Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Dmip.ecb.epm.br
Journal of Medical Microbiology (2006), 55, 127–131
Detection of mixed infections with Mycobacteriumlentiflavum and Mycobacterium avium by moleculargenotyping methods
Philip Suffys,1 Adalgiza da Silva Rocha,1 Adeilton Branda˜o,2Bart Vanderborght,3 Wouter Mijs,4 Geert Jannes,4 Fernanda C. Q. Mello,3Heloisa da Silveira Paro Pedro,5 Leila de Souza Fonseca,6Rosaˆngela Siqueira de Oliveira,7 Sylvia Cardoso Lea˜o7and Maria Helena Fe´res Saad1
Department of Mycobacterioses1 and Department of Tropical Medicine2, Oswaldo Cruz
Institute, Fiocruz, Rio de Janeiro, Brazil
3,6University Hospital Clementino Fraga Filho3 and Microbiology Institute6, Federal University of
Rio de Janeiro (UFRJ), Rio de Janeiro, Brazil
4Innogenetics N. V., Technologiepark 6, B-9052 Ghent, Belgium
5Adolfo Lutz Institute, Sa˜o Paulo, Brazil
7Department of Microbiology, Immunology and Parasitology, Paulista School of Medicine,
Three mycobacterial isolates, one from the blood of an HIV-infected patient and two consecutiveisolates from a woman with unknown HIV status, had been identified as belonging to theMycobacterium avium complex by conventional procedures. In both patients, using genetic analysisprocedures such as PCR–restriction enzyme analysis (PRA) of the hsp65 gene, a commerciallyavailable reverse hybridization-based assay (INNO-LiPA MYCOBACTERIA) and/or sequencinganalysis of the 16S–23S internal transcribed spacer (ITS), the presence of Mycobacteriumlentiflavum was also demonstrated. At the time of detection, both cases were also infected with M.
avium, suggesting an underestimation of infection with M. lentiflavum and co-infection with different
2002). The main reservoir in the environment has not been
Mycobacterium lentiflavum is a slowly growing acid-fast
firmly established, but organisms with M. lentiflavum-like
bacillus (AFB) that has biochemical characteristics identical
16S rRNA gene sequences were detected in soil samples from
to those of organisms belonging to the Mycobacterium
the UK and from France (Mendum et al., 2000) and the
avium complex (MAC) and mycolic acid and fatty acid
species seems to be frequently present in drinking water
chromatography patterns very similar to those of Myco-
distribution systems in Finland (Torvinen et al., 2004). We
bacterium simiae, so genetic analysis is necessary for con-
here report the detection of a co-infection with M. aviumand M. lentiflavum in the blood or lung of two different
clusive identification (Springer et al., 1996). This organism
has been isolated from sterile clinical samples in Italy,Switzerland, Germany, France and Spain (Springer et al.,1996; Tortoli et al., 1997; Niobe et al., 2001; Ibanez et al.,2002) and from sputum samples in Brazil (da Silva Rocha
et al., 1999) and Italy (Molteni et al., 2005) and, recently,
cases of human disease have been reported, includingchronic pulmonary disease (Molteni et al., 2005), cervical
Case 1. In December 1994, a 27-year-old Caucasian male was sub-
lymphadenitis (Cabria et al., 2002), liver abscess (Tortoli
mitted to a renal biopsy at the Clementino Fraga Filho University
et al., 2002) and fatal disseminated infection (Ibanez et al.,
Hospital in Rio de Janeiro and membranoproliferative glomerulo-nephritis type I was diagnosed. The individual was submitted tointravenous corticoid treatment and discharged from the hospital
Abbreviations: AFB, acid-fast bacillus; ITS, internal transcribed spacer;
while continuing oral methylprednisone treatment that was gradu-
MAC, Mycobacterium avium complex; PRA, PCR–restriction enzyme
ally reduced until interruption in December 1995. By that time, the
patient had developed lymphopenia (as shown by CD4 lymphocyte
counts of 500 cells mm23) that was held under control, but, in
M. intracellulare and M. avium, respectively, according to Thierry
September 1996, he returned with weight loss, cough, fever and oral
et al. (1993), while the presence of the insertion sequence IS1245 is
candidiasis. A chest X-ray revealed a diffuse reticulonodular infiltrate
indicative of M. avium (Guerrero et al., 1995). Because the two cases
suggestive of active pulmonary disease. Sputum bacteriology showed
were investigated independently by different research groups, the
no evidence of AFB, but pneumocystosis, a definitive marker of
methodologies performed on the isolates from the two patients were
AIDS, was diagnosed and infection with HIV was confirmed. Treat-
ment of pneumocystosis resulted in clinical improvement but,3 weeks later, the patient returned with high fever and aqueous diar-rhoea. A blood culture was performed and was positive for AFB.
