Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Dpi.dipa.co.id
Copyright 2002 by The Endocrine Society
VIII: Meta-Analysis of the Efficacy of Vitamin D Treatment in Preventing Osteoporosis in Postmenopausal Women
EMMANUEL PAPADIMITROPOULOS, GEORGE WELLS, BEVERLEY SHEA, WILLIAM GILLESPIE,BRUCE WEAVER, NICOLE ZYTARUK, ANN CRANNEY, JONATHAN ADACHI, PETER TUGWELL,ROBERT JOSSE, CAROL GREENWOOD, GORDON GUYATT, THE OSTEOPOROSIS METHODOLOGYGROUP, AND THE OSTEOPOROSIS RESEARCH ADVISORY GROUP
are based. The evidence supporting the current guidelines,particularly with respect to the administration of vitamin D,
Objective: To review the effect of vitamin D on bone
is limited. Gillespie et al. (4) have conducted a meta-analysis
density and fractures in postmenopausal women. Data Source: We searched MEDLINE and EMBASE from
addressing the effect of vitamin D on vertebral and nonver-
1966 to 1999 and examined citations of relevant articles and
tebral fractures. This meta-analysis met major methodolog-
proceedings of international meetings. We contacted osteo-
ical criteria: the question was clear and sensible, inclusion
porosis investigators and primary authors to identify addi-
and exclusion criteria were explicit, and the search for studies
tional studies and to obtain unpublished data. Study Selection: We included 25 trials that randomized
The Gillespie et al. meta-analysis is, however, limited in
women to standard or hydroxylated vitamin D with or with-
that it did not address the effect of vitamin D on bone density.
out calcium supplementation or a control and measured
Furthermore, Gillespie et al. took a relatively conservative
bone density or fracture incidence for at least 1 yr.
approach to pooling, and made little use of regression meth-
Data Extraction: For each trial, three independent review-
ods to explore the appropriateness of combining data across
ers assessed the methodological quality and abstracted data.
different forms of vitamin D and variations in study design. Data Synthesis: Vitamin D reduced the incidence of ver-
As a result, the Gillespie study was largely descriptive and
tebral fractures [relative risk (RR) 0.63, 95% confidence in-
permitted few definitive conclusions (4). As part of our series
terval (CI) 0.45– 0.88, P Ͻ 0.01) and showed a trend toward
of systematic reviews of osteoporosis treatment, we therefore
reduced incidence of nonvertebral fractures (RR 0.77, 95% CI
conducted another systematic review to address these lim-
0.57–1.04, P ϭ 0.09). Most patients in the trials that evaluated
itations using the Cochrane methodology. We describe the
vertebral fractures received hydroxylated vitamin D, and
methods of our review in detail in Section I.
most patients in the trials that evaluated nonvertebral frac-tures received standard vitamin D.
Hydroxylated vitamin D had a consistently larger impact
on bone density than did standard vitamin D. For instance,
1. Inclusion criteria. Studies satisfied the following inclusion
total body differences in percentage change between hy-
criteria; 1) participants were women older than 45 yr with
droxylated vitamin D and control were 2.06 (0.72, 3.40) and
absence of menses for a minimum of 6 months; 2) the treat-
0.40 (Ϫ0.25, 1.06) for standard vitamin D. At the lumbar spineand forearm sites, hydroxylated vitamin D doses above 50 g
ment group received some form of vitamin D greater than
yield larger effects than lower doses.
400 IU daily, or some form of dihydroxyvitamin D; 3) a
Vitamin D resulted in an increased risk of discontinuing
follow-up of at least 1 yr; 4) results reported on x-ray evi-
medication in comparison to control as a result of either
dence of fractures of hip, vertebrae, or wrist, or bone mineral
symptomatic adverse effects or abnormal laboratory results
density measured in grams per centimeter or grams per
(RR 1.37, 95% CI 1.01–1.88), an effect that was similar in trials
centimeter squared, by single-photon absorptiometry, dual-
of standard and hydroxylated vitamin D.
photon absorptiometry, or dual x-ray absorptiometry in at
Conclusions: Vitamin D decreases vertebral fractures and
least one of the following sites: femoral neck, total hip, tro-
may decrease nonvertebral fractures. The available data are
chanter, lumbar spine, total body, and the combined forearm,
uninformative regarding the relative effects of standard and
and reporting results on individual patients (as opposed to
number of fractures); 5) the study was designed as a ran-domized control trial (RCT).
We included studies irrespective of whether calcium was
added to vitamin D in the treatment or provided to the
NUMBER OF groups have developed guidelines for
the prevention and treatment of osteoporosis (1–3).
control group. We considered doses of vitamin D of no more
Guidelines are only as strong as the evidence on which they
than 100 IU daily to be negligible, and thus included studiesin which control patients received vitamin D in these lowdoses. We excluded studies that compared different types or
Abbreviations: CI, Confidence interval; RCT, randomized control
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
2. Study search and selection. The structured and tested Co-
early postmenopausal women with bone density in the nor-
chrane Collaborative approach for identifying RCTs, as de-
mal or near normal range (prevention) vs. women with es-
scribed by Dickersin et al. (5) and modified for the Cochrane
Muscular Skeletal Group, guided our MEDLINE and
EMBASE searches. We also conducted hand searches of bib-
liographic references and the Cochrane Controlled Trials
7) level of calcium supplementation (Ͻ500 mg or Ͼ500 mg)
Register and included all references in the Cochrane reviews
6. Statistical analysis. For fractures, we calculated a RR using
update to September 2000 (5). We asked content experts to
methods described by Fleiss (6). We constructed two-by-two
identify published or unpublished relevant RCTs we had
tables for both vertebral and nonvertebral fractures in each
overlooked. Two reviewers (E.P., B.S.) examined each title
study for which the data were available, and calculated the
generated from the search and identified potentially eligible
associated risk ratios. We tested for heterogeneity using a 2
articles for which we obtained the abstracts. For abstracts
procedure (6). We tested whether our a priori hypotheses
consistent with study eligibility, we obtained the full article
could explain variability in the magnitude of treatment ef-
fects across studies using a procedure described by Hedges
3. Methodological quality. We rated the methodological quality
and Olkin (7). For study design, which had the four levels
of each eligible study with respect to concealment of ran-
described above (A, B, C, and D), we used the following
domization; whether patients, caregivers, and those measur-
planned orthogonal contrasts: A vs. [B, C, D]; [B, C] vs. D;
ing outcome were blind to allocation; the extent of loss to
follow-up; and whether the analysis was intention to treat.
