebaceous glands as most recurrences
satisfied’’ with the treatment, four (33%) reported being
occurred in the treatment zones of the largest acne
‘‘satisfied’’ and seven (59%) reported being ‘‘very satis-
lesions. We attribute our results to the permanent reduc-
fied.’’ The mean score for patient satisfaction was
tion in sebum excretion achieved by selective electro-
3.50 ± 0.67 (out of 4). The most common reported
thermolysis through the precise destruction of hyperactive
ª 2011 The International Society of Dermatology
International Journal of Dermatology 2011
Sebaceous gland electrothermolysis in acne
final treatment, and (d) at 1 year after
ment, (b) at 1 month after the first treat-
treatment, and (d) at 1 year after the last
sebaceous glands by electrical heat.3 Reducing the pro-
our study. This reliable, strong insulation permitted us to
duction of sebum, which is a medium for bacteria
use electrical power at a voltage sufficiently high to elimi-
growth, is helpful for normalizing Propionibacterium ac-
nate the target tissue without damaging the surface of the
nes hypercolonization. It is also possible that this inter-
vention-induced heat extended to the thermal destruction
Because this study is not a comparison study, it is
of bacteria.4 Moreover, the development of new technol-
impossible to directly compare the efficacy of this treat-
ogy, which allowed for very tight adhesion between the
ment with that of other treatments. However, selective
short, thin needle and insulating material, was critical to
electrothermolysis has some notable advantages over
International Journal of Dermatology 2011
ª 2011 The International Society of Dermatology
Sebaceous gland electrothermolysis in acne
other acne treatments. Most conventional topical agents
blue and red light sources.11–15 However, the therapeu-
– including antimicrobials, retinoids and anti-inflamma-
tic efficacy of these modalities is limited and relapse is
tory agents – must be applied daily for several weeks
common after these treatments are stopped. As selective
before any effect is seen, and most are associated with
electrothermolysis results in the permanent destruction
some degree of skin irritation.2,5–7 Similarly, many of
of treated sebaceous glands, it is associated with a low
the conventional oral medications used in treating acne
relapse rate. Additionally, this intervention achieves
– including antibiotics, oral contraceptives and retinoids
therapeutic efficacy in only two or three treatment ses-
– have significant portfolios of side-effects, including,
sions. Unlike photodynamic therapy, selective electro-
but not limited to, gastrointestinal upset, antibiotic
thermolysis does not require patients to avoid sun
resistance, thromboembolic events and teratogenicity.2,8–
exposure for 48 h after treatment and can be used in
By contrast, selective electrothermolysis performed by
properly trained therapists has not been associated with
In conclusion, our results suggest that selective electro-
any severe side-effects. As this method is not a systemic
thermolysis is clinically effective for the treatment of acne
treatment, many of the intrinsic problems associated
and that it is associated with minimal complications.
with the current acne regimens (e.g. patient compliance
Although few studies have fully described this treatment,
and associated side-effects) are not applicable. More
we contend that selective electrothermolysis represents
recently, optical treatments have been introduced as
another effective treatment modality that supports consis-
alternative treatments for acne, including pulsed dye
tent remission in acne. However, as this is a small study,
lasers (PDLs), infrared diode lasers, radiofrequency
additional, larger studies are needed to fully evaluate this
devices, intense pulsed light (IPL), and broad-spectrum
ª 2011 The International Society of Dermatology
International Journal of Dermatology 2011
Sebaceous gland electrothermolysis in acne
randomized, controlled multicenter study. Arch DermatolRes 2007; 299: 467–473.
The authors of this study would like to express their sin-
10 Eady EA, Gloor M, Leyden JJ. Propionibacterium acnes
cere condolences to the family of the late Dr Toshio Ko-
resistance: a worldwide problem. Dermatology 2003;
11 Seaton ED, Charakida A, Mouser PE, et al. Pulsed-dye
laser treatment for inflammatory acne vulgaris:
randomized controlled trial. Lancet 2003; 362: 1347–
1 Rivera AE. Acne scarring: a review and current treatment
modalities. J Am Acad Dermatol 2008; 59: 659–676.
12 Ruiz-Esparza J, Gomez JB. Non-ablasive radiofrequency
2 Thiboutot D, Gollnick H, Bettoli V, et al. New insights
for active acne vulgaris: the use of deep dermal heat in
into the management of acne: an update from the Global
the treatment of moderate to severe active acne vulgaris
Alliance to Improve Outcomes in Acne Group. J Am
(thermotherapy): a report of 22 patients. Dermatol Surg
Acad Dermatol 2009; 60(Suppl.): 1–50.