Upon treatment with streptomycin, sulphamethoxazole/trimethro-prim and corticoid, the patient improved and was discharged from
the hospital in October 1996. Two weeks later he returned to thehospital and received zidovidine and didanosine and was discharged
Blood culture yielded small, pale-yellow, smooth-domed
with the recommendation to return for regular re-evaluation. The
colonies of AFB after 28 days of incubation at 37 uC in
patient died a few months later in another hospital and no data are
LJ medium and the culture was identified as MAC by
available on the exact cause of death.
conventional biochemical methods (negative for Tweenhydrolysis, nitrate reduction and urease and positive for
Case 2. In 1996, a 64-year-old woman was diagnosed with tubercu-
catalase and tellurite reduction). Part of the sample was
losis in the State of Mato Grosso. Despite treatment for tuberculosis
treated by heat shock and submitted to genetic characteri-
since February 1997, she presented to Public Health Care in Votu-
zation by PRA of part of the hsp65 gene (Telenti et al., 1993;
poranga, Sa˜o Paulo, with cough, fever, coryza, weakness, lack ofappetite, severe weight loss and dyspnoea. The X-ray showed bilat-
da Silva Rocha et al., 2002): no digestion with BstEII and
eral thin-walled cavitations and sputum collection revealed AFB. She
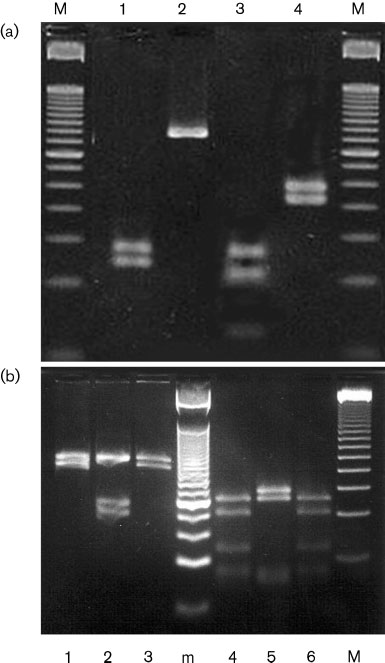
145/125 bp fragments with HaeIII were obtained (Fig. 1a).
was therefore enrolled in 1998 at the ‘Nu´cleo de Gesta˜o Assistencial’,
According to the literature, this pattern is identical to M.
a health care service. During the following 4 years, she was sub-
lentiflavum I (Springer et al., 1996), but this pattern has also
mitted to several treatment schemes for tuberculosis, including anti-
been described for M. simiae (da Silva Rocha et al., 2002).
biotics such as clarithromycin, ethambutol, clofazimine, rifampicin
The isolate was submitted to INNO-LiPA MYCOBACTERIA
and doxycycline. During this period, the patient did not showimprovement but rather a gradual worsening of the clinical symp-
and hybridized with the Mycobacterium species probe but
toms was observed with frequent positive bacilloscopy and mycobac-
not with the probes specific for MAC, confirming that the
terial cultures. In August 2002 she died of uterine cancer at 26 kg in
isolate did not belong to this complex. Since the INNO-LiPA
assay does not contain probes specific for M. lentiflavum orM. simiae, sequencing of the 16S–23S ITS was performed
Culture, conventional identification and drug susceptibility
and the isolate was confirmed to be M. lentiflavum.