We used analytic strategies similar to those for fracture
We used more than one reviewer in the selection of studies,
rates in examining the incidence of side effects and toxicity.
the assessment of methodological quality, and the extraction
For each bone density site (lumbar spine, total body, com-
of data. For all aspects of the review in which raters made
bined hip, and combined forearm), we calculated the
duplicate judgements, they resolved disagreements by
weighted mean difference in bone density between treatment
and control groups using the percentage change from base-line in the treatment and placebo groups and the associated
4. Data collection. Reviewers abstracted data regarding study
sd values. We constructed regression models in which the
design, patient characteristics, treatment duration, dosage,
independent variables were year and dose and the depen-
mean change, and sd values for bone density, and number
dent variable the effect size, and we used this regression to
of vertebral and nonvertebral fractures. For toxicity, we ex-
determine the years across which pooling was appropriate.
amined the rate of withdrawal due to side effects and the rate
To assess whether the magnitude of heterogeneity (differ-
of withdrawal due to investigator-labeled adverse laboratory
ences in apparent treatment effect across studies) was greater
results. On most occasions, the adverse laboratory result
than one might expect by chance, we conducted a test based
was hypercalciuria. We sought key data that were missing
on the 2 distribution with N-1 degrees of freedom, where N
from the original reports through correspondence with the
5. A priori hypotheses regarding heterogeneity. To explore rea-sons for differences in results between studies (heterogene-
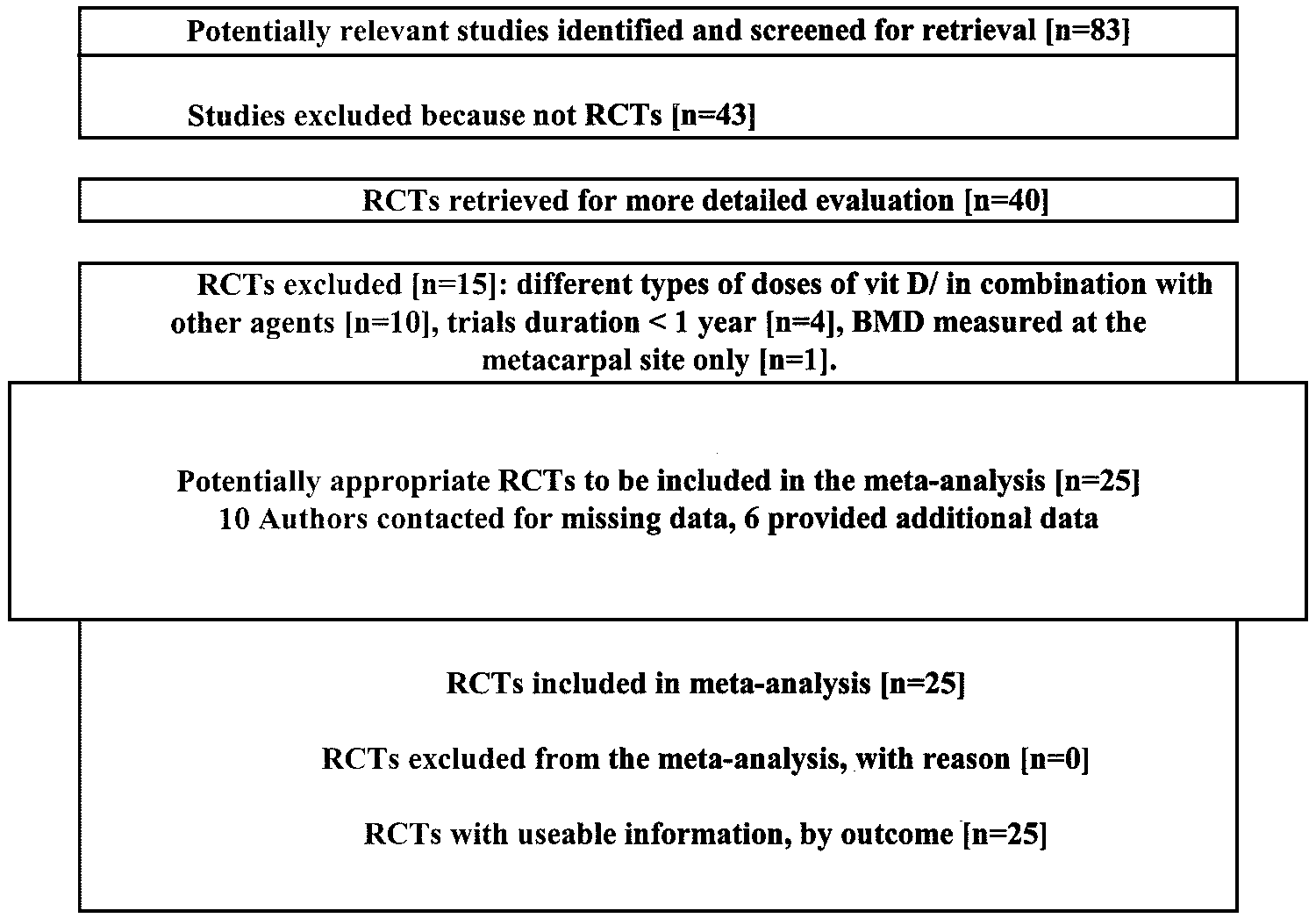
1. Search results. Electronic and hand searching resulted in the
ity), we developed a priori hypotheses relating to the study
retrieval of a total of 83 published papers that addressed the
design, the methodological quality of the study, and the
relationship between vitamin D and bone mineral density or
study population. We describe these hypotheses below:
fracture incidence (Fig. 1). Forty described RCTs (8 – 47). Rea-
1) We identified four study designs; given that calcium
sons for excluding 15 of these trials (33– 47) were: 10 trials
itself increases bone density relative to ordinary diet, we
compared different types or doses of vitamin D, or studied
anticipated that we would see the largest effects with trial
combinations of vitamin D with other agents, without in-
design A, intermediate effects with trial designs B and C, and
cluding a control group that did not receive vitamin D (33–37,
the smallest effect with trial design D.