3 Kobayashi T, Tamada S. Selective electrothermolysis of
13 Ortiz A, Van Vliet M, Lask G, et al. A review of lasers
the sebaceous glands: treatment of facial seborrhea.
and light sources in the treatment of acne vulgaris.
J Cosmet Laser Ther 2005; 7: 69–75.
4 Lloyd JR, Mirkov M. Selective photothermolysis of the
14 Choi YS, Suh HS, Yoon MY, et al. Intense pulsed light
sebaceous glands for acne treatment. Lasers Surg Med
vs. pulsed-dye laser in the treatment of facial acne: a
randomized split-face trial. J Eur Acad Dermatol
5 Thiboutot D, Zaenglein A, Weiss J, et al. An aqueous gel
fixed combination of clindamycin phosphate 1.2% and
15 Haedersdal M, Togsverd-Bo K, Wulf HC. Evidence-based
benzoyl peroxide 2.5% for the once-daily treatment of
review of lasers, light sources and photodynamic therapy
moderate to severe acne vulgaris: assessment of efficacy
in the treatment of acne vulgaris. J Eur Acad Dermatol
and safety in 2813 patients. J Am Acad Dermatol 2008;
16 Hörfelt C, Funk J, Frohm-Nilsson M, et al. Topical
6 Gollnick HP, Draelos Z, Glenn MJ, et al. Adapalene-
methyl aminolaevulinate photodynamic therapy for
benzoyl peroxide, a unique fixed-dose combination
treatment of facial acne vulgaris: results of a randomized,
topical gel for the treatment of acne vulgaris: a
controlled study. Br J Dermatol 2006; 155: 608–613.
transatlantic, randomized, double-blind, controlled study
17 Haedersdal M, Togsverd-Bo K, Wiegell SR, et al. Long-
in 1670 patients. Br J Dermatol 2009; 161: 1180–1189.
pulsed dye laser versus long-pulsed dye laser-assisted
7 Rao GR, Ghosh S, Dhurat R, et al. Efficacy, safety, and
photodynamic therapy for acne vulgaris: a randomized
tolerability of microsphere adapalene vs. conventional
controlled trial. J Am Acad Dermatol 2008; 58:
adapalene for acne vulgaris. Int J Dermatol 2009; 48:
18 Oh SH, Ryu DJ, Han EC, et al. A comparative study of
8 Ellis CN, Krach KJ. Uses and complications of
topical 5-aminolevulinic acid incubation times in
isotretinoin therapy. J Am Acad Dermatol 2001; 45:
photodynamic therapy with intense pulsed light for the
treatment of inflammatory acne. Dermatol Surg 2009;
9 Akman A, Durusoy C, Senturk M, et al. Treatment of
acne with intermittent and conventional isotretinoin: a
International Journal of Dermatology 2011
ª 2011 The International Society of Dermatology
Uusi n sorkkaraportteihin on tulossa kolme uutta koodia: valkovi van paise, sorkkasyylä ja sorkkavälin li kakasvu. Nimet on muutettu kansankielisiksi, mutta ni den tarkoitus on antaa tarkempaa ja yksityiskohtaisempaa informaatiota ontumaa aiheuttavista valkovi van ongelmista ja toisaalta tarttuvista sorkkasairauksista. edustavat sekä syylää että ajotulehdusta ja ne pitää hoitaa antibi
Desert Explorer Tour di 15 giorni con accompagnatore locale parlante italiano 1° Italia/Windhoek Partenza con volo di linea Air Namibia per Windhoek. Pasti e pernottamento a bordo. 2° Windhoek Arrivo all’aeroporto di Windhoek e, dopo il disbrigo delle formalità doganali, trasferimento e sistemazione all’Hotel Safari Court. Resto della giornata a disposizione. Pernott
 Selective sebaceous gland electrothermolysis as a treatment
Jin W. Lee1, MD, Beom J. Kim1, MD, PhD, Myeung N. Kim1, MD, PhD, and
Although many therapeutic options exist for acne, relapse often occurs after treatment is
stopped. Some preliminary evidence suggests that selective electrothermolysis of the seba-
ceous glands may represent a novel therapeutic intervention. This trial was conducted to
evaluate the efficacy and tolerability of selective sebaceous gland electrothermolysis for the
treatment of facial acne. Twelve patients with facial acne were enrolled, all of whom under-
went three sessions of therapy. During each session, a 1.5-mm-long needle with 0.45-mm
of base insulation was inserted into pores of acne lesions. Upon insertion, a high-frequency
electrical current was applied for 0.25–0.50 s, for a total output of 40 W. Each treatment
session took approximately 30–60 min. Subject response to therapy was evaluated at
1 month and 12 months after the final treatment. All the enrolled subjects completed the
study and all reported satisfaction with treatment results. In all cases, a reduction in inflam-
matory and non-inflammatory lesion counts was observed after three sessions of selective
electrothermolysis, although a few small papules and comedones persisted in several
areas of untreated facial skin. Mean lesion reduction at 1 month after the final treatment
was 98.14% for inflammatory lesions and 83.09% for non-inflammatory lesions. Clinical
success was achieved in the majority of patients (seven of 12 patients) at 1 month after
the second treatment, and in all patients at 1 month after the final treatment. All patients
reported transient post-treatment erythema, which faded after a few days. Clinically evident
relapse occurred in two of 12 patients (16.7%) 1 year after the final treatment session.