testing. AFB staining was performed by the Ziehl–Neelsen method. For case 1, a blood culture was performed using the lysis-centrifugation
A subculture obtained from a small amount of the original
method (Fandinho et al., 1997) and colonies of AFB were grown byincubation on Lo¨wenstein–Jensen (LJ) medium. For case 2, sputum
bacterial mass in the tube containing LJ medium before
culture on LJ medium was performed after decontamination using
submitting it to heat shock was grown in Middlebrook 7H9
the Petroff method and centrifugation (Kent & Kubica, 1985). Sub-
and reanalysed by PRA. On this occasion, the M. avium II
culture was carried out on LJ medium and colonies were submitted
restriction digest was observed and no (not even weak)
to conventional identification (Kent & Kubica, 1985).
bands corresponding to the M. lentiflavum pattern werefound.
Genetic characterization. For genetic analysis, part of the samplewas submitted to three consecutive cycles of snap freezing andboiling in 10 mM Tris/HCl, 1 mM EDTA and 1 % Triton X-100.
The INNO-LiPA MYCOBACTERIA assay is commercially available(Innogenetics) for detection of Mycobacterium and identification of
Among the 15 Mycobacterium cultures obtained from 1997
members of the Mycobacterium tuberculosis (MTB) complex, Myco-
to 2001 on LJ medium, 12 were identified as MAC and 3 as
bacterium kansasii, M. xenopi, M. gordonae, M. avium, M. intracellu-
M. gordonae using conventional biochemical identification
lare, M. scrofulaceum and M. chelonae, targeting the 16S–23S rRNA
procedures (data not shown). Among these, two cultures,
internal transcribed spacer (ITS) region (Miller et al., 2000); this
one obtained in June 1998 and the other in September 2000
assay was evaluated in Brazil with excellent results (Suffys et al.,
and both identified as MAC, were submitted to molecular
2001). The PCR–restriction enzyme analysis (PRA) assay was origin-ally described by Telenti et al. (1993) and is based on amplification
identification procedures. Both cultures were identified as
of part of hsp65 and restriction analysis with HaeIII and BstEII;
M. intracellulare I by PRA; however, amplification results
evaluation of the assay in Brazil also demonstrated the straightfor-
using primers from the M. intracellulare-specific DT1
wardness of the method (da Silva Rocha et al., 2002). Sequencing
fragment and the M. avium-specific DT6 and IS1245
was performed on the amplified ITS that was used for INNO-LiPA
fragments were contradictory. The first isolate was negative
using a QIAquick PCR purification kit (Qiagen) and sequenced
in the three PCR systems, while the more recent isolate was
using an ABI PRISM BigDye Terminator cycle sequencing ready
positive upon amplification of DT6 and IS1245; both results
reaction kit on an ABI PRISM 377 sequencer (Applied Biosystems). Sequence analysis was performed by comparison against a database
were therefore inconsistent with the identification as M.
present at Innogenetics and against GenBank using SEQED and FASTA
of the Wisconsin Package (version 9.1; Genetics Computer Group). Some PCR systems for differentiation of M. intracellulare and M.
For that reason, subcultures were prepared on 7H10-OADC
avium were used: amplification of DT1 or DT6 is characteristic for
plates and the molecular tests were repeated on isolated
Mycobacterium lentiflavum and M. avium co-infection
contaminated bronchoscope, gastric juice and urinesamples (Springer et al., 1996), lymph nodes (Tortoli et al.,1997; Haase et al., 1997), bronchoalveolar lavage fluid and,very recently, sputum (Molteni et al., 2005); the presentreport is to our knowledge the second to demonstratedetection of M. lentiflavum in Brazil. Infection with MACis frequent in Brazilian AIDS patients (Barreto et al., 1993)and because routine identification procedures do not differ-entiate some Mycobacterium species (including M. lenti-flavum) from MAC, use of genetic methods for identifi-cation on a more routine basis would give a better idea of theprevalence of such species in this country.