39 – 43); 4 trials because trial duration was less than 1 yr (38,
A) vitamin D and calcium supplementation vs. normal diet
44 – 46); and 1 trial because bone mineral density was mea-
B) vitamin D alone vs. normal diet
sured at the metacarpal site only (47). Thus, 25 RCTs fulfilled
C) vitamin D combined with calcium supplementation vs.
our eligibility criteria (Table 1) (8 –32).
Of the 25 trials included in this analysis, we had to contact
D) vitamin D alone vs. calcium supplementation
10 authors for additional information (9 –11, 14, 16, 18, 19, 21,
2) whether the experimental intervention was standard
27, 31). Six investigators supplied the information we needed
vitamin D or 25-OH vitamin D on the one hand, or hydroxy-
lated vitamin D (1,25-OH vitamin D or calcitriol) on the other
Table 1 describes these 25 studies in which a total of 4017
patients received some form of vitamin D and 4107 a con-
3) different methodological quality (randomization con-
trolled intervention. Seventeen trials enrolled patients with
cealed or unconcealed; blinded or unblinded; extent of loss
decreased bone density; 10 used some form of standard vi-
to follow-up; intention-to-treat analysis);
tamin D, 14 hydroxylated vitamin D, and 1 trial had both a
4) primary prevention vs. secondary treatment, hypothe-
standard and a hydroxylated vitamin D group in comparison
sizing that the magnitude of the treatment effect may vary in
to a control group (24). Follow-up ranged from 1 to 5 yr; loss
Endocrine Reviews, August 2002, 23(4):560 –569
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
FIG. 1. Search results for calcium/vitamin D review.
to follow-up was less than 10% in two studies, between 10
pooling of years and doses was determined by the regression
and 20% in 8 studies, 20% or greater in 13, and unknown in
analyses described in detail in Section I.
2 trials (10, 27). Eighteen trials were blinded (8, 9, 11–21,
When sample size was adequate, the data showed large,
23–25, 30, 31), 5 trials were not (22, 26, 28, 29, 32), and the
consistent, statistically significant effects of hydroxylated vi-
blinding status was not clear in 2 of the trials (10, 27).
tamin D in all sites for all doses above 0.43 g. The effect ofstandard vitamin D on bone density was consistently much
2. Fractures. Of the 25 eligible studies, 8 (total 1130 patients)
smaller, and reached statistical significance only for lumbar
measured the effect of vitamin D on morphometric vertebral
spine at 1 yr and the femoral neck at final year. The difference
fractures; all but 1 tested hydroxylated vitamin D. Rates of
between standard and hydroxylated vitamin D was statis-
vertebral fractures in the control groups varied from 1% to
tically significant for total body (P ϭ 0.03) and for combined
58%. Figure 2 depicts the results of the individual studies and
forearm (P ϭ 0.01) after the final year of treatment. Figure 4
the pooled estimates of the effect of vitamin D on vertebral
depicts the results for combined forearm.
fractures, and Table 2 summarizes the pooled estimates. The
For three of the analyses, there were large differences in
pooled estimate indicates a 37% reduction in RR (95% CI
results between trials reflected in small P values associated
0.45– 0.88) (Table 2). The point estimates from the individual
with the formal test of heterogeneity. We found a number of
trials are somewhat disparate, although the formal test of
apparent contributing factors (Table 4). We have already
heterogeneity did not reach conventional levels of statistical
noted the differential impact by type of vitamin D. Contrary
significance. None of the factors we identified in advance
to our prediction of little difference between trial designs B
explained the heterogeneity that does exist.
(vitamin D supplementation vs. normal diet) and C (vitamin
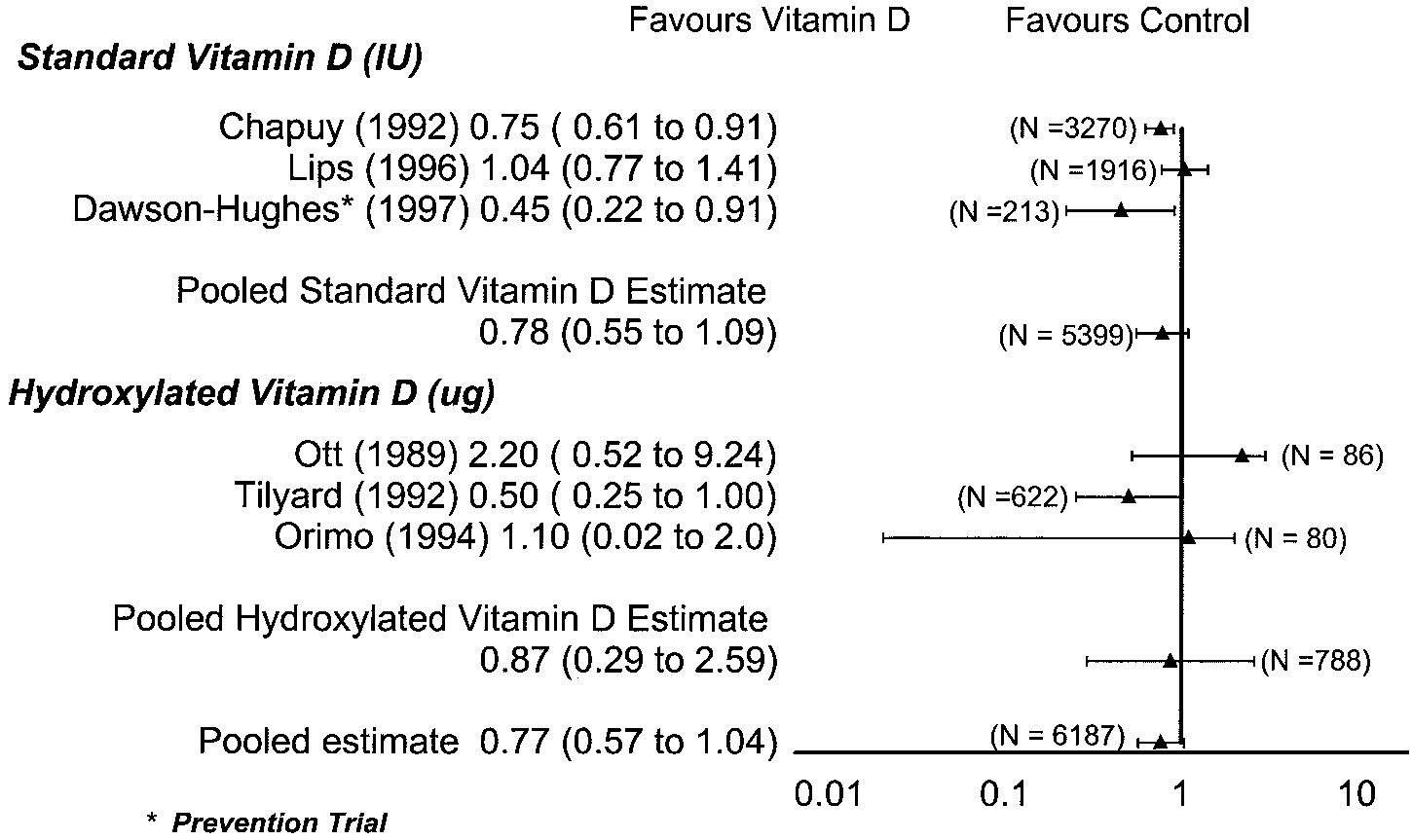
Six studies (a total of 6187 patients) measured the effect of
D and calcium supplementation vs. calcium supplementa-
vitamin D on nonvertebral fractures. Fracture rates in the
tion), the lumbar spine site did show significance. The result
control group varied from 0% to 21%. Studies with standard
was anomalous: standard vitamin D when compared with
vitamin D enrolled far more patients then studies of hy-
regular diet showed a substantial negative effect on bone
droxylated vitamin D (Table 2). The pooled estimate suggests
density, whereas when vitamin D and calcium were com-
a RR reduction of 23%, but the CI includes a RR increase of