Selective sebaceous gland electrothermolysis as a treatment
Jin W. Lee1, MD, Beom J. Kim1, MD, PhD, Myeung N. Kim1, MD, PhD, and
Although many therapeutic options exist for acne, relapse often occurs after treatment is
stopped. Some preliminary evidence suggests that selective electrothermolysis of the seba-
ceous glands may represent a novel therapeutic intervention. This trial was conducted to
evaluate the efficacy and tolerability of selective sebaceous gland electrothermolysis for the
treatment of facial acne. Twelve patients with facial acne were enrolled, all of whom under-
went three sessions of therapy. During each session, a 1.5-mm-long needle with 0.45-mm
of base insulation was inserted into pores of acne lesions. Upon insertion, a high-frequency
electrical current was applied for 0.25–0.50 s, for a total output of 40 W. Each treatment
session took approximately 30–60 min. Subject response to therapy was evaluated at
1 month and 12 months after the final treatment. All the enrolled subjects completed the
study and all reported satisfaction with treatment results. In all cases, a reduction in inflam-
matory and non-inflammatory lesion counts was observed after three sessions of selective
electrothermolysis, although a few small papules and comedones persisted in several
areas of untreated facial skin. Mean lesion reduction at 1 month after the final treatment
was 98.14% for inflammatory lesions and 83.09% for non-inflammatory lesions. Clinical
success was achieved in the majority of patients (seven of 12 patients) at 1 month after
the second treatment, and in all patients at 1 month after the final treatment. All patients
reported transient post-treatment erythema, which faded after a few days. Clinically evident
relapse occurred in two of 12 patients (16.7%) 1 year after the final treatment session. Sebaceous gland electrothermolysis in acne
side-effect was transient erythema at the sites of treated
lesions. The inflammatory content (pus) released by gentle
pressure spread to the surrounding tissue, inducing ery-
thema and further inflammation. Although this occurred
in all subjects, the redness typically faded within several
days and seldom persisted for a week. Other severe
adverse events – such as pigmentary alterations, scarring
and infections – were not reported. One year after the final
treatment, two of 12 patients (16.7%) were found to have
relapsed. However, in both cases, the acne was rated as
Lloyd and Mirkov4 first reported selective sebaceous
gland photothermolysis as an effective treatment for acne.
Sebaceous gland electrothermolysis in acne
side-effect was transient erythema at the sites of treated
lesions. The inflammatory content (pus) released by gentle
pressure spread to the surrounding tissue, inducing ery-
thema and further inflammation. Although this occurred
in all subjects, the redness typically faded within several
days and seldom persisted for a week. Other severe
adverse events – such as pigmentary alterations, scarring
and infections – were not reported. One year after the final
treatment, two of 12 patients (16.7%) were found to have
relapsed. However, in both cases, the acne was rated as
Lloyd and Mirkov4 first reported selective sebaceous
gland photothermolysis as an effective treatment for acne.