Niobe et al. (2001) published the ITS sequences of a clinicalisolate of M. lentiflavum and of the type strain ATCC 51985and, although the 16S rRNA gene sequence of the clinicalisolate had 100 % identity to the sequence of the type strain,the ITS sequence of the clinical isolate had only 92?6 %identity to that of strain ATCC 51985, suggesting the need tostudy ITS variability in this species. The ITS sequence of oneM. lentiflavum isolate described here was identical to thatpublished by Niobe et al. (2001), as was the case for anotherisolate obtained from a sputum sample of an HIV-positiveindividual from Rio de Janeiro (data not shown). Thissuggests that the ITS sequence variability, at least in Brazil, islimited or non-existent while, interestingly, the isolatespresented different PRA patterns (Springer et al., 1996). Bearing in mind that the whole ITS sequence was evaluatedwhile restriction enzyme analysis only demonstrates crea-tion or destruction of restriction sites, this finding suggests
Fig. 1. Ethidium-bromide-stained agarose gels showing PRA of
that mutation in the two genes seems to occur at different
the hsp65 gene. (a) PRA patterns of isolates from Case 1.
HaeIII (lane 1) and BstEII (2) digestion products of M. lentifla-vum I and HaeIII (3) and BstEII (4) digestion products of M.
In both patients, mixed mycobacterial populations were
avium II; lanes M contain a 50 bp ladder. (b) PRA patterns of
present upon genetic analysis. Although an M. lentiflavum
isolated colonies of the second isolate of Case 2, including
pattern was observed in the original sample from the first
BstEII of M. avium II (lanes 1 and 3) and of M. lentiflavum III
patient, M. avium was observed exclusively in the sample
(2) and HaeIII of M. avium II (4 and 6) and of M. lentiflavum III
that was obtained after culturing of a fraction of that sample,
(5); lane M contains a 50 bp ladder and lane m contains a
suggesting the selection of M. avium either by fractionating
the sample during collection or because of the faster growthof M. avium; M. lentiflavum has been reported to be lessvirulent than M. intracellulare in mice (Saito et al., 2000),
colonies. In the second isolate, a mixed population contain-
and this needs to be further investigated. This suggests the
ing colonies with two different morphologies was observed;
importance of submitting identical fractions to different
PRA analysis resulted in the M. lentiflavum III pattern for
identification procedures and considering analysis of
the small yellow colonies, while the pale colonies were
isolated colonies, as confirmed by the results of character-
identified as M. avium II. This confirms the presence of a
ization of separate colonies of the second isolate of case 2.
mixed infection with two different species and explains the
Besides observing different colony morphology using this
earlier results obtained using amplification systems for DT1,
strategy, two genotypes belonging to different species were
DT6 and IS1245. On the other hand, analysis of the earlier
isolated culture yielded small yellow colonies only and PRApatterns were all M. lentiflavum III.
In the initial identification, both isolates of the secondpatient were identified as M. intracellulare by PRA. Com-paring PRA patterns of M. intracellulare and M. lentiflavum
III, the BstEII fragments are indistinguishable and there is a
In contrast to M. avium, a species isolated frequently from
one-band difference upon HaeIII digestion, a 60 bp band in
the blood of HIV-infected individuals, isolation of M.
M. intracellulare I that is absent from M. lentiflavum III.
lentiflavum from blood was described only recently (Niobe
Failure to observe the 60 bp band or the appearance of
et al., 2001). Previous reports describe isolates from
the 60 bp band from M. avium could have led to this
misinterpretation (Fig. 1b); the influence of such bands on
correct pattern interpretation has been observed before (da
This study was supported by CNPq (PRONEX 661028/1998-4), an
Silva Rocha et al., 1999; Lea˜o et al., 2005).