pared with calcium alone there was no effect. However, this
4%. The studies show quite disparate results (Fig. 3), al-
result was based upon the comparison of only two trials.
though the CIs are widely overlapping. The test of hetero-
High vs. low levels of calcium supplementation yielded sig-
geneity reaches our threshold for statistical significance for
nificantly different effects for all three analyses presented in
standard vitamin D and the combined results. None of the
Table 4. For hydroxylated doses (0.50 –1.00 g) at the com-
factors we identified in advance, however, explained the
bined forearm sites at yr 1–3, the effect of vitamin D was
greater for patients receiving lower levels of calcium; but for
For both fracture analyses, funnel plots showed no sug-
lumbar spine and total body with standard doses at final
year, the effect was greater for those receiving higher levels
3. Bone density. Table 3 summarizes the impact of vitamin D
of calcium. Intention-to-treat analysis and loss-to-follow-up
on bone mineral density at the four sites we examined. The
results were also statistically significant for total body and
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
300 IU Cholecalciferol vs. placebo
700 IU Cholecalciferol vs. placebo
0.75 g ␣-Hydroxyvitamin D vs.
400 IU Cholecalciferol vs. placebo
400 IU Cholecalciferol vs. placebo
1 g ␣-Calcidiol vs. control (B)
0.5 g ␣-Cacidiol vs. placebo (C)
800 IU Cholecalciferol vs. placebo
0.5 g Calcitriol vs. 1 g calcium
a, Trial design: A ϭ Vitamin D (VD)ϩ Calcium (Ca) vs. Normal Diet (ND); B ϭ VD vs. ND; C ϭ VDϩ Ca vs. Ca; D ϭ VD vs. Ca. b, Data not available/collected.
Endocrine Reviews, August 2002, 23(4):560 –569
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
0.62 g Calcitriol vs. placebo (C)
1600 IU ␣-Calcidial vs. control (C)
0.43 g Calcitriol vs. placebo (C)
1.0 g ␣-Calcidiol vs. control (D)
0.5 g or 1.0 g ␣-Calcidiol vs.
0.5 g ␣-Calcidiol vs. placebo (B)
0.5 g Dihydroxycholecalciferol vs.
0.25 g Dihydroxycholecalciferol vs.
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
FIG. 2. RR with 95% CI for vertebral fractures after treatment with vitamin D.
TABLE 2. Weighted RR with 95% CI after treatment with vitamin D
We interpreted P Յ 0.05 as indicating important between-study differences in results.
FIG. 3. RR with 95% CI for nonvertebral fractures after treatment with vitamin D.
combined forearm bone density. Larger effects were seen in
hydroxylated vitamin D on forearm bone density. One trial,
studies that did conduct an intention-to-treat analysis. The
appreciably larger than the rest, showed a negligible effect of
small number of studies makes inferences from these anal-
hydroxylated vitamin D on forearm bone density. A number
of small trials showed a substantial effect (Fig. 5). Although
For all bone density analyses, we found only one instance
by no means definitively demonstrating publication bias,
suggesting publication bias, the investigation of the effect of
these results do raise the possibility.
Endocrine Reviews, August 2002, 23(4):560 –569
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
TABLE 3. Weighted mean difference of bone density after treatment with vitamin D
FIG. 4. Weighted mean difference of distal forearm after treatment with vitamin D. 4. Side effects and toxicity. Our pooled estimate of the RR of
Two issues of study design are particularly problematic.
discontinuing medication as a result of either symptomatic
First, the methods of supplementation, and the use of cal-
adverse effects or abnormal laboratory results from the 12
cium in addition to vitamin D, vary from study to study. In
trials that reported such events was 1.37 (95% CI 1.01–1.88,
the prior section in this series, we presented a meta-analysis
P value 0.05, heterogeneity P value 0.99). The RR of with-
suggesting that calcium alone increases bone density from
drawal was similar in the trials of standard Vitamin D (RR
1.5% to 2%. We therefore anticipated that we might see
1.40, 95% CI, 0.94 to 2.06, p values 0.10) and hydroxylated
largest effects when the intervention, but not the control
vitamin D (RR 1.34, 95% CI 0.80 –2.24, P value 0.27), respec-
group, received calcium in addition to vitamin D. We ex-
tively (P value on the difference between the two estimates
pected intermediate effects when calcium was withheld
from, or offered to, both treatment and control groups, and
smallest effects when calcium was given to only the controlarm.
Inferences from the results of these analyses are limited by
The fracture data revealed quite a different pattern: the
the variability in study designs, methodological weaknesses
largest effect and most precise estimate of vitamin D effect
in the primary studies (including lack of blinding in many
on fracture came from a study in which only the control
studies), the paucity of data, and the inconsistency of results.
group received calcium (21). Similarly, we failed to see the
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
expected pattern in our examination of heterogeneity of find-
ings in studies of bone density (Table 4). These puzzling
results highlight the uncertainties regarding the effects of
vitamin D that the studies to date have not resolved.
The second major issue in the possibility that vitamin D
will have a different impact in different populations. We
could not explore this issue adequately because studies typ-
ically did not record baseline levels of vitamin D, the most
likely explanation of heterogeneity of treatment effect across
The variability in study results further limits any infer-
ences one can make on the basis of the studies to date. We
found statistically significant heterogeneity not only in a
number of our bone density analyses, but also in the analysis
of the effect of standard vitamin D, and the pooled analysis
of all formulations, on nonvertebral fractures. Our a priori
hypotheses failed to adequately explain this variability.
Nevertheless, combining across all trials, we found a sig-
nificant effect of vitamin D in reducing vertebral fractures
and a trend toward reduction in nonvertebral fractures (Ta-
ble 2 and Figs. 2 and 3). The case for a biological mechanism
for the vitamin D effect gains some strength from our anal-
ysis of bone density, which suggested a positive impact on
bone density at every site, particularly with hydroxylated
The biology of standard and hydroxylated vitamin D is
sufficiently different that one might be reluctant to pool in the
first place (48). Both forms showed a similar effect on frac-
tures. However, the confidence intervals around these effects
are extremely wide, and it is quite possible that true effects
differ greatly. Thus, the available data provide little guidance
on the choice of vitamin D formulation.
In summary, secure inferences from the available random-
ized trials of vitamin D are very limited. Vitamin D formu-
lations probably reduce vertebral fractures. Their impact on
nonvertebral fractures is uncertain. Moreover, the relative
impact of different formulations on fracture rates, and the
extent to which vitamin D effects vary in different popula-
tions, is extremely uncertain. These issues offer potentially
fruitful questions for subsequent investigation.
1. 1996 AACE Clinical practice guidelines for the prevention and
treatment of postmenopausal osteoporosis. J Fla Med Assoc 83:
2. Kanis JA, Delmas P, Burckhardt P, Cooper C, Torgerson D 1997
Guidelines for diagnosis and management of osteoporosis. The
Endocrine Reviews, August 2002, 23(4):560 –569
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
European Foundation for Osteoporosis and Bone Disease. Osteo-
controlled 2-year study in 315 normal females. Eur J Clin Invest
3. Scientific Advisory Board, Osteoporosis Society of Canada 1996
25. Geusens P, Dequeker J 1986 Long-term effect of nandrolone de-
Clinical practice guidelines for the diagnosis and management of
canoate, 1␣ hydroxyvitamin D3, or intermittent calcium infusion
osteoporosis. Scientific Advisory Board, Osteoporosis Society of
therapy on bone mineral content, bone remodeling and fracture
rate in symptomatic osteoporosis: a double-blind controlled study.
4. Gillespie WJ, Henry DA, O’Connell DL, Robertson J 1999 Vita-
min D and vitamin D analogues for preventing fractures associated
26. Shiraki M, Orimo H, Ito H, Akiguchi I, Nakao J, Takahashi R,
with involutional and post-menopausal osteoporosis. Cochrane
Ishizuka S 1985 Long-term treatment of postmenopausal osteo-
porosis with active vitamin D3 1-␣-hydroxycholecalciferol and 1,24
5. Dickersin K, Scherer R, Lefebvre C 1994 Identifying relevant
dihydroxycholecalciferol. Endocrinol Jpn 32:305–315
studies for systematic reviews. BMJ 309:1286 –1291
27. Orimo H, Shiraki M, Hayashi T, Nakamura T 1987 Reduced
6. Fleiss JL 1993 The statistical basis of meta-analysis. Stat Methods
occurrence of vertebral crush fractures in senile osteoporosis
treated with 1␣-vitamin D3. Bone Miner 3:47–52
7. Hedges LV, Olkin I 1985 Statistical methods for meta-analysis. San
28. Komulainen M, Kroger H, Tuppurainen MT, Heikkinen AM, Alhava E, Honkanen R, Jurvelin J, Saarikoski S 1999 Prevention
8. Baeksgaard L, Anderson KP, Hyldstrup L 1998 Calcium and vi-
of femoral and lumber bone loss with hormone replacement ther-
tamin D supplementation increase spinal BMD in healthy post-
apy and vitamin D3 in early postmenopausal women: A popula-
menopausal women. Osteoporos Int 8:255–260
tion-based 5-year randomized trial. J Clin Endocrinol Metab 84:
9. Chapuy MC, Arlot ME, Duboeuf F, Brun J, Crouzet B, Arnaud S, Delmas PD, Meunier PJ 1992 Vitamin D3 and calcium to prevent
29. Shiraki M, Orimo H 1991 The effect of estrogen, and sex-steroids
hip fractures in elderly women. N Engl J Med 327:1637–1642
and thyroid hormone preparation on bone mineral density in senile
10. Christiansen C, Christiansen MS, Rodbro P, Hagen C, Transbol
osteoporosis: a comparative study of the effect of 1␣-hydroxy-
I 1981 Effect of 1,25-dihydroxy-vitamin D3 in itself or combination
cholecalciferol on senile osteoporosis. Nippon Naibunpi Gakkai
with hormone treatment in preventing postmenopausal osteopo-
30. Caniggia A, Delling G, Nuti R, Lore F, Vattimo A 1984 Clinical,
11. Dawson-Hughes B, Dallal GE, Krall EA, Harris S, Sokoll LJ,
biochemical and histological results of a double-blind trial with
Falconer G 1991 Effect of vitamin D supplementation on winter-
1,25-dihydroxyvitamin D3, estradiol and placebo in post-meno-
time and overall bone loss in healthy postmenopausal women. Ann
pausal osteoporosis. Acta Vitaminol Enzymol 6:117–128
31. Thomsen K, Riis B, Christiansen C 1986 Effect of estrogen/ge-
12. Gallagher JC, Goldgar D 1990 Treatment of postmenopausal os-
stagen and 24R, 25-dihydroxyvitamin D3 therapy on bone forma-
teoporosis and high doses of synthetic calcitriol. Ann Intern Med