 Sebaceous gland electrothermolysis in acne
final treatment, and (d) at 1 year after
ment, (b) at 1 month after the first treat-
treatment, and (d) at 1 year after the last
sebaceous glands by electrical heat.3 Reducing the pro-
our study. This reliable, strong insulation permitted us to
duction of sebum, which is a medium for bacteria
use electrical power at a voltage sufficiently high to elimi-
growth, is helpful for normalizing Propionibacterium ac-
nate the target tissue without damaging the surface of the
nes hypercolonization. It is also possible that this inter-
vention-induced heat extended to the thermal destruction
Because this study is not a comparison study, it is
of bacteria.4 Moreover, the development of new technol-
impossible to directly compare the efficacy of this treat-
ogy, which allowed for very tight adhesion between the
ment with that of other treatments. However, selective
short, thin needle and insulating material, was critical to
electrothermolysis has some notable advantages over
International Journal of Dermatology 2011
ª 2011 The International Society of Dermatology
Sebaceous gland electrothermolysis in acne
final treatment, and (d) at 1 year after
ment, (b) at 1 month after the first treat-
treatment, and (d) at 1 year after the last
sebaceous glands by electrical heat.3 Reducing the pro-
our study. This reliable, strong insulation permitted us to
duction of sebum, which is a medium for bacteria
use electrical power at a voltage sufficiently high to elimi-
growth, is helpful for normalizing Propionibacterium ac-
nate the target tissue without damaging the surface of the
nes hypercolonization. It is also possible that this inter-
vention-induced heat extended to the thermal destruction
Because this study is not a comparison study, it is
of bacteria.4 Moreover, the development of new technol-
impossible to directly compare the efficacy of this treat-
ogy, which allowed for very tight adhesion between the
ment with that of other treatments. However, selective
short, thin needle and insulating material, was critical to
electrothermolysis has some notable advantages over
International Journal of Dermatology 2011
ª 2011 The International Society of Dermatology
 Sebaceous gland electrothermolysis in acne
other acne treatments. Most conventional topical agents
blue and red light sources.11–15 However, the therapeu-
– including antimicrobials, retinoids and anti-inflamma-
tic efficacy of these modalities is limited and relapse is
tory agents – must be applied daily for several weeks
common after these treatments are stopped. As selective
before any effect is seen, and most are associated with
electrothermolysis results in the permanent destruction
some degree of skin irritation.2,5–7 Similarly, many of
of treated sebaceous glands, it is associated with a low
the conventional oral medications used in treating acne
relapse rate. Additionally, this intervention achieves
– including antibiotics, oral contraceptives and retinoids
therapeutic efficacy in only two or three treatment ses-
– have significant portfolios of side-effects, including,
sions. Unlike photodynamic therapy, selective electro-
but not limited to, gastrointestinal upset, antibiotic
thermolysis does not require patients to avoid sun
resistance, thromboembolic events and teratogenicity.2,8–
exposure for 48 h after treatment and can be used in
By contrast, selective electrothermolysis performed by
properly trained therapists has not been associated with
In conclusion, our results suggest that selective electro-
any severe side-effects. As this method is not a systemic
thermolysis is clinically effective for the treatment of acne
treatment, many of the intrinsic problems associated
and that it is associated with minimal complications.
Sebaceous gland electrothermolysis in acne
other acne treatments. Most conventional topical agents
blue and red light sources.11–15 However, the therapeu-
– including antimicrobials, retinoids and anti-inflamma-
tic efficacy of these modalities is limited and relapse is
tory agents – must be applied daily for several weeks
common after these treatments are stopped. As selective
before any effect is seen, and most are associated with
electrothermolysis results in the permanent destruction
some degree of skin irritation.2,5–7 Similarly, many of
of treated sebaceous glands, it is associated with a low
the conventional oral medications used in treating acne
relapse rate. Additionally, this intervention achieves
– including antibiotics, oral contraceptives and retinoids
therapeutic efficacy in only two or three treatment ses-
– have significant portfolios of side-effects, including,
sions. Unlike photodynamic therapy, selective electro-
but not limited to, gastrointestinal upset, antibiotic
thermolysis does not require patients to avoid sun
resistance, thromboembolic events and teratogenicity.2,8–
exposure for 48 h after treatment and can be used in
By contrast, selective electrothermolysis performed by
properly trained therapists has not been associated with
In conclusion, our results suggest that selective electro-
any severe side-effects. As this method is not a systemic
thermolysis is clinically effective for the treatment of acne
treatment, many of the intrinsic problems associated
and that it is associated with minimal complications.