International Collaborations in Disease Research (ICIDR) grant andFAPESP 98/11746-1. R. S. de O. was supported by CAPES and
Sequencing also confirmed that the isolates were actually
A. da S. R. by Faperj. We thank Lucilaine Ferrazoli for patient record
M. lentiflavum rather than M. intracellulare. In our earlier
information and Dr Lee Riley for his thoughts on existing but not yet
study, the PRA pattern M. lentiflavum III was also observed
in about half of the M. intracellulare isolates, adding onemore identifying pattern for the latter species (da SilvaRocha et al., 1999). The fact that these two species that are
hard to separate by conventional identification and have thesame PRA type co-exist in Brazil demonstrates the need to
Barreto, J. A., Palaci, M., Ferrazoli, L. & 7 other authors (1993). Isolation of Mycobacterium avium complex from bone marrow
use different genotype assays for some organisms. Also, M.
aspirates of AIDS patients in Brazil. J Infect Dis 168, 777–779.
lentiflavum was present in cultures from material taken with
Cabria, F., Torres, M. V., Garcia-Cia, J. I., Dominguez-Garrido, M. N.,
a 2 year interval, showing that this species is more than a
Esteban, J. & Jimenez, M. S. (2002). Cervical lymphadenitis caused
by Mycobacterium lentiflavum. Pediatr Infect Dis J 21, 574–575.
da Silva Rocha, A., da Costa Leite, C., Torres, H. M., de Miranda,
Prior to the HIV era, mixed mycobacterial infections
A. B., Pires Lopes, M. Q., Degrave, W. M. & Suffys, P. N. (1999). Use
consisted mainly of M. tuberculosis and some atypical
of PCR-restriction fragment length polymorphism analysis of the
mycobacteria. However due to immune suppression, simul-
hsp65 gene for rapid identification of mycobacteria in Brazil.
taneous infection with different atypical Mycobacterium
species is now more frequent; polyclonal infection of M.
da Silva Rocha, A., Werneck Barreto, A. M., Dias Campos, C. E.,
avium strains has been reported in AIDS patients in Brazil
Villas-Boˆas da Silva, M., Fonseca, L., Saad, M. H., Degrave, W. M. &
(Oliveira et al., 2000; Saad et al., 2000). So far, simultaneous
Suffys, P. N. (2002). Novel allelic variants of mycobacteria isolated in
infection of M. avium and M. lentiflavum has not been
Brazil as determined by PCR-restriction enzyme analysis of hsp65. J Clin Microbiol 40, 4191–4196.
reported, probably because the two species are phenotypi-
Fandinho, F. C., Grinsztejn, B., Veloso, V. G., Lourenc¸o, M. C. S.,
cally indistinguishable. Although we suspect that Case 2
Werneck-Barroso, E., Joa˜o, E., Nogueira, A. S. & de Souza
could initially have been infected with M. avium (and M.
gordonae), superinfection with M. lentiflavum probably
infection: testing a simple and inexpensive method for use in
occurred when the patient was being treated for cancer.
developing countries. Bull World Health Organ 75, 361–366.
Infection with M. lentiflavum has been diagnosed in the lung
Galarraga, M. C., Torreblanca, A. & Jimenez, M. S. (2002). Isolation
of a woman that had been treated with corticoids because of
of Mycobacterium lentiflavum in a case of suspected lung cancer.
suspicion of lung cancer (Galarraga et al., 2002), but this
Enferm Infecc Microbiol Clin 20, 93–94 (in Spanish).
association is difficult to confirm here because not all
Guerrero, C., Bernasconi, C., Burki, D., Bodmer, T. & Telenti, A.
isolates have been submitted to genetic analysis. Because of
(1995). A novel insertion element from Mycobacterium avium,
the lack of clinical data and the presence of different
IS1245, is a specific target for analysis of strain relatedness. J ClinMicrobiol 33, 304–307.
mycobacterial species, it was not possible to associate the
Haase, G., Kentrup, H., Skopnik, H., Springer, B. & Bottger, E. C.
presence of M. lentiflavum with the pathological states of the
(1997). Mycobacterium lentiflavum: an etiologic agent of cervical
patients, but both disseminated disease (Niobe et al., 2001)
lymphadenitis. Clin Infect Dis 25, 1245–1246.
and chronic pulmonary disease (Oliveira et al., 2000) caused
Ibanez, R., Serrano Heranz, R., Jimenez-Palop, M., Roman, C.,
by M. lentiflavum have been reported. Although M. lenti-
Corteguera, M. & Jimenez, S. (2002). Disseminated infection caused
flavum has been reported to be susceptible to several anti-
by slow-growing Mycobacterium lentiflavum. Eur J Clin Microbiol
biotics used for treatment of infection with mycobacteria
other than M. tuberculosis (MOTT) (Niobe et al., 2001;
Idigoras, P., Beristain, X. & Jimenez-Pajares, M. S. (2004). Clinically
Molteni et al., 2005), the clinical significance of suscept-
insignificant Mycobacterium lentiflavum isolation in 30 patients.
ibility testing of these organisms has not been fully validated
Enferm Infecc Microbiol Clin 22, 199–200 (in Spanish).
and complicates decisions on proper treatment of infection
Kent, P. T. & Kubica, G. P. (1985). Public Health Mycobacteriology. A
Guide for the Level III Laboratory. Atlanta: Centers for DiseaseControl.
The fact that M. lentiflavum has been reported in particular
Lea˜o, S. C., Bernardelli, A., Cataldi, A. & 23 other authors (2005).
situations as one of the more frequently isolated myco-
Multicenter evaluation of mycobacteria identification by PCRrestriction enzyme analysis in laboratories from Latin America and
bacteria not associated with disease (Idigoras et al., 2004),
the Caribbean. J Microbiol Methods 61, 193–199.
has been isolated from drinking water (Torvinen et al., 2004)
Mendum, T. A., Chilima, B. Z. & Hirsch, P. R. (2000). The PCR
and can lead to fatal disseminated disease highlights the
amplification of non-tuberculous mycobacterial 16S rRNA sequences
importance of the correct identification of this species.
from soil. FEMS Microbiol Lett 185, 189–192.
Molecular identification tools can aid in characterization
Miller, N., Infante, S. & Cleary, T. (2000). Evaluation of the LiPA
and thus in better understanding of the epidemiology of this
MYCOBACTERIA assay for identification of mycobacterial species from
BACTEC 12B bottles. J Clin Microbiol 38, 1915–1919.
Mycobacterium lentiflavum and M. avium co-infection
Molteni, C., Gazzola, L., Cesari, M., Lombardi, A., Salerno, F., Tortoli,
mycobacteria: description of Mycobacterium lentiflavum sp. nov.
E., Codecasa, F., Penati, V., Franzetti, F. & Gori, A. (2005).
Mycobacterium lentiflavum infection in immunocompetent patients.
Suffys, P. N., da Silva Rocha, A., de Oliveira, M. & 9 other authors
(2001). Rapid identification of mycobacteria to the species level
Niobe, S. N., Bebear, C. M., Clerc, M., Pellegrin, J.-L., Bebear, C. &
using INNO-LiPA Mycobacteria, a reverse hybridization assay. J Clin
Maugein, J. (2001). Disseminated Mycobacterium lentiflavum infec-
tion in a human immunodeficiency virus-infected patient. J Clin
Telenti, A., Marchesi, F., Balz, M., Bally, F., Bottger, E. & Bodmer, T.
(1993). Rapid identification of mycobacteria to the species level by
Oliveira, R. S., Sircili, M. P., Ueki, S. Y. M., Telles, M. A. S., Schnabel,
polymerase chain reaction and restriction enzyme analysis. J Clin
B., Briones, M. R. S. & Lea˜o, S. C. (2000). PCR-restriction enzyme
analysis of a bone marrow isolate from a human immunodeficiency
Thierry, D., Vincent, V., Clement, F. & Guesdon, J. L. (1993).
virus-positive patient discloses polyclonal infection with two
Isolation of specific DNA fragments of Mycobacterium avium and
Mycobacterium avium strains. J Clin Microbiol 38, 4643–4645.
their possible use in diagnosis. J Clin Microbiol 31, 1048–1054.