tion in postmenopausal women. J Bone Miner Res 1:503–507
32. Chen JT, Shiraki M, Hasumi K, Tanaka N, Katase K, Kato T, Hirai
13. Jensen GF, Christiansen C, Transbol I 1982 Treatment of post- Y, Nakamura T, Ogata E 1997 1-␣ Hydroxyvitamin D3 treatment
menopausal osteoporosis. A controlled therapeutic trial comparing
decreases bone turnover and modulates calcium-regulating hor-
oestorogen/gestgen, 1,25-dihydroxy-vitamin D3 and calcium. Clin
mones in early postmenopausal women. Bone 20:557–562
33. Falch JA, Odegaard OR, Finnanger AM, Matheson I 1987 Post-
14. Lips P, Wilco C, Graafmans MS, Ooms ME, Bezemer PD, Bouter
menopausal osteoporosis: no effect of three years treatment with
LM 1996 Vitamin D supplementation and fracture incidence in
1,25-dihydroxycholecalciferol. Acta Medica Scand 221:199 –204
elderly persons. Ann Intern Med 124:400 – 406
34. Arthur RS, Piraino B, Candib D, Cooperstein L, Chen T, West C,
15. Menczel J, Foldes J, Steinberg R, Leichter I, Shalita B, Bdolah- Puschett J 1990 Effect of low-dose calcitriol and calcium therapy on Abram T, Kadosh S, Mazor Z, Ladkani D 1994 Alfacalcidol (␣D3)
bone histomorphometry and urinary calcium excretion in osteo-
and calcium in osteoporosis. Clin Orthop 300:241–247
porotic women. Miner Electrolyte Metab 16:385–390
16. Ooms ME, Roos JC, Bezemer PD, van der Vijgh WJ, Bouter LM,
35. Lyritis GP, Androulakis C, Magiasis B, Charalambaki Z, Tsakala- Lips P 1995 Prevention of bone loss by vitamin D supplementation kos N 1994 Effect of nandrolone decontae and 1-␣-hydroxy-
in elderly women: a randomized double-blind trial. J Clin Endo-
calciferol on patients with vertebral osteoporosis collapse: a dou-
ble-blind clinical trial. Bone Miner 27:209 –217
17. Orimo H, Shiraki M, Hayashi Y, Hoshino T, Onaya T, Miyazaki
36. Eriksson SA, Lindgren JU 1993 Combined treatment with calci- S, Kurosawa H, Nakamura T, Ogawa N 1994 Effects of 1␣-
tonin and 1,25-dihydroxyvitamin D3 for osteoporosis in women.
hydroxyvitamin D3 on lumbar bone mineral density and vertebral
fractures in patients with postmenopausal osteoporosis. Calcif Tis-
37. Caniggia A, Lore F, Nuti R, Martini G, Frediani B, DiCairano G
1992 Role of the active vitamin D metabolite and 1␣-hydroxylated
18. Orwoll ES, McClung MR, Oviatt SK, Recker RR, Weigel RM 1989
analogs in the treatment of postmenopausal osteoporosis. J Nutr Sci
Histomorphometric effects of calcium or calcium plus 25-
hydroxyvitamin D3 therapy in senile osteoporosis. J Bone Miner
38. Gallagher JC, Jerpbak CM, Jee WSS, Johnson KA, DeLuca HF, Riggs BL 1982 1,25-Dihydroxyvitamin D3: short- and long-term
19. Ott SM, Chesnut III CH 1989 Calcitriol treatment is not effective
effects on bone and calcium metabolism in patients with post-
in postmenopausal osteoporosis. Ann Intern Med 110:267–274
menopausal osteoporosis. Proc Natl Acad Sci USA 79:3325–3329
20. Riis BJ, Thomsen K, Christiansen C 1986 Does 25R,25(OH)2-
39. Masud T, Mulcahy B, Thompson AV, Donnelly S, Keen RW,
vitamin D3 prevent postmenopausal bone loss? Calcif Tissue Int
Doyle DV, Spector TD 1998 Effects of cyclical etidronate combined
with calcitriol versus cyclical etidronate alone on spine and femoral
21. Tilyard MW, Speanrs GF, Thomsen J, Dovey S 1992 Treatment of
neck bone mineral density in postmenopausal osteoporotic
postmenopausal osteoporosis with calcitriol or calcium. N Engl
40. Aloia JF, Vaswani A, Yeh JK, Ellis K, Yasumura S, Cohn SH 1988
22. Ushiroyama T, Okamura S, Ikeda A, Ueki M 1995 Efficacy of
Calcitriol in the treatment of postmenopausal osteoporosis. Am J
ipriflavone and 1␣ vitamin D therapy for the cessation of vertebral
bone loss. Int J Gynecol Obstet 48:283–288
41. Aloia JF, Vaswani A, Yeh JK, Ross PL, Flaster E, Dilmanian A 1994
23. Dawson-Hughes B, Harris S, Krall E, Dallal GE 1997 Effect of
Calcium supplementation with and without hormone replacement
calcium and vitamin D supplementation on bone density in men
therapy to prevent postmenopausal bone loss. Ann Intern Med
and women 65 years of age or older. N Engl J Med 337:670 – 676
24. Christiansen C, Christiansen M, McNair P, Hagen C, Stocklund
42. Recker RR, Davies KM, Dowd RM, Heaney RP 1999 The effect of K, Trasnbol IB 1980 Prevention of early postmenopausal bone loss:
low-dose continuous estrogen and progesterone therapy with cal-
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
cium and vitamin D on bone in elderly women: a randomized,
1983 Calcium, vitamin D and anabolic steroid in treatment of aged
controlled trial. Ann Intern Med 130:897–904
bones: double-blind placebo-controlled long-term clinical trial. Age
43. Dawson-Hughes B, Harris SS, Krall EA, Dallal GE, Falconer G, Green CL 1995 Rates on bone loss in postmenopausal women
46. Veijo Hoikka, EM, Alhava AA, Paavo K, Veikko R 1980 Treatment
randomly assigned to one of two dosages of vitamin D. Am J Clin
of osteoporosis with 1-␣-hydroxycholecalciferol and calcium. Acta
44. Grady D, Halloran B, Cummings S, Leveille S, Wells L, Black D,
47. Nordin BE, Baker MR, Horsman A, Peacock M 1985 A prospective Byl N 1991 1,25-Dihydroxyvitamin D3 and muscle strength in
trial of the effect of vitamin D supplementation on metacarpal bone
elderly: a randomized controlled trial. J Clin Endocrinol Metab
loss in elderly women. Am J Clin Nutr 42:470 – 474
48. DeLuca HF 1988 The vitamin D story: a collaborative effort of basic
45. Inkovaara J, Gothoni G, Halttula R, Heikinheimo R, Tokola O
science and clinical medicine. FASEB J 2:224 –236
Behavioral Interview Techniques – The STAR Approach Situation or Describe the situation that you were in or the task that you needed to accomplish. You must describe a specific event or situation, not a generalized description of what you have done in the past. Be sure to give enough detail for the interviewer to understand. This situation can be from a previous job, from a volunteer ex
JETTI KATZ TROPICAL MEDICINE LAB TEST REQUISITION AND PRICE LIST Patient Name:________________________________ Purged: Non Purged: $ 400.00 Routine O/P Stool: Macroscopic and microscopy exam of stool for routine Protozoa and all Helminths, plus Entamoeba Histolytica Stool Antigen by E.I.A. and Giardia Stool Antigen by E.I.A. $ 670.00 Panel 1 Stool Test: Includes all test
 Endocrine Reviews, August 2002, 23(4):560 –569
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
FIG. 1. Search results for calcium/vitamin D review.
