Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Doi:10.1016/s0195-5616(03)00052-4
Craig Webb, DVM, PhD*, David C. Twedt, DVM
College of Veterinary Medicine and Biomedical Sciences, Colorado State University,
Gastritis—inflammation of the stomach—is a frequently cited differential
yet rarely characterized diagnosis in cases of canine anorexia and vomit-ing. Although the list of rule-outs for acute or chronic gastritis is extensive(Box 1) [1], a review of the veterinary literature reveals fewer than 15 articlesthat have focused on clinical cases of canine gastritis over the last 25 years[2–14]. The dog frequently appears in the human literature as an ex-perimentally manipulated model for the study of endoscopic techniques orthe effect of medications on gastric mucosa [15–20]. In the veterinarypatient, cases of acute gastritis are rarely pursued with the complete di-agnostic armamentarium, and cases of chronic gastritis are rarely found tooccur as an entity isolated from the rest of the gastrointestinal tract. Thisarticle focuses on those findings most clinically relevant to cases of caninegastritis in veterinary medicine.
The mucosal lining of the stomach normally acts as an effective defensive
barrier against acidity, detergents, bacteria, and changes in temperature. That mucosal defense consists of secretions, cells, and blood. Normal gastricsecretions represent the first line of defense and include acid, mucus,bicarbonate, and antibacterial substances. The gastric epithelium serves asa barrier to the back-diffusion of acid and is quickly repaired by restitutionafter injury. The gastric microvasculature is exquisitely responsive to neu-ronal, hormonal, and inflammatory signals. This blood supply is central tothe maintenance of gastric mucosal integrity, the elimination of noxioussubstances, and gastric epithelial turnover [21–23]. Macrophages and mastcells are part of the innate immune system that coordinates the gastric
* Clinical Sciences Department, Colorado State University, 300 West Drake Road, Fort
0195-5616/03/$ - see front matter Ó 2003 Elsevier Inc. All rights reserved. doi:10.1016/S0195-5616(03)00052-4
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
Box 1. Differential diagnosis for cases of acute or chronicgastritis in dogs
Basenji, Norwegian Lundehund (atrophic gastritis)
Dietary indiscretion, foreign bodiesDrugs
Nonsteroidal anti-inflammatory drugs (NSAIDs),
corticosteroids, antibiotics, chemotherapeutics
Eosinophilic gastritisFood allergy, food sensitivityGranulomatous gastritis
Idiopathic, infectious, neoplasia, foreign body, systemic
Immune-mediated gastritisInfectious gastritis
Lymphocytic/plasmacytic gastritisMotility disorders, reflux disease
NeoplasiaParasitic gastritisSecondary gastritis (systemic disease)
Central nervous system disease, renal failure, liver failure,
inflammatory response when challenged by antigenic stimulation [24]. Finally, like much of the gastrointestinal tract, the gastric mucosa has a largecapacity for quickly repairing damaged tissue (ie, restitution of ulceratedmucosal epithelium) [25].
In cases of excessive or inappropriate gastric inflammation, although
a cause or causative agent is rarely determined, many of the pathologicchanges have been elucidated [26,27]. Chemical injury, ischemia, infection, orantigens can stimulate the release of inflammatory mediators and vasoactivecompounds from a variety of cell types (eg, neutrophils, mast cells, platelets,endothelial cells, neurons) (Box 2) [28,29]. Subsequent exfoliation of surfacegastric epithelial cells and disruption of the normal mucosal barrier result inback-diffusion of gastric acid, pepsin, and gastric lipase. This inflammatorycascade stimulates further acid secretion and mucosal damage, increases cellmembrane permeability, and alters microvascular blood flow. The continuedinterplay between ischemia and inflammation results in gastric erosion,ulceration, hypoxia, hemorrhage, edema, and necrosis [30].
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
Box 2. Inflammatory and vasoactive mediators of gastritis
Endothelin-1HistamineNitric oxideNeuropeptides
Calcitonin gene-related peptideSubstance P
‘‘Garbage gut’’ is a catch-all diagnosis for cases of acute gastritis, where
dogs are likely to have ingested actual garbage, molds, fungi, spoiled or rawfood, leftovers, or cat litter. Beyond the radiographic demonstration of gastricdistention secondary to overindulgence, these cases are infrequently subjectedto extensive diagnostic effort. These patients usually respond to a brief periodof gastric inactivity and dietary counseling, although acute pancreatitis isa serious potential sequela. Persistent or repeat offenders should be examinedfor causes of polyphagia and pica (eg, malnourishment, maldigestion,malabsorption, hyperadrenocorticism, behavioral issues). Outbreaks of foodpoisoning such as are periodically seen in the human population seem to beeither rare or underappreciated events in our canine companions.
Foreign bodies may cause direct physical damage to the mucosal barrier
on their way through, or they may lodge in the pylorus, resulting in acutegastritis, vomiting, gastric ulceration, and biochemical changes consistentwith an upper gastrointestinal obstruction. The diagnosis can be straightfor-ward when the foreign object is radiographically distinct; however, thepylorus can be a difficult region to elucidate, and tumors, pyloric hyper-plasia or stenosis, and gastric atony must be considered on the list ofdifferentials. Progression of the disease, repeat radiographic images, con-trast studies, or ultrasound examination may provide additional clues in
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
cases of acute gastritis that do not respond to conservative management asanticipated. Uncomplicated cases of acute gastritis should resolve withoutthe use of antiemetics, H2-receptor blockers, or gastrointestinal protectants,and their indiscriminant use may mask symptoms that would otherwiseprompt a more in-depth examination of the patient.
The onset of gastrointestinal symptoms related to the ingestion of specific
food items, where the underlying mechanism is an immune-mediatedreaction, defines a food allergy. Pruritus rather than gastritis is the mostcommon clinical sign of a food allergy, and the stomach may not bethe portion of the gastrointestinal tract most commonly afflicted. In fact,gastrointestinal symptoms may be present in only 10% to 15% of cases ofcanine food allergy, although up to 50% of cats with chronic idiopathicgastrointestinal symptoms may respond to manipulation of the dietaryprotein source [31].
In many cases, human beings diagnosed as being allergic to certain foods
are also found to be suffering from Helicobacter pylori infection, compli-cating the interpretation of gastric pathologic findings [32]. In children withconfirmed cases of food allergy, a close relation was found to duodenalpathologic findings, whereas no significant association was seen with gastriclesions [33]. A similar lack of gastric pathologic findings was demonstratedin human adults suffering from food allergies without concurrent H pyloriinfection [34]. Proteins are the foodstuff most commonly incriminatedin food-allergic dogs, and the gastric mucosa is not normally a site ofabsorption for these polypeptides (Box 3). The age of onset can be anywherebetween puppy and adulthood, although many reports identify a significantnumber of young animals (\1 year of age).
The pathophysiology of a food-allergic reaction is complex and not yet
completely understood. The adverse response may involve immediate,delayed, or mixed hypersensitivity reactions as well as multiple inflamma-tory cells and mediators. Gut-associated lymphoid tissue can present intactmaterial to the host immune system through specialized gastrointestinalantigen-presenting cells, M cells, and macrophages. IgA-producing B cells,IgE antibodies, helper T cells, eosinophils, and mast cells are all located inthe lamina propria of the digestive tract as potential contributors to theantigen-driven response. Histamine, serotonin, vasoactive intestinal poly-peptide, proteinases, prostaglandins, leukotrienes, and interleukins are justa few of the inflammatory mediators released by the complex interplay ofthe various cell types present [35–37].
Ideally, the diagnosis of a food allergy would include identification of the
offending antigen; demonstration of the correlation between antigenexposure, clinical signs, and pathologic changes; and elucidation of theimmunologic mechanism. If the symptoms are eliminated in response to anappropriate diet trial, it should be demonstrated that they reappear with thesubsequent reintroduction of the incriminated antigen—a diagnostic stepusually declined by owners.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
Box 3. Foodstuffs thought to induce an adverse immuneresponse in the dog
Commercial dog foodsBeefKidney beansFlavoringsMuttonCorn
PorkSoyPreservativesChickenRiceSupplementsHorsePotatoDyesRabbitMaize
In contrast, food intolerance is a nonimmune, idiosyncratic, physiologic,
metabolic, or toxic response to a food item. Symptoms of food intolerancemay mimic any abnormal gastrointestinal reaction; therefore, it isa particularly difficult condition to diagnose [37]. Food intolerance maybe the result of a deficiency in a specific digestive enzyme, with the mostoften cited example being lactose intolerance secondary to a deficiency in theenzyme lactase.
More than 30 varieties of plants and innumerable household chemicals
are potential causes of canine gastritis (Box 4) [1]. Although not a toxin byitself, the urease activity of H pylori is in part responsible for the patho-genicity of this organism in people. Many plants contain the same enzyme,which may contribute indirectly to their role in gastritis [38]. Chemicals maybe directly caustic to the gastric mucosa or may affect gastric function(ie, increased acid secretion, decreased bicarbonate secretion, change inmotility) and result in secondary inflammation.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
Box 4. Common household plants and chemicals associatedwith gastritis
DaffodilEthylene glycolMushroomsDeodorantsIvyDetergents
NitratesRhododendronHeavy metalsPoinsettia
HollyBleachHoneysucklePine oilMistletoeRubbing alcoholJasmineDriveway salt
NSAIDs are one of the most common causes of acute gastric erosion and
chronic gastric ulceration leading to hospitalization and even death inhuman beings [39]. These compounds work by blocking the conversionof arachidonic acid into inflammatory mediators via the cyclooxygenase(COX) enzyme. Despite the advent of NSAIDs manufactured specificallyfor veterinary patients (eg, carprofen [Rimadyl], etodolac [Etogesic]), the useof aspirin is still commonplace for dogs with occasional stiffness or chronicosteoarthritis. Ibuprofen, acetaminophen, and indomethacin are othercommon over-the-counter NSAIDs administered by owners or ingested byopportunistic pets [40,41]. The depletion of endogenous protective prosta-glandins, a decrease in mucus and bicarbonate secretions, a disruption of theepithelial cell layer, a reduction of the surface epithelial cell hydrophobicity,a reduction in mucosal blood flow, an increase in neutrophil adherence, anddirect mucosal injury are all components of the deleterious effects ofNSAIDs on the gastric mucosa [42,43]. The antrum and pylorus are theportions of the stomach most susceptible to NSAID-induced lesions. Thoselesions can range from surface erythema to erosions to full-thicknessulcerations [44]. The greater the severity of mucosal damage, the greater isthe volume of blood entering the gastric lumen and the more likely it is thathematemesis or melena is part of the presenting complaint.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
Because of the prevalence of NSAID-induced gastric ulceration, the
development of increasingly specific COX-2 inhibitors has burgeoned intoa multibillion dollar pharmaceutic industry, and COX-2 selective inhibitorsare now some of the most frequently prescribed drugs in human medicine[45]. The theory behind the use of COX-2 inhibitors is illustrated in Fig. 1[46]. Although not entirely COX-2 selective, Rimadyl and Etogesic are twoNSAIDs approved for use in dogs and designed to reduce ulcer formationrelative to aspirin. Endoscopic examination used to compare the gastricmucosa of dogs given aspirin with that of dogs treated with etodolac foundthat dogs given aspirin invariably had mucosal erosions by day 17 oftreatment, whereas none of the dogs given etodolac were found to have anygastric lesions [47]. Regardless of the NSAID administered, none of the dogsin this study were found to have any biochemical abnormalities, vomiting,anorexia, or melena. Other similar studies have confirmed the ubiquity ofgastric lesions in dogs receiving aspirin as well as illustrating only the mostminor changes in dogs receiving either etodolac or carprofen [48,49].
Interestingly, the COX selectivity of these NSAIDs seems to depend in
part on the specific assay conditions used to determine the COX-2/COX-1ratio. Using an in vitro canine monocyte/macrophage cell line, carprofenwas found to be only 1.75 times more active against COX-2 than COX-1[50]. In a separate study using an enzymatic assay, carprofen inhibitedcanine COX-2 activity 100 times more effectively than COX-1 activity [51]. Regardless of the molecular mechanism of action, both carprofen andetodolac seem to be significantly less ulcerogenic than aspirin.
New and more specific COX-2 inhibitors are being continually developed
and made available to the veterinary practitioner. For example, deracoxib(Deramaxx) is a recently released NSAID designed to act as a specific
Fig. 1. Function of prostaglandin products formed from arachidonic acid through cyclo-oxygenase COX-1 and COX-2 enzymatic pathways.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
COX-2 antagonist. Novartis claims the in vitro COX-1/COX-2 IC50 (amountof drug required to inhibit 50% of enzyme activity) ratio is 1275, consistentwith a COX-2 specific medication. Deracoxib is approved by the US Foodand Drug Administration (FDA) for use in dogs to help controlpostoperative pain after orthopedic procedures. The manufacturer reportsno gastrointestinal, renal, or hepatic toxicity and no blood clottingabnormalities or drop in plasma protein. At the time of publication, noinformation was available regarding the use of Deramaxx in clinical cases. Despite the theoretic advantages of COX-2 inhibitors, this class of drug isnot without potential side effects and should not be prescribed withoutappropriate client education [46,52,53].
In addition to NSAIDs, corticosteroids, antibiotics, and chemothera-
peutics are potential causes of acute gastritis, anorexia, and vomiting. Thedeleterious mechanisms behind bouts of gastritis induced by these med-ications remain unclear (ie, direct mucosal injury, alterations in gastric pH,stimulation of innate immunity) and seem to be highly variable and hostdependent. Corticosteroids decrease and alter the composition of gastricmucus and decrease mucosal cell turnover. The association betweendexamethasone therapy and melena has been appreciated for some time,and the combination of corticosteroids and NSAIDs creates an extremelyulcerogenic gastric environment [54]. Gastric lesions can appear as soon as36 hours after dexamethasone administration alone [55].
Mycotic gastritis has been rarely reported (ie, pythiosis), and the acidic
environment of the empty stomach is usually free of bacteria. Salmonellaspp, Campylobacter jejuni, and Clostridium perfringens are differentials forgastroenteritis, with diarrhea as the most common presenting complaint,and are not discussed further in this article [56]. H pylori is a well-establishedcause of chronic gastritis and gastric ulceration in people, but whether thesespiral-shaped organisms play a role in the pathologic changes of caninegastritis remains to be established [57,58]. A variety of Helicobacter spp(although not H pylori) [59,60] can be found in the stomachs of upward of80% of dogs whether they are vomiting or not [61–63]. The possible modesof transmission may include fecal-oral, oral-oral, water-borne infection,or through nursing. Urease production, cytology, histopathology, culture,serology, and polymerase chain reaction (PCR) analysis can be used todiagnose Helicobacter infection, but in most naturally infected dogs, thesespecies seem to cause no clinically significant change in gastric physiology orfunction [63,64]. In addition, one treatment regimen commonly used in casesof human H pylori gastritis (the combination of amoxicillin, metronidazole,and famotidine) proved effective at suppressing canine gastric Helicobacterinhabitants for only a brief period of time [64,65]. The differences inHelicobacter spp pathogenicity between people and dogs may be related to
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
differences in the infective Helicobacter species themselves or to differencesin the host immune response to the infective organisms. In fact, some casesof gastritis in dogs with Helicobacter spp do respond favorably to treatmentdirected at this organism. Although Helicobacter spp can readily be found inthe stomachs of vomiting dogs, it would seem unwise to cite that discoveryas reason for ending the search for cause in cases of canine gastritis [66].
Pathogenic enteric viruses in dogs include parvovirus, distemper virus,
rotavirus, and coronavirus. Gastritis is rarely the primary concern in thesediseases, with intestinal or systemic involvement being most responsiblefor patient morbidity and mortality. Parvovirus, in particular, is an on-going area of active research, and the reader is referred to a review on thesubject [67].
The incidence of canine gastric ulcer disease are undetermined. Although
vomiting and anorexia would be the expected symptoms of this condition,human gastric ulcer disease can remain clinically ‘‘silent’’ for a substantialperiod during the progression of the disease.
The cause of gastric ulcer formation is most likely multifactorial, in-
volving mucosal, vascular, endocrine, and neurologic variables. For ex-ample, stress is an accepted cause of gastric ulceration in people, and there isan increased incidence of ulcerogenesis in stressed hypothyroid ratsmediated by gastric acid hypersecretion [68].
Septic patients, postoperative patients, and patients that have been
burned or experienced head trauma are predisposed to developing gastriculcers [69]. Increased vagal activity, increased gastric acid secretion, hista-mine release, decreased mucosal barrier function, decreased prostaglandinsynthesis, and decreased mucosal blood flow are all potential causativefactors [70]. The vagus nerve mediates excitatory input for increased acidsecretion by parietal cells and increased bowel motility. In addition to thevagal release of acetylcholine, a wide variety of neuromodulators are knownto be active in the gut (ie, serotonin, norepinephrine, gastrin, somatostatin,substance P, vasointestinal active peptide [VIP]), and both VIP and thyro-tropin-releasing hormone (TRH) have been shown to induce or aggