Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Commonweb.unifr.ch
Journal of Consulting and Clinical Psychology
Copyright 2003 by the American Psychological Association, Inc.
Cognitive Therapy Versus Fluoxetine in Generalized Social Phobia:
David M. Clark, Anke Ehlers, and Freda McManus
Ann Hackmann, Melanie Fennell, Helen Campbell,
Teresa Flower, Clare Davenport, and Beverley Louis
Sixty patients meeting Diagnostic and Statistical Manual of Mental Disorders (4th ed.; AmericanPsychiatric Association, 1994) criteria for generalized social phobia were assigned to cognitive therapy(CT), fluoxetine plus self-exposure (FLU ϩ SE), or placebo plus self-exposure (PLA ϩ SE). Atposttreatment (16 weeks), the medication blind was broken. CT and FLU ϩ SE patients then entered a3-month booster phase. Assessments were at pretreatment, midtreatment, posttreatment, end of boosterphase, and 12-month follow-up. Significant improvements were observed on most measures in all 3treatments. On measures of social phobia, CT was superior to FLU ϩ SE and PLA ϩ SE at midtreatmentand at posttreatment. FLU ϩ SE and PLA ϩ SE did not differ. CT remained superior to FLU ϩ SE atthe end of the booster period and at 12-month follow-up. On general mood measures, there were fewdifferences between the treatments.
Social phobia is a common and disabling disorder (Magee, Eaton,
azepines, monoamine oxidase inhibitors, and selective serotonin
Wittchen, Gonagle, & Kessler, 1996) that is associated with marked
reuptake inhibitors (SSRIs). In several countries concerns about
vocational underachievement and an increased risk of depression,
dependency have led to the recommendation that benzodiazepines
suicide, and alcohol abuse (Heckelman & Schneier, 1995; Rapee,
should only be used for brief periods (e.g., Committee on Safety of
1995). Onset is typically in adolescence or earlier (Rapee, 1995).
Medicines, 1988), which limits their utility in treating a chronic
Perhaps because many patients see the disorder as part of their
condition such as social phobia. Phenelzine is the best validated
personality, treatment-seeking rates are low in comparison with other
monoamine oxidase inhibitor. Three controlled trials (Heimberg et
anxiety disorders, such as panic disorder (Fresco, Erwin, Heimberg, &
al., 1998; Liebowitz et al., 1992; Versiani et al., 1992) have found
Turk, 2000; Magee et al., 1996). However, in the past 15 years
phenelzine superior to placebo. A fourth trial (Gelernter et al.,
considerable progress has been made in developing effective pharma-
1991) failed to find a significant difference between phenelzine
cological and psychological treatments.
and placebo on the main social phobia measures but did find a
Within pharmacological approaches (see Hood & Nutt, 2001,
difference on a secondary measure of work and social disability.
for a review), the three best validated interventions are benzodi-
Among the SSRIs, controlled trials have established superiorityover placebo medication for fluvoxamine (Stein, Fyer, Davidson,Pollack, & Wiita, 1999), sertraline (Blomhoff et al., 2001; Van
David M. Clark, Anke Ehlers, and Freda McManus, Department of
Ameringen, Swinson, Walker, & Lane, 1999; Van Ameringen et
Psychology, Institute of Psychiatry, London, United Kingdom; Ann Hack-
al., 2001), and paroxetine (Allgulander, 1999; Baldwin, Bobes,
mann, Melanie Fennell, Helen Campbell, Teresa Flower, Clare Davenport,and Beverley Louis, Department of Psychiatry, University of Oxford,
Stein, Scharwa¨chter, & Faure, 1999; Stein et al., 1998).
Within psychological approaches, the best validated treatments
Freda McManus is now at Isis Education Centre, Warneford Hospital,
are behavioral and cognitive– behavioral. Five meta-analytic re-
Oxford, United Kingdom. Helen Campbell is now at the Berkshire Health-
views (Chambless & Hope, 1996; Fedoroff & Taylor, 2001; Feske
care National Health Service Trust, Reading, United Kingdom; Teresa
& Chambless, 1995; Gould, Buckminster, Pollack, Otto, & Yap,
Flower is now at the Adolescent Forensic Health Service, Parkville, Vic-
1997; Taylor, 1996) have summarized studies comparing behav-
toria, Australia; Clare Davenport is now at the Department of Public Health
ioral and cognitive– behavioral treatments (CBTs) with various
and Epidemiology, University of Birmingham, Birmingham, United King-
control conditions, and each reached broadly similar conclusions.
dom; Beverley Louis is now at the Central Middlesex Hospital, London,United Kingdom.
Exposure alone and exposure with cognitive restructuring are both
The research was funded by the Wellcome Trust. Anke Ehlers is a
associated with significantly greater effect sizes than are waiting
Wellcome Principal Research Fellow. Eli Lilly provided the identically
list control conditions. Individual studies have failed to provide
packaged 20-mg capsules of fluoxetine and placebo. We are grateful to
convincing evidence of a difference in efficacy between exposure
Hester Barrington-Ward, Katie Bradbury, Jessica Bolton, Philip Cowen,
alone and exposure with cognitive restructuring. However, in one
Christopher Fairburn, Carolyn Fordham, Michael Gelder, Antje Ho˝rst, and
meta-analysis (Taylor, 1996), only the combination of exposure
and cognitive restructuring was superior to placebo control condi-
Correspondence concerning this article should be addressed to David M.
tions. A particularly encouraging finding has been the excellent
Clark, Department of Psychology, PO Box 77, Institute of Psychiatry, DeCrespigny
maintenance of gains after the end of effective psychological
treatment. For example, Heimberg, Salzman, Holt, and Blendell
(1993) found that patients who received cognitive– behavioral
with a simple practical procedure such as self-exposure. To esti-
group treatment (CBGT) retained their gains at 5-year follow-up
mate the extent to which improvements associated with fluoxetine
and remained significantly less symptomatic than patients who had
plus self-exposure were active pharmacological effects, we also
received a control treatment (education-support).
included a placebo plus self-exposure condition in the study.
Despite the positive findings reported for existing behavioral
and cognitive– behavioral treatments, it is generally agreed that
there is scope for further development. First, a significant subset ofpatients fail to achieve optimal benefit from the existing treatment
programs. For example, in an intent-to-treat analysis, Heimberg etal. (1998) reported that fewer than 60% of patients who received
Patients were initially randomly assigned to CT, fluoxetine plus self-
CBGT were classified as treatment responders. Using a stricter
exposure (FLU ϩ SE), or placebo plus self-exposure (PLA ϩ SE). Allo-cation to fluoxetine or placebo was double-blind. Patients had up to 16
improvement criterion, Mattick and Peters (1988) reported that
weekly treatment sessions. After 16 weeks, the medication blind was
only 38% of patients who completed their cognitive– behavioral
broken. Patients who were allocated to FLU ϩ SE continued their medi-
program were considered optimally improved (achieved high end-
cation for 3 months and had up to three treatment sessions during this
state functioning). Second, one recent meta-analytic review (Fe-
booster period. Patients who were allocated to CT had the same number of
doroff & Taylor, 2001) has concluded that pharmacotherapies
booster sessions. Patients initially allocated to placebo were withdrawn
(particularly SSRIs) yield the largest initial effect sizes in social
from the trial at 16 weeks and offered their choice of CT, FLU ϩ SE, or
phobia, although there is some evidence for greater relapse after
a combination of both treatments. Assessments, which included ratings
discontinuation of medication than after termination of CBT
completed by an independent assessor, were at pretreatment, midtreatment,
posttreatment (16 weeks), end of the booster period, and 12-month
The present study reports a randomized controlled trial that
evaluated a new CBT and compared it with treatment with anSSRI. The new CBT is the cognitive therapy (CT) program de-
veloped by Clark, Wells, and colleagues on the basis of their
Local general practitioners, psychiatrists, and psychologists were sent a
cognitive model of social phobia. Clark and Wells’s (1995) cog-
letter requesting referrals to a trial of psychological and pharmacological
nitive model, which is very similar to the model described by
treatments for social phobia. Advertisements in the local press and shop-
Rapee and Heimberg (1997), is largely focused on the maintenance
ping centers also brought the trial to the attention of potential participants
of social phobia and attempts to explain why patients with social
(all of whom had to be referred by a clinician). Referrers were informed
phobia fail to benefit from the naturalistic exposure that is pro-
that open trials suggested that CT and fluoxetine were both effective, and
vided by their everyday interactions with other people. Four main-
it was not known which was more effective. Referred patients were
tenance processes are particularly highlighted. The maintenance
assessed using a combination of the Anxiety Disorders Interview Schedule
processes are (a) an increase in self-focused attention and moni-
for DSM–IV (ADIS; Brown, Di Nardo, & Barlow, 1994) and the Structured
toring with a linked reduction in observation of other people and
Clinical Interview for DSM–IV, Axis-I disorders (SCID-I; First, Spitzer,
their responses; (b) the use of misleading internal information
Gibbon, & Williams, 1995). All patients were assessed with the overviewmodule of the SCID-I and the social phobia module of the ADIS. If the
(particularly anxious feelings and spontaneously occurring, dis-
SCID-I screener module indicated that another Axis-I disorder might be
torted images of themselves seen from an observer perspective) to
present, the SCID-I module for that disorder was also administered. All
make excessively negative inferences about how one appears to
patients were also assessed with the Avoidant Personality Disorder section
others; (c) extensive use of safety behaviors that are intended to
of the SCID: Axis-II Disorders Interview (SCID-II; First, Gibbon, Spitzer,
prevent feared catastrophes but have the consequence of maintain-
Williams, & Benjamin, 1997). The Borderline Personality Disorder section
ing negative beliefs, increasing feared symptoms, and making
of SCID-II was administered if it was clinically relevant. Diagnostic
patients come across to others in ways that are likely to elicit less
interviews were conducted by clinical psychologists who had received
friendly responses (although termed behaviors, a substantial pro-
extensive training in the SCID and ADIS. All diagnoses were also checked
portion of the safety behaviors are cognitive strategies); and (d) the
with a senior clinician (David M. Clark). Patients were accepted if they met
use of negatively biased anticipatory and postevent processing.
the following criteria: (a) Diagnostic and Statistical Manual of MentalDisorders (4th ed.; DSM–IV; American Psychiatric Association, 1994)
The CT program includes a series of procedures that are specifi-
criteria for generalized social phobia;1 (b) condition duration of at least 6
cally focused on reversing the maintaining processes specified in
months; (c) social phobia was considered their main problem; (d) age
between 18 and 60 years; (e) willingness to accept random allocation; (f)
The SSRI chosen for comparison with CT is fluoxetine. At the
no current major depressive disorder, bipolar disorder, psychosis, alcohol
time the trial was conducted, no controlled trials of fluoxetine had
or substance dependency, or epilepsy; (g) not pregnant and had no intention
been reported. However, five open trials of fluoxetine (Black,
to become pregnant; (h) social phobia had not been previously treated with
Uhde, & Tancer, 1992; Koponen, Lepola, & Juhani, 1995; Perugi
an SSRI, CT, or exposure therapy; (i) no psychotropic medication use or,
et al., 1994; Schneier, Chin, Hollander, & Liebowitz, 1992; VanAmeringen, Mancini, & Streiner, 1993) had obtained promising
results. Following the example of two previous pharmacotherapy
Following the DSM–IV (American Psychiatric Association, 1994, pp.
412– 413), we diagnosed the generalized subtype of social phobia if the
trials in social phobia (Blomhoff et al., 2001, with sertraline;
assessors considered that an individual’s fears “related to most social
Gelernter et al., 1991, with phenelzine), fluoxetine was combined
situations” and involved fear of “both public performance situations and
with weekly self-exposure assignments. Combining medication
social interaction situations.” Inspection of patients’ pretreatment Liebow-
with self-exposure was intended to produce a closer approximation
itz Social Anxiety Scales (LSAS; Liebowitz, 1987) indicated that accepted
to routine clinical practice, as it was thought that many United
patients feared a median of 20 of the 24 situations specified on the scale
Kingdom clinicians who use medication are likely to combine it
alternatively, willingness to be withdrawn from medication before the start
trial, patients were informed that they might be asked to provide a blood
of the trial (a minimum 4-week drug-free period was required before a
sample without advance warning during one of their treatment sessions.
patient could start trial treatment); and (j) agreed not to start any additional
Blood was taken from 16 patients (80%) in each group during a session
treatment during the trial. With the exception of borderline personality
between Weeks 9 and 13. An independent laboratory, blind to allocation,
disorder, Axis II personality disorders were not a reason for exclusion.
assayed for fluoxetine and norfluoxetine levels. After the blind was broken,
Of 123 social phobia patients referred for possible inclusion in the trial,
the assays indicated that no patients allocated to placebo had fluoxetine or
63 did not meet entry criteria. Reasons for exclusion were as follows: social
its metabolite in their blood. All patients allocated to fluoxetine had
phobia was not the main problem (19 patients); participation was declined
significant blood levels of fluoxetine (M ϭ 331.5 g/ml, SD ϭ 149.1
(14 patients); previous treatment with an SSRI (9 patients); social phobia
g/ml) and norfluoxetine (M ϭ 217.7 g/ml, SD ϭ 89.8 g/ml). Prior to
was too mild or too specific (8 patients); use of medication with psycho-
starting medication, patients were told that there is good reason to believe
tropic effects that would be medically inappropriate to withdraw (6 pa-
that social phobia is maintained by a neurochemical disturbance that can be
tients); previous CBT for social phobia (3 patients); current major depres-
rectified by fluoxetine. They were told that as the dose built up, fluoxetine
sive disorder (3 patients); and borderline personality disorder (1 patient).
should help make them more confident in social situations but that to gain
The remaining 60 patients met entry criteria and were allocated to treat-
the maximum benefit from the medication they would also need to sys-
ment (20 per condition) on a stratified random basis. Stratification vari-
tematically expose themselves to feared social situations, with exposure
ables were gender (male, female) and avoidant personality disorder
being organized in a graded way to progressively build self-confidence.
(present, absent). Within each of the stratification cells, sealed allocations
From Session 3 onward, therapists set several new exposure assignments
each week and reviewed the assignments during the next session. Therewere no therapist-accompanied or in-session exposure assignments. Ses-
sions typically lasted 30 – 40 min.
CT was based on Clark and Wells’s (1995) model of the mainte-
nance of social phobia and used a variety of procedures to reverse themaintaining factors identified in the model. The procedures were described
CT was delivered by four clinical psychologists who were experienced
in detail in a therapist manual (Clark, 1997) and can also be found in briefer
in the use of CBTs for anxiety. The medication plus self-exposure treat-
form in Wells (1997, Chapter 7) and Clark (2001, pp. 419 – 427). The main
ments were delivered by four specialist registrars in psychiatry with several
steps in treatment were as follow: (a) developing with patients a personal
years of out-patient practice with a mixed caseload that included anxiety
version of Clark and Wells’s model using their own thoughts, images,
disorders. As do many pharmacotherapists, the psychiatrists had extensive
anxiety symptoms, safety behaviors, and attentional strategies; (b) safety
prior experience with SSRIs but only modest formal training in CBT. All
behaviors and self-focused attention experiment: Key safety behaviors
therapists treated at least two practice social phobia cases in the relevant
were identified and their adverse effects demonstrated with an experiential
treatment modality (CT or medication ϩ SE) before the start of the trial.
exercise in which patients role-played a difficult social situation while
During the trial, all therapists had regular supervision with David M. Clark
focusing attention on themselves and using their safety behaviors and then
to check protocol adherence and assist with planning future sessions. A
while focusing attention externally and attempting to drop their safety
random selection of session tapes was also reviewed. In the medication
behaviors; (c) shifting focus of attention to the social situation: Patients
conditions, additional supervision from a senior psychiatrist was provided.
were encouraged to focus their attention externally to reduce problematic
No protocol violations were detected.
self-monitoring and to obtain more accurate information about how theyare responded to by other people; (d) video feedback was used to modify
distorted self-imagery: Patients viewed a video of the safety behaviors andattention experiment and videos of other occasions in which they engaged
Social phobia. Independent assessors rated patients’ fear and avoid-
in feared social tasks under an instructional set that was designed to make
ance across a range of social situations using the ADIS. The mean rating
the discrepancy between patients’ negative, distorted self-images and their
across all fear and avoidance items was analyzed. Patients completed five
objective social performance particularly evident (see Harvey, Clark,
standardized self-report social phobia scales: Mattick and Clarke’s (1998)
Ehlers, & Rapee, 2000, for a description and evaluation of this procedure);
Social Phobia Scale and Social Interaction Anxiety Scale; the LSAS;
(e) behavioral experiments: Extensive use was made of behavioral exper-
Marks and Mathews’s (1979) Fear Questionnaire Social Phobia subscale
iments in which patients specified their feared outcomes for various social
(FQ-SOC); and the Fear of Negative Evaluation Scale (Watson & Friend,
situations and tested out whether they occurred during planned exposure to
1969). To date, the LSAS has most commonly been used as an assessor
the situations using in-session role-plays and in-session and homework-
rating. However, Baker, Heinrichs, Kim, and Hofman (2002) have recently
based in vivo assignments. To maximize disconfirmation, patients were
provided data that support its use as a self-report instrument. An additional
encouraged to drop safety behaviors and focus their attention externally.
self-report measure, the Social Phobia Weekly Summary Scale (SPWSS),
“Widening bandwidth” exercises in which patients intentionally acted
which was developed by our group, was also included. The five-item
against their excessively rigid rules for social interaction while observing
SPWSS has good internal consistency (Cronbach’s ␣ ϭ .81) and consists
the consequences were included; (f) problematic anticipatory and
of 0 – 8 ratings of social anxiety, social avoidance, self-focused versus
postevent processing was identified: Discussion usually showed that the
external attention, anticipatory processing, and postevent rumination.
disadvantages of anticipatory and postevent processing greatly exceeded its
General mood. The Beck Anxiety Inventory (BAI; Beck, Epstein,
advantages and, armed with this knowledge, patients were encouraged to
Brown, & Steer, 1988) and the Beck Depression Inventory (BDI; Beck,
drop it; and (g) dysfunctional assumptions were also identified and mod-
Rush, Shaw, & Emery, 1979) were used to assess anxious and depressed
ified by behavioral experiments and by cognitive restructuring techniques.
All social phobia and general mood measures were given at each
Medication and self-exposure (FLU ϩ SE and PLA ϩ SE).
assessment except for the midtreatment assessment, when the ADIS (as-
who were allocated to medication and self-exposure instructions were
sessor rating) and the LSAS (patient self-report) were omitted.
started on identically packaged 20-mg capsules of either fluoxetine orplacebo. Dose was increased to 40 mg in Week 2 or 3. A maximum dose
of 60 mg was permitted. All but 1 patient in each group received themaximum dose (usually by Week 5 or 6). The remaining 2 patients reached
Analyses were intent to treat. All patients who started treatment and
40 mg (FLUϩ SE) and 20 mg (PLA ϩ SE), respectively. At the start of the
provided at least one postintake assessment were included in the analyses
with last available data carried forward, with the exception of the 12-monthfollow-up analysis, in which data for patients who failed to reach theposttreatment assessment were not carried forward.2 To identify any dif-ferences between groups before treatment, we compared initial scores forthe three treatment groups with the liberal procedure of separate one-wayanalyses of variance (ANOVAs) for each measure. To identify any differ-ences between groups at midtreatment, posttreatment or follow-up, weused one-way analyses of covariance (ANCOVAs) with pretreatmentscores as covariates followed by post hoc Duncan’s multiple range testswhen comparing more than two means. We used t tests to identify signif-icant within-treatment changes. A two-step approach was adopted to dealwith multiple measurement of social phobia. First, a single unweightedsocial phobia composite was created and analyzed. Only if the compositerevealed significant between- or within-group differences were furtherANCOVAs or t tests performed on individual social phobia measures. Thecomposite was generated with the procedure recommended by Rosenthal
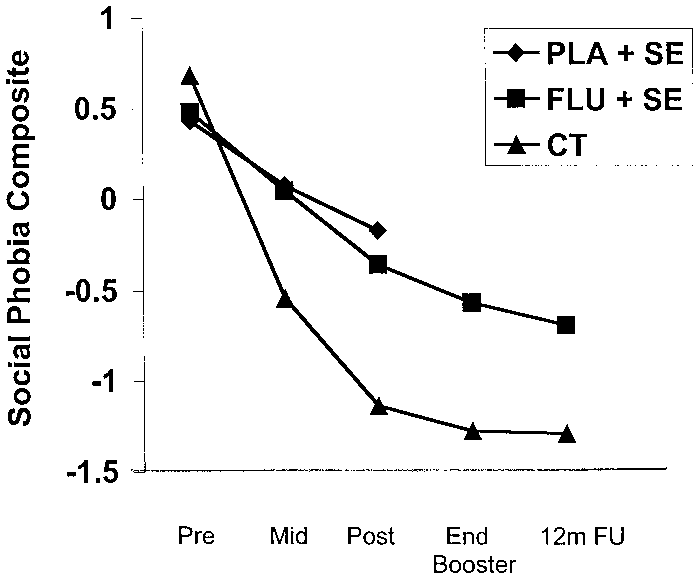
Social phobia composite scores at each assessment. CT ϭ
and Rosnow (1991) and adopted in several previous trials (e.g., Clark et al.,
cognitive therapy; FLU ϩ SE ϭ fluoxetine plus self-exposure; PLA ϩ
1994, 1999; Hollon et al., 1992). Patients’ scores on each (of seven) social
SE ϭ placebo plus self-exposure; pre ϭ pretreatment, mid ϭ midtreat-
phobia measures were standardized (M ϭ 0, SD ϭ 1) across pre- and
ment; post ϭ posttreatment; 12m FU ϭ 12-month follow-up.
posttreatment assessments by converting to Z scores. The composite ateach assessment occasion was the mean of the Z scores on that occasion.
which five individual measures were administered. At pretreat-ment, one-way ANOVAs indicated that there were no significant
At midtreatment (8 weeks), ANCOVA revealed a significant
treatment effect on the social phobia composite. Paired compari-
Patients’ mean age was 33.2 years (SD ϭ 8.1). Mean duration of
sons indicated that CT was superior to FLU ϩ SE and PLA ϩ SE,
social phobia was 13.3 years (SD ϭ 11.3). Fifty-two percent were
which did not differ from each other. Analysis of the five individ-
women. Fifty percent were married or cohabiting. Seventy-two
ual social phobia measures indicated that CT was superior to
percent were employed, 12% were students, and 16% were unem-
FLU ϩ SE on two measures and superior to PLA ϩ SE on three
ployed. Thirty-three percent left school by age 16, 11% completed
measures. Within-group t tests were used to assess pretreatment to
high school, and 56% had some higher education. Forty-three
midtreatment change. All three treatments were associated with
percent met criteria for avoidant personality disorder. Fourteen
significant pretreatment to midtreatment improvement on the so-
percent were taking psychotropic medication from which they had
cial phobia composite and most individual measures. The mea-
to be withdrawn before the start of the trial. There were no
sures that were not significant were the Fear of Negative Evalua-
significant differences between the treatment groups in any of
tion Scale in the FLU ϩ SE condition and FQ-SOC and SPWSS in
At posttreatment (16 weeks), there were significant ANCOVA
Dropouts and Number of Sessions Attended
treatment effects on the social phobia composite and all sevenindividual measures. Paired comparisons indicated that CT was
Four patients withdrew before the end of treatment: 2 because of
superior to FLU ϩ SE and PLA ϩ SE on each measure. FLU ϩ
side-effects (1 in FLU ϩ SE, 1 in PLA ϩ SE), 1 (PLA ϩ SE) to
SE did not differ from PLA ϩ SE.3 The t tests indicated that the
seek treatment elsewhere, and 1 (PLA ϩ SE) relocated for work.
CT and FLU ϩ SE conditions were associated with significant
Two further patients (both FLU ϩ SE) were withdrawn. One
pretreatment to posttreatment improvement on the social phobia
unexpectedly became pregnant, and the other became severely
composite and all individual measures. PLA ϩ SE was associated
depressed and required additional emergency treatment. For these
with significant pretreatment to posttreatment improvement on all
patients, assessments at the point of withdrawal (Weeks 6, 3, 5, 9,
7, & 12, respectively) were used in the posttreatment and end-of-booster-period analyses. Patients were offered up to 16 treatmentsessions and 3 booster sessions. For completers, the mean numbers
2 The main reason for the 12-month follow-up was to determine whether
of sessions attended were CT, 15.1 (SD ϭ 1.7) treatment sessions
treatment gains were maintained. In this context, we considered carrying
and 2.5 (SD ϭ 0.9) booster sessions; FLU ϩ SE, 13.5 (SD ϭ 1.8)
forward the last observation for patients who did not attend the 12-month
treatment sessions and 2.7 (SD ϭ 0.9) booster sessions; and
follow-up problematic, as it assumes that such individuals did not relapse. As a consequence, the extent to which treatment gains were maintained
PLA ϩ SE, 13.2 (SD ϭ 2.8) treatment sessions. For dropouts, the
could be overestimated. At the request of an anonymous reviewer, a
mean numbers of treatment sessions attended were FLU ϩ SE, 6.7
reanalysis of the 12-month follow-up data using the carried forward strat-
(SD ϭ 3.8) and PLA ϩ SE, 5.7 (SD ϭ 2.5).
egy was also conducted. The results were essentially the same as thosereported in the text. CT remained superior to FLU ϩ SE on the social
Effects of Treatment on Social Phobia
phobia composite, but the number of individual social phobia measures thatshowed a significant difference between the two treatments increased from
Figure 1 shows the social phobia composite, and Table 1 shows
four to six. The additional measures were the ADIS and LSAS.
the individual social phobia measures at each time point. The
3 A completers-only analysis in which the patients who had less than 16
social phobia composite was based on seven individual social
weeks on medication were excluded produced essentially similar results,
phobia measures at all time points except for midtreatment, at
with FLU ϩ SE and PLA ϩ SE failing to differ on any measure.
Table 1Outcome Measures at Each Assessment
Within an assessment occasion, means with no subscripts and those that share the same subscript do not differ. Means with nonoverlapping
subscripts differ at p Ͻ .05 or better. a Two fluoxetine and self-exposure patients restarted fluoxetine between the end of the booster period and the 12-month follow-up. Patients were asked torefrain from seeking any additional nontrial treatment during the follow-up period. No cognitive therapy patient had additional trial or nontrial treatment. Two fluoxetine and self-exposure patients started a course of psychological treatment between the end of the booster period and the 12-month follow-up. Both had a full assessment, data from which were used for the 12-month follow-up analysis, before starting the additional treatment. b At pretreatment, group effect was based on one-way analysis of variance. At all other assessment points group effect was based on one-way analysis ofcovariance, with pretreatment scores as the covariate. Significant ( p Ͻ .01) analysis of variance or analysis of covariance main effects were investigatedwith post hoc Duncan’s multiple range tests when more than two means were involved. † p Ͻ .1.
* p Ͻ .05. ** p Ͻ .01. Effects of Treatment on General Mood
phobia measures. For both treatments, t tests comparing 12-monthfollow-up scores with patients’ scores at posttreatment and at the
In contrast to the social phobia measures, ANCOVAs indicated
end of the booster phase were all nonsignificant, indicating that the
that the three treatments did not differ in their effects on the
treatment gains were maintained at 12-month follow-up, but there
general mood measures (BAI and BDI) at either midtreatment or
was no evidence of further, sustained improvement. For the gen-
posttreatment (see Table 1). However, in all three treatments there
eral mood measures, CT was superior to FLU ϩ SE on the BAI but
were significant pretreatment to midtreatment and pretreatment to
posttreatment improvements on the BAI and the BDI (all ps Ͻ.05).
To gain a clearer impression of the magnitude of the improve-
ment in social phobia associated with each treatment condition, we
At 16 weeks the medication blind was broken and patients on
calculated uncontrolled pretreatment to posttreatment, end of
placebo were withdrawn from the trial. Patients who had received
booster, and follow-up effect sizes for the social phobia composite
CT or FLU ϩ SE entered a 3-month booster phase during which
using the following formula: Effect size ϭ (mean social phobia
they received up to three additional sessions. Fluoxetine was
composite at pretreatment – mean social phobia composite at
maintained at full dose in the booster phase. At the end of the
posttreatment, end of booster, or follow-up) Ϭ pooled standard
booster phase, no further treatment sessions were offered and
deviation. Table 2 shows the data. Depending on the assessment
fluoxetine was gradually withdrawn over a 3- to 6-week period.
point, uncontrolled effect sizes ranged from 2.14 to 2.53 for CT
and from 0.92 to 1.36 for FLU ϩ SE. Controlled effect sizes in
ANCOVA indicated that CT was superior to FLU ϩ SE on the
which the posttreatment means for CT and FLU ϩ SE were
social phobia composite and four of seven individual social phobia
compared with PLA ϩ SE were also computed using the following
measures (see Table 1). The t tests comparing posttreatment and
formula: Controlled effect size ϭ (PLA ϩ SE posttreatment co-
end of booster phase scores were used to determine whether
variance adjusted mean Ϫ CT or FLU ϩ SE posttreatment
treatment gains were maintained or improved on in the boosterperiod. For CT none were significant, indicating that treatmentgains were maintained. For FLU ϩ SE significant improvement
was observed in the social phobia composite, t(19) ϭ 3.02, p Ͻ
Effect Sizes for the Social Phobia Composite at Posttreatment,
0.1; the ADIS, t(18) ϭ 3.02, p Ͻ .01; the FQ-SOC, t(17) ϭ 2.68,
End of Booster Period, and 12-Month Follow-Upp Ͻ .05; and the Social Interaction Anxiety Scale, t(18) ϭ 3.66,p Ͻ .001. For the general mood measures, ANCOVA indicated
that CT did not differ from FLU ϩ SE. The t tests comparing
posttreatment and end of booster scores were nonsignificant, in-
dicating that for both CT and FLU ϩ SE treatment gains in general
Note. CT ϭ cognitive therapy; FLU ϩ SE ϭ fluoxetine plus self-
exposure; PLA ϩ SE ϭ placebo plus self-exposure. Effect size ϭ (mean
ANCOVA indicated that CT remained superior to FLU ϩ SE on
composite at pretreatment minus mean composite at posttreatment, end of
the social phobia composite and four of seven individual social
booster or at follow-up) Ϭ pooled standard deviation.
covariance-adjusted mean) Ϭ pooled standard deviation. Cohen
several of the procedures involved in the CT program (dropping
(1988) proposed a threefold classification of effect sizes: small
safety behaviors, shifting to an external focus of attention, and
(0.20 – 0.49), medium (0.50 – 0.79), and large (0.80 and above).
using video feedback) have beneficial effects over and above those
According to this system, the posttreatment controlled effect size
obtained with a similar duration control procedure (Harvey et al.,
for CT (1.31) is large, and the posttreatment controlled effect size
2000; Morgan & Raffles, 1999; Wells et al., 1995; Wells &
Meta-analyses of other CBTs for social phobia (Fedoroff &
Taylor, 2001; Feske & Chambless, 1995; Gould et al., 1997;
Taylor, 1996) have reported mean pretreatment to posttreatment
Multiple regression was used to identify possible predictors of
effect sizes between 0.80 and 1.08 for social phobia measures. In
treatment response in the total sample. Six possible predictors
trials that have focused exclusively on generalized social phobia
(initial level of depression, duration of social phobia, and presence
(Hope, Herbert, & White, 1995; Salaberria & Echeburua, 1998;
of avoidant personality disorder and patient age, gender, and
Scholing & Emmelkamp, 1993), CBT pretreatment to posttreat-
marital status) were entered, with the dependent variable being the
ment effect sizes on the social phobia measures that were used in
social phobia composite residualized gain scores at posttreatment.
the current trial have ranged from 0.56 to 1.31. The pretreatment
None of the predictors were significant.
to posttreatment effect size observed with CT in the current trial(2.14) is substantially larger, which raises the possibility that the
Equivalence Analysis for FLU ϩ SE Versus PLA ϩ SE
new CT program has enhanced efficacy. However, comparisonsbetween trials are fraught with difficulty because of differences in
To investigate the apparent lack of difference between FLU ϩ
selection criteria, patient demographics, and other characteristics.
SE and PLA ϩ SE, we conducted an equivalence analysis (see
For this reason, a within-trial comparison between CT and other
Rogers, Howard, & Vessey, 1993) on the social phobia composite
established behavioral and cognitive– behavioral programs is
data for the two medication conditions. Equivalence analysis al-
lows one to further explore a null result by calculating the largestpossible difference between two conditions that a study may havemissed because of limitations of statistical power. Setting alpha at
Effectiveness of Medication Plus Self-Exposure
.05 and using equivalence analysis, we reject the hypothesis thatFLU ϩ SE has a posttreatment adjusted mean on the social phobia
Patients who received medication plus self-exposure showed
composite that is more than 0.70 superior to that for PLA ϩ SE.
significant and substantial improvements on almost all social pho-
However, we are not able to reject the hypothesis that FLU ϩ SE
bia measures between pretreatment and posttreatment. The im-
is more effective than PLA ϩ SE but the difference is less than
provement observed with PLA ϩ SE was not surprising given the
0.70. If we convert this calculation into controlled effect sizes, our
established efficacy of self-exposure in phobic disorders. At the
sample size does not allow us to reject the hypothesis that, com-
time the trial was planned, five open trials (Black et al., 1992;
pared with the PLA ϩ SE control condition, FLU ϩ SE has a
Koponen et al., 1995; Perugi et al., 1994; Schneier et al., 1992;
positive effect size of up to 0.56 (a medium effect size in Cohen’s
Van Ameringen et al., 1993) suggested that fluoxetine is effective.
Since the start of the trial, several randomized controlled trialsestablishing the effectiveness of other SSRIs have been published. Given these points, we were surprised to find that FLU ϩ SE was
not more effective than PLA ϩ SE. This finding cannot be attrib-uted to inadequate dosage, as almost everyone was prescribed the
Effectiveness of Cognitive Therapy
maximum of 60 mg and plasma analysis indicated excellent com-
The overall pattern of results indicates that CT is an effective
pliance, with all patients in the fluoxetine condition having suitable
treatment for generalized social phobia. Patients treated with CT
blood levels of fluoxetine and its metabolite (norfluoxetine). There
improved significantly more than patients who received self-
are at least three other (possibly interacting) explanations for the
exposure instructions combined with fluoxetine or placebo. In
lack of difference between FLU ϩ SE and PLA ϩ SE.
addition, the gains obtained in treatment were well maintained at
First, the present trial is underpowered relative to most recent
medication trials that routinely have larger cell sizes. Our
In line with routine clinical practice, CT sessions were longer
equivalence-testing analysis indicated that with our cell size of 20
than medication plus self-exposure sessions. This raises the pos-
patients, a difference between FLU ϩ SE and PLA ϩ SE equiv-
sibility that the superiority of CT could have been due to greater
alent to a medium controlled effect size (Cohen, 1988), could have
therapist contact. A further trial with a control treatment involving
been missed. Since the completion of the trial, two other groups
an identical amount of therapist contact is required to definitively
have reported fluoxetine versus placebo comparisons. The results
address this question. However, there are two reasons for suppos-
obtained by these two groups are consistent with the reduced
ing that therapist contact alone is unlikely to explain the superi-
power argument. In a published study using cell sizes of 30 per
ority of CT. First, in a recent social phobia trial, Heimberg et al.
group, Kobak, Greist, Jefferson, and Katzelnick (2002) failed to
(1998) found that 150-min sessions of education and support were
find a significant difference between fluoxetine and placebo. By
no more effective than 30-min sessions devoted to administering a
contrast, in a conference paper, Huppert, Roth, Keefe, Davidson,
pill placebo, and both conditions were inferior to 150-min sessions
and Foa (2002) reported obtaining some significant differences
of CBGT. Second, therapy experiments that attempt to assess the
between fluoxetine and placebo when a larger cell size (approxi-
short-term impact of discrete therapy maneuvers have shown that
mately 60 patients per group) was used.
Second, fluoxetine may be less effective in social phobia than
the three other SSRIs (fluvoxamine, sertraline, paroxetine) thathave been shown to be effective in randomized controlled trials.
In CT and FLU ϩ SE the improvements obtained at the end of
Consistent with this suggestion, the controlled effect sizes ob-
treatment were maintained at 1-year follow-up. The CT finding is
served with fluoxetine in the present trial and in Kobak et al.’s
in line with other CBT research (see Fedoroff & Taylor, 2001;
(2002) trial are generally lower than those reported in trials of the
Taylor, 1996). For medications, some studies (e.g., Liebowitz et
other SSRIs (see Fedoroff & Taylor, 2001; Gould et al., 1997). A
al., 1999) have shown an increased relapse rate following discon-
trial involving a direct comparison between fluoxetine and the
tinuation. It is encouraging that this did not happen in the present
other SSRIs is required to clarify this point. If fluoxetine does turn
study, perhaps because medication was combined with self-
out to be less effective, the finding may be an important lead in
exposure. Further studies could explore this issue by comparing
helping clarify the neurobiology of social anxiety. For example,
long-term outcome of medication alone versus medication plus
fluoxetine differs from fluvoxamine, sertraline, and paroxetine in
the relative balance of its noradrenergic and serotinergic effects(Leonard, 1996; Stahl, 1998).
Third, the fluoxetine versus placebo contrast in the present trial
may have been shorter than ideal. Kobak et al.’s (2002) main
Four limitations need to be borne in mind when interpreting the
contrast was after 14 weeks and ours was after 16 weeks. How-
study. First, as mentioned above, the sample size for a drug–
ever, patients in the present trial who stayed on fluoxetine after the
placebo comparison was relatively modest, and a medium size
medication blind was broken (at 16 weeks) showed further signif-
active medication effect could have been missed. Second, it is
icant improvement between that point and the end of the booster
possible that fluoxetine is less effective than some other SSRIs
period (28 weeks). It is therefore possible that a significant differ-
and, as a consequence, one cannot assume that the observed
ence between fluoxetine and placebo might have emerged between
difference between CT and FLU ϩ SE would generalize to other
SSRIs. Third, the exposure element in the medication ϩ SE groups
The present trial was relatively unusual in combining medica-
was less extensive than in most formal exposure programs. There
tion with self-exposure. Only two previous social phobia medica-
were no therapist-assisted or in-session exposure exercises. In
tion trials (Blomhoff et al., 2001; Gelernter et al., 1991) have had
addition, as do many pharmacotherapists, the psychiatrists who
a similar design. However, it seems unlikely that adding self-
delivered the medication treatments had little previous formal
exposure contributed to lack of difference between fluoxetine and
training in CBT. It is possible that both fluoxetine and placebo
placebo, as Kobak et al. (2002) did not use self-exposure and still
would have been associated with greater improvement if they had
failed to find a significant difference between fluoxetine and
been combined with a more extensive exposure program delivered
by therapists with specialized training in CBT. Fourth, it is unclearwhether the results can be generalized to patients with specificsocial phobia or to patients with generalized social phobia and
Contrast Between Social Phobia and General Mood
concurrent major depression, as both types of patient were ex-
cluded from the study. Specific social phobia was excluded be-cause it is generally less disabling and was also considered less
In contrast to the results obtained with standardized measures of
likely to respond to medication, but no studies have formally tested
social phobia, at posttreatment there were no significant between-
this suggestion. Comorbid major depression was excluded to en-
group differences on the two general mood measures (BDI and
sure that any medication effect was not an indirect consequence of
BAI). The substantial improvements in depression that were ob-
treating depression rather than a direct effect on social phobia.
served with all three treatments are consistent with the view thatmuch of the depressed mood observed in our patients was second-ary to their social phobia. This is perhaps not surprising when one
recalls that patients with concurrent major depressive disorderwere excluded from the study. The observed lack of difference
Allgulander, C. (1999). Paroxetine in social anxiety disorder: A random-
ized placebo-controlled study. Acta Psychiatrica Scandinavica, 100,
between the three treatments on the BDI in our sample could be
viewed as an indication of the treatments’ particularly specific
American Psychiatric Association. (1994). Diagnostic and statistical man-
effects on social phobia or it could be the consequence of a floor
ual of mental disorders (4th ed.). Washington DC: Author.
effect. Consistent with the latter suggestion, in all three treatments
Baker, S. L., Heinrichs, N., Kim, H-J., & Hofman, S. G. (2002). The
the posttreatment means for the BDI were in the nonclinical range.
Liebowitz Social Anxiety Scale as a self-report instrument: A prelimi-
Similarly to the BDI, the BAI showed substantial but broadly
nary psychometric analysis. Behaviour Research and Therapy, 40, 701–
similar improvement in all three treatments, with CT differing
from FLU ϩ SE only at the 12-month follow-up. Posttreatment
Baldwin, D., Bobes, J., Stein, D. J., Scharwa¨chter, I., & Faure, M. (1999).
means for the BAI were in the minimal or mild anxiety range
Paroxetine in social phobia/social anxiety disorder: A randomized,
(Beck & Steer, 1993), suggesting a floor effect on this measure as
double-blind, placebo-controlled trial. British Journal of Psychiatry,175, 120 –126.
well. In addition, the BAI may have relatively poor sensitivity as
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory
an outcome measure in phobic disorders because the extensive
for measuring clinical anxiety: Psychometric properties. Journal of
avoidance of feared situations shown by severe phobics can result
Consulting and Clinical Psychology, 56, 893– 897.
in low pretreatment scores on general measures of anxious mood
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitivetherapy of depression. New York: Guilford Press.
Beck, A. T., & Steer, R. A. (1993). Beck Anxiety Inventory Manual. San
ficial effects of video feedback following a stressful social task. Behav-
Antonio, TX: Psychological Corporation. iour Research and Therapy, 38, 1183–1192.
Black, B., Uhde, T. W., & Tancer, M. E. (1992). Fluoxetine for the
Heckelman, L. R., & Schneier, F. R. (1995). Diagnostic issues. In R.
treatment of social phobia. Journal of Clinical Psychopharmacology, 12,
Heimberg, M. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Socialphobia: Diagnosis, assessment and treatment (pp. 2–20). New York:
Blomhoff, S., Haug, T. T., Hellstro¨m, K., Holme, I., Humble, M., Madsbu,
H. P., et al. (2001). Randomized controlled general practice trial of
Heimberg, R. G., Liebowitz, M. R., Hope, D. A., Schneier, F. R., Holt,
sertraline, exposure therapy and combined treatment in generalized
C. S., Welkowitz, L. A., et al. (1998). Cognitive– behavioral group
social phobia. British Journal of Psychiatry, 179, 23–30.
therapy vs. phenelzine therapy for social phobia. Archives of General
Brown, T. A., Di Nardo, P. A., & Barlow, D. H. (1994). Anxiety DisordersInterview Schedule for DSM–IV. Albany, NY: Graywind Publications.
Heimberg, R. G., Salzman, D. G., Holt, C. S., & Blendell, K. A. (1993).
Chambless, D. L., & Hope, D. A. (1996). Cognitive approaches to the
Cognitive– behavioral group treatment for social phobia: Effectiveness
psychopathology and treatment of social phobia. In P. M. Salkovskis
at 5-year follow-up. Cognitive Therapy and Research, 14, 1–23.
(Ed.), Frontiers of cognitive therapy (pp. 345–382). New York: Guilford
Hollon, S. D., De Rubeis, R. J., Evans, M. D., Wierner, M. J., Garvey,
M. J., Grove, W. M., et al. (1992). Cognitive therapy and pharmaco-
Clark, D. M. (1997). Cognitive therapy for social phobia: Some notes for
therapy for depression: Singly and in combination. Archives of Generaltherapists. Unpublished manuscript.
Clark, D. M. (2001). A cognitive perspective on social phobia. In W. R.
Hood, S. D., & Nutt, D. J. (2001). Psychopharmacological treatments: An
Crozier & L. E. Alden (Eds.), International handbook of social anxiety
overview. In W. R. Crozier & L. E. Alden (Eds.), International hand-
(pp. 405– 430). Chichester, UK: Wiley. book of social anxiety (pp. 471–504). Chichester, UK: Wiley.
Clark, D. M., Salkovskis, P. M., Hackmann, A., Middleton, H., Anasta-
Hope, D., Herbert, J., & White, C. (1995). Diagnostic subtype, avoidant
siades, P., & Gelder, M. G. (1994). A comparison of cognitive therapy,
personality disorder, and efficacy of cognitive– behavioral group therapy
applied relaxation and imipramine in the treatment of panic disorder.
for social phobia. Cognitive Therapy and Research, 19, 399 – 417. British Journal of Psychiatry, 164, 759 –769.
Huppert, J. D., Roth, D. A., Keefe, F. J., Davidson, J. R. T., & Foa, E. B.
Clark, D. M., Salkovskis, P. M., Hackmann, A., Wells, A., Ludgate, J., &
(2002, November). Comprehensive CBT, fluoxetine, and their combina-tion: A randomized, placebo controlled trial. Paper presented at the 36th
Gelder, M. (1999). Brief cognitive therapy for panic disorder: A ran-
Annual Convention of the Association for Advancement of Behavior
domized controlled trial. Journal of Consulting and Clinical Psychology,
Kobak, K. A., Greist, J. H., Jefferson, J. W., & Katzelnick, D. J. (2002).
Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In
Fluoxetine in social phobia: A double-blind, placebo-controlled pilot
R. Heimberg, M. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social
study. Journal of Clinical Psychopharmacology, 22, 257–262. phobia: Diagnosis, assessment and treatment (pp. 69 –93). New York:
Koponen, H., Lepola, U., & Juhani, L. E. V. (1995, March). Fluoxetine insocial phobia: A pilot study. Paper presented at the 15th National
Cohen, J. (1988). Statistical power analysis for the behavioral sciences
Conference of the Anxiety Disorders Association of America, Pitts-
Committee on Safety of Medicines. (1988). Benzodiazepines, dependence
Leonard, B. E. (1996). The comparative pharmacological properties of
and withdrawal symptoms. Current Problems, 21, 1–2.
selective serotonin re-uptake inhibitors in animals. In J. P. Feighner &
Fedoroff, I. C., & Taylor, S. (2001). Psychological and pharmacological
W. F. Boyer (Eds.), Selective serotonin re-uptake inhibitors (2nd ed., pp.
treatments of social phobia: A meta-analysis. Journal of Clinical Psy-chopharmacology, 21, 311–324.
Liebowitz, M. R. (1987). Social phobia. Modern problems in Pharma-
Feske, U., & Chambless, D. L. (1995). Cognitive– behavioral versus ex-
posure only treatment for social phobia: A meta-analysis. Behavior
Liebowitz, M. R., Heimberg, R. G., Schneier, F. R., Hope, D. A., Davies,
S., Holt, C. S., et al. (1999). Cognitive– behavioral group therapy versus
First, B. M., Gibbon, M., Spitzer, R. L., Williams, J. B. W., & Benjamin,
phenelzine in social phobia: Long-term outcome. Depression and Anx-
L. S. (1997). User’s guide for the Structured Clinical Interview forDSM–IV Axis II Personality Disorders: SCID-II. Washington, DC:
Liebowitz, M. R., Schneier, F., Campeas, R., Hollander, E., Hatterer, J.,
Fyer, A. J., et al. (1992). Phenelzine vs. atenolol in social phobia: A
First, B. M., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1995).
placebo-controlled comparison. Archives of General Psychiatry, 49,User’s guide for the Structured Clinical Interview for DSM–IV Axis IDisorders: SCID-I Clinician Version. Washington, DC: American Psy-
Magee, W. J., Eaton, W. W., Wittchen, H-U., Gonagle, K. A., & Kessler,
R. C. (1996). Agoraphobia, simple phobia, and social phobia in the
Fresco, D. M., Erwin, B. A., Heimberg, R. G., & Turk, C. L. (2000). Social
National Comorbidity Survey. Archives of General Psychiatry, 53, 159 –
phobia and specific phobias. In M. G. Gelder, J. Lopez-Ibor, & N. C.
Andreasen (Eds.), New Oxford textbook of psychiatry (pp. 794 – 807).
Marks, I., & Mathews, A. M. (1979). Brief standard self-rating for phobic
Oxford, UK: Oxford University Press.
patients. Behaviour Research and Therapy, 17, 263–267.
Gelernter, C. S., Uhde, T. W., Cimbolic, P., Arnkoff, D. B., Vittone, B. J.,
Mattick, R. P., & Clarke, J. C. (1998). Development and validation of
Tancer, M. E., & Bartko, J. J. (1991). Cognitive– behavioral and phar-
measures of social phobia scrutiny fear and social interaction anxiety.
macological treatments of social phobia: A controlled study. Archives ofBehaviour Research and Therapy, 36, 455– 470. General Psychiatry, 48, 938 –945.
Mattick, R. P., & Peters, L. (1988). Treatment of severe social phobia:
Gould, R. A., Buckminster, S., Pollack, M. H., Otto, M. W., & Yap, L.
Effects of guided exposure with and without cognitive restructuring.
(1997). Cognitive– behavioral and pharmacological treatment for social
Journal of Consulting and Clinical Psychology, 56, 251–260.
phobia: A meta-analysis. Clinical Psychological Science Practice, 4,
Morgan, H., & Raffles, C. (1999). Does reducing safety behaviours im-
prove treatment response in patients with social phobia? Australian and
Harvey, A. G., Clark, D. M., Ehlers, A., & Rapee, R. M. (2000). Social
New Zealand Journal of Psychiatry, 33, 503–510.
anxiety and self-impression: Cognitive preparation enhances the bene-
Perugi, G., Nassini, S., Lenzi, M. Simonini, E., Cassano, G. B., & McNair,
D. M. (1994). Treatment of social phobia with fluoxetine. Anxiety, 1,
Taylor, S. (1996). Meta-analysis of cognitive– behavioral treatments for
social phobia. Journal of Behavior Therapy and Experimental Psychi-
Rapee, R. M. (1995). Descriptive psychopathology of social phobia. In R.
Heimberg, M. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social
Van Ameringen, M., Lane, R. M., Bowen, R. C., Chokka, P. R., Goldner,
phobia: Diagnosis, assessment and treatment (pp. 41– 69). New York:
E. M., Johnston, D. G., et al. (2001). Sertraline treatment of generalized
social phobia: A 20 week, double-blind, placebo-controlled study. Amer-
Rapee, R. M., & Heimberg, R. G. (1997). A cognitive– behavioral model of
ican Journal of Psychiatry, 158, 275–281.
anxiety in social phobia. Behaviour Research & Therapy, 35, 741–756.
Van Ameringen, M., Mancini, C., & Streiner, D. L. (1993). Fluoxetine
Rogers, J. L., Howard, K. I., & Vessey, J. T. (1993). Using significance
efficacy in social phobia. Journal of Clinical Psychiatry, 54, 27–31.
tests to evaluate equivalence between two experimental groups. Psycho-
Van Ameringen, M., Swinson, R. P., Walker, J. R., & Lane, R. M. (1999). logical Bulletin, 113, 553–565.
A placebo-controlled study of sertraline in generalized social phobia.
Rosenthal, R., & Rosnow, R. L. (1991). Essentials of behavioral research:Journal of the European College of Neuropsychopharmacology,Methods and data analysis (2nd ed.). New York: McGraw-Hill.
Salaberria, K., & Echeburua, E. (1998). Long-term outcome of cognitive
Versiani, M., Nardi, A. E., Mundim, F. D., Alves, A. B., Liebowitz, M. R.,
therapy’s contribution to self-exposure in vivo to the treatment of
& Amrein, R. (1992). Pharmacotherapy of social phobia: A controlled
generalized social phobia. Behavior Modification, 22, 262–284.
study with moclobemide and phenelzine. British Journal of Psychiatry,
Schneier, F. R., Chin, S. J., Hollander, E., & Liebowitz, M. R. (1992).
Fluoxetine in social phobia. Journal of Clinical Psychopharmacology,
Watson, D., & Friend, R. (1969). Measurement of social-evaluative anxi-
ety. Journal of Consulting and Clinical Psychology, 33, 448 – 457.
Scholing, A., & Emmelkamp, P. M. G. (1993). Exposure with and without
Wells, A. (1997). Cognitive therapy of anxiety disorders: A practice
cognitive therapy for generalized social phobia: Effects of individual and
manual and conceptual guide. Chichester, UK: Wiley.
group treatment. Behaviour Research and Therapy, 31, 667– 681.
Wells, A., Clark, D. M., Salkovskis, P. M., Ludgate, J., Hackmann, A., &
Stahl, S. M. (1998). Not so selective serotonin inhibitors. Journal of
Gelder, M. (1995). Social phobia: The role of in-situation safety behav-
Clinical Psychiatry, 59, 343–344.
iors in maintaining anxiety and negative beliefs. Behavior Therapy, 26,
Stein, M. B., Fyer, A. J., Davidson, J. R. T., Pollack, M. H., & Wiita, B.
(1999). Fluvoxamine treatment of social phobia (social anxiety disor-
Wells, A., & Papageorgiou, C. (1998). Social phobia: Effects of external
attention on anxiety, negative beliefs, and perspective taking. Behavior
der): A double-blind, placebo-controlled study. American Journal of
Stein, M. B., Liebowitz, M. R., Lydiard, B., Pitts, C. D., Bushnell, W., &
Gergel, I. (1998). Paroxetine treatment of generalized social phobia
(social anxiety disorder): A randomized controlled trial. JAMA, 280,
Puppy Strangles I want to alert you to a condition that may onset in puppies between the ages of two and four months. Because it is often misdiagnosed and because it has potentially fatal consequences, you may want to bring this information to your veterinarian's attention should your puppy present any of the typical symptoms: The condition is variously referred to as juvenile cellulitis
Video Presentation Transcript >>Good morning from the Centers of Disease Control and Prevention where we are currently managing public health responses to not only the ongoing H1N1 outbreak but also Anthrax, Salmonella and the Haiti Earthquake response. I'm not sure where I'm supposed to point this. This is the first presentation, CDC Public Health Preparedness and Response. [background
 with last available data carried forward, with the exception of the 12-monthfollow-up analysis, in which data for patients who failed to reach theposttreatment assessment were not carried forward.2 To identify any dif-ferences between groups before treatment, we compared initial scores forthe three treatment groups with the liberal procedure of separate one-wayanalyses of variance (ANOVAs) for each measure. To identify any differ-ences between groups at midtreatment, posttreatment or follow-up, weused one-way analyses of covariance (ANCOVAs) with pretreatmentscores as covariates followed by post hoc Duncan’s multiple range testswhen comparing more than two means. We used t tests to identify signif-icant within-treatment changes. A two-step approach was adopted to dealwith multiple measurement of social phobia. First, a single unweightedsocial phobia composite was created and analyzed. Only if the compositerevealed significant between- or within-group differences were furtherANCOVAs or t tests performed on individual social phobia measures. Thecomposite was generated with the procedure recommended by Rosenthal
Social phobia composite scores at each assessment. CT ϭ
and Rosnow (1991) and adopted in several previous trials (e.g., Clark et al.,
cognitive therapy; FLU ϩ SE ϭ fluoxetine plus self-exposure; PLA ϩ
1994, 1999; Hollon et al., 1992). Patients’ scores on each (of seven) social
SE ϭ placebo plus self-exposure; pre ϭ pretreatment, mid ϭ midtreat-
phobia measures were standardized (M ϭ 0, SD ϭ 1) across pre- and
ment; post ϭ posttreatment; 12m FU ϭ 12-month follow-up.
with last available data carried forward, with the exception of the 12-monthfollow-up analysis, in which data for patients who failed to reach theposttreatment assessment were not carried forward.2 To identify any dif-ferences between groups before treatment, we compared initial scores forthe three treatment groups with the liberal procedure of separate one-wayanalyses of variance (ANOVAs) for each measure. To identify any differ-ences between groups at midtreatment, posttreatment or follow-up, weused one-way analyses of covariance (ANCOVAs) with pretreatmentscores as covariates followed by post hoc Duncan’s multiple range testswhen comparing more than two means. We used t tests to identify signif-icant within-treatment changes. A two-step approach was adopted to dealwith multiple measurement of social phobia. First, a single unweightedsocial phobia composite was created and analyzed. Only if the compositerevealed significant between- or within-group differences were furtherANCOVAs or t tests performed on individual social phobia measures. Thecomposite was generated with the procedure recommended by Rosenthal
Social phobia composite scores at each assessment. CT ϭ
and Rosnow (1991) and adopted in several previous trials (e.g., Clark et al.,
cognitive therapy; FLU ϩ SE ϭ fluoxetine plus self-exposure; PLA ϩ
1994, 1999; Hollon et al., 1992). Patients’ scores on each (of seven) social
SE ϭ placebo plus self-exposure; pre ϭ pretreatment, mid ϭ midtreat-
phobia measures were standardized (M ϭ 0, SD ϭ 1) across pre- and
ment; post ϭ posttreatment; 12m FU ϭ 12-month follow-up.