Endocrine Reviews, August 2002, 23(4):560 –569
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
FIG. 1. Search results for calcium/vitamin D review.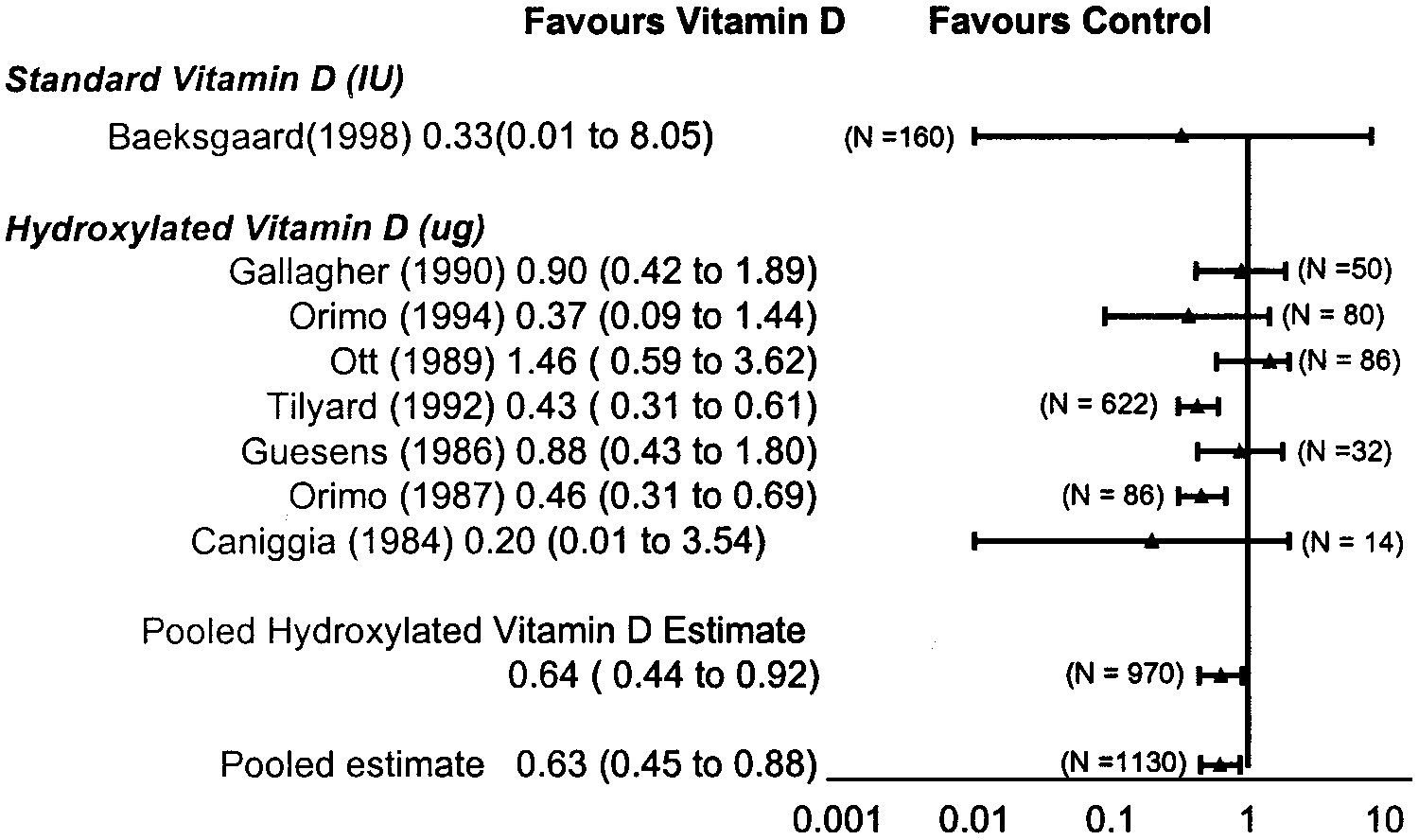
 Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
FIG. 2. RR with 95% CI for vertebral fractures after treatment with vitamin D.
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
FIG. 2. RR with 95% CI for vertebral fractures after treatment with vitamin D.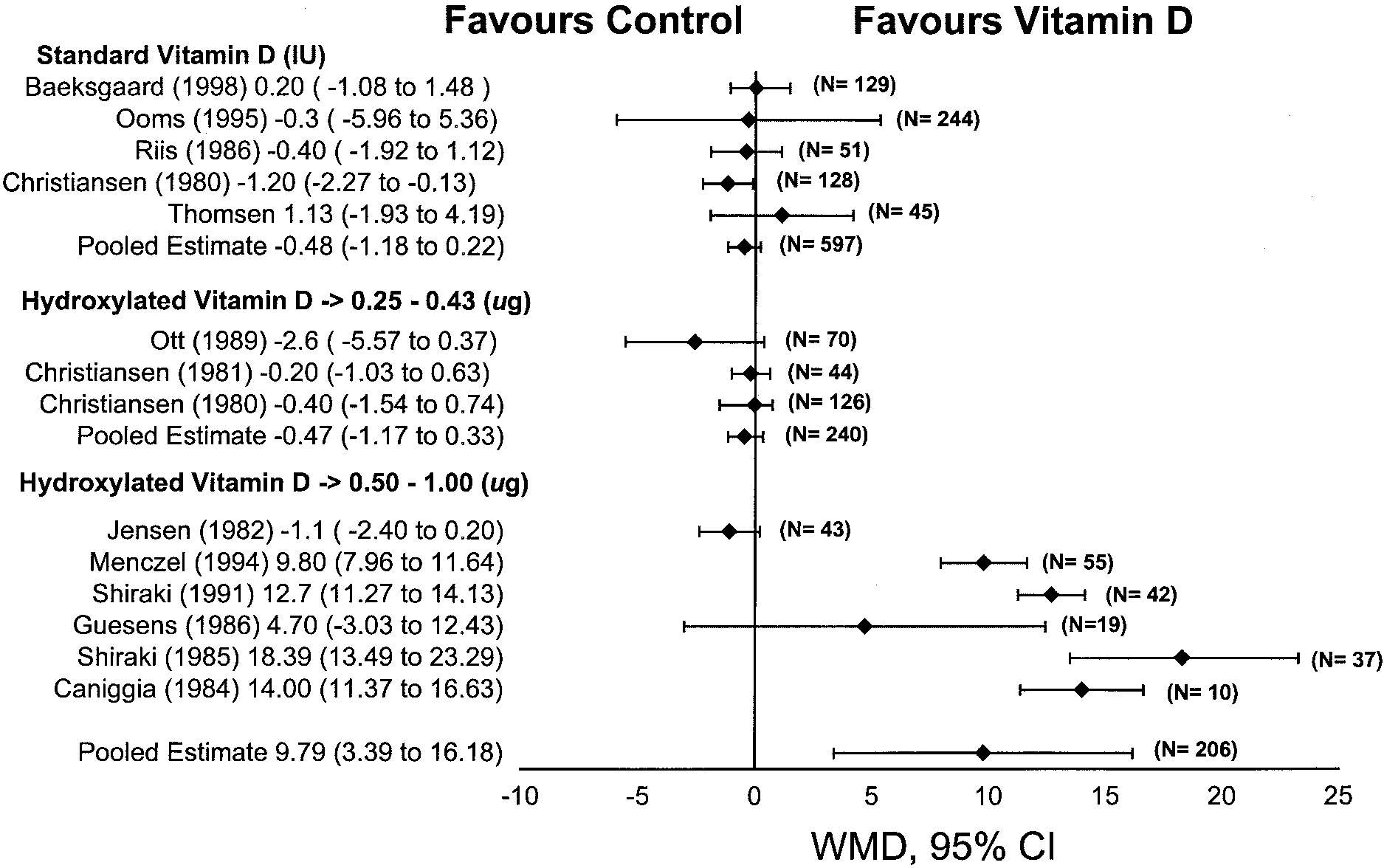 Endocrine Reviews, August 2002, 23(4):560 –569
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
TABLE 3. Weighted mean difference of bone density after treatment with vitamin D
FIG. 4. Weighted mean difference of distal forearm after treatment with vitamin D.
Endocrine Reviews, August 2002, 23(4):560 –569
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
TABLE 3. Weighted mean difference of bone density after treatment with vitamin D
FIG. 4. Weighted mean difference of distal forearm after treatment with vitamin D.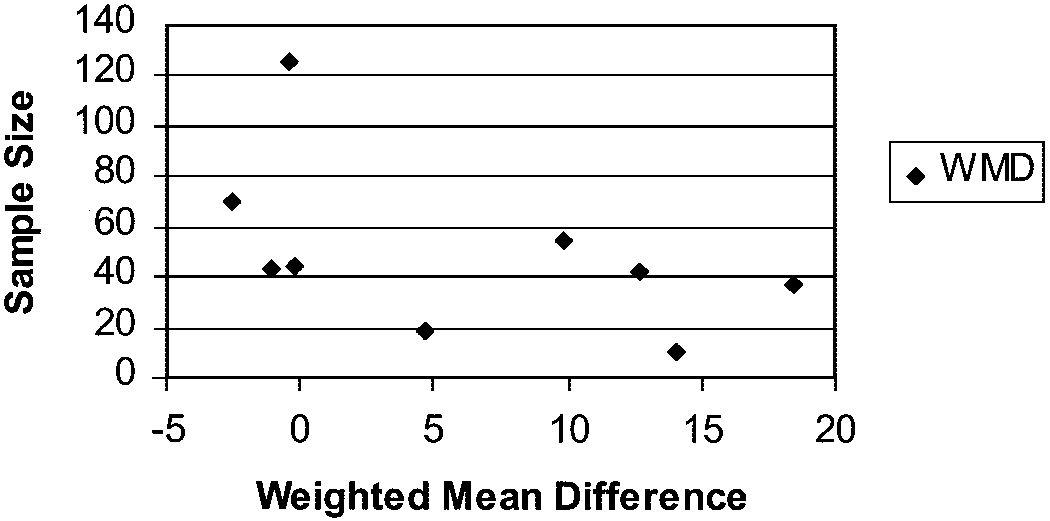 Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
expected pattern in our examination of heterogeneity of find-
ings in studies of bone density (Table 4). These puzzling
results highlight the uncertainties regarding the effects of
vitamin D that the studies to date have not resolved.
Guyatt et al. • Meta-Analyses of Osteoporosis Therapies
Endocrine Reviews, August 2002, 23(4):560 –569
expected pattern in our examination of heterogeneity of find-
ings in studies of bone density (Table 4). These puzzling
results highlight the uncertainties regarding the effects of
vitamin D that the studies to date have not resolved.