Saad, M. H., Telles, M. A., Porfirio, F., Ferrazoli, L., de Souza
Tortoli, E., Piersimoni, C., Kirschner, P. & 10 other authors (1997).
Fonseca, L., Johnson, W., Jr & Riley, L. W. (2000). Multiple isolates
Characterization of mycobacterial isolates phylogenetically related to,
from aids patients: aspects of an analysis by a genotypic marker
but different from Mycobacterium simiae. J Clin Microbiol 35, 697–702.
and microbial susceptibilities variations. Mem Inst Oswaldo Cruz 95,
Tortoli, E., Bartoloni, A., Erba, M. L., Levre`, E., Lombardi, N.,
Mantella, A. & Mecocci, L. (2002). Human infections due to
Saito, H., Murakami, K., Yajima, M., Ishii, N. & Kwon, H. H. (2000).
Mycobacterium lentiflavum. J Clin Microbiol 40, 728–729.
The virulence for mice of newly described mycobacterial species.
Torvinen, E., Suomalainen, S., Lehtola, M. J., Miettinen, I. T.,
Zacheus, O., Paulin, L., Katila, I. T. & Martikainen, P. J. (2004).
Springer, B., Wu, W.-K., Bodmer, T. & 10 other authors (1996).
Mycobacteria in water and loose deposits of drinking water distribu-
Isolation and characterization of a unique group of slowly growing
tion systems in Finland. Appl Environ Microbiol 70, 1973–1981.
European Journal of Anaesthesiology 2007; 24: 568–570r 2007 Copyright European Society of AnaesthesiologyGuidelines for anaesthesiologist specialist training in pain medicineSECTION AND BOARD OF ANAESTHESIOLOGY1, European Union of Medical SpecialistsWorking party on Pain Medicine: A. J. Cunningham*, J. T. A. Knapey, H. Adriaensenz, W. P. Blunniez,E. Buchsery, Z. GoldikJ, W. Ilias**, V. Paver-
PROCESS RESOURCES, INC. PRI 10440 CORPORATE DRIVE • SUGAR LAND, TEXAS 77478 281-240-0955 • FAX 281-240-8025 e-mail: richardtrout@processresources.com PROCESS RESOURCES, INC. AND SUBSIDIARIES STANDARD TERMS AND CONDITIONS OF SALE The equipment, software, materials and services (collectively, the “Equipment”) which are described on the face hereof shall
 Mycobacterium lentiflavum and M. avium co-infection
contaminated bronchoscope, gastric juice and urinesamples (Springer et al., 1996), lymph nodes (Tortoli et al.,1997; Haase et al., 1997), bronchoalveolar lavage fluid and,very recently, sputum (Molteni et al., 2005); the presentreport is to our knowledge the second to demonstratedetection of M. lentiflavum in Brazil. Infection with MACis frequent in Brazilian AIDS patients (Barreto et al., 1993)and because routine identification procedures do not differ-entiate some Mycobacterium species (including M. lenti-flavum) from MAC, use of genetic methods for identifi-cation on a more routine basis would give a better idea of theprevalence of such species in this country.
Mycobacterium lentiflavum and M. avium co-infection
contaminated bronchoscope, gastric juice and urinesamples (Springer et al., 1996), lymph nodes (Tortoli et al.,1997; Haase et al., 1997), bronchoalveolar lavage fluid and,very recently, sputum (Molteni et al., 2005); the presentreport is to our knowledge the second to demonstratedetection of M. lentiflavum in Brazil. Infection with MACis frequent in Brazilian AIDS patients (Barreto et al., 1993)and because routine identification procedures do not differ-entiate some Mycobacterium species (including M. lenti-flavum) from MAC, use of genetic methods for identifi-cation on a more routine basis would give a better idea of theprevalence of such species in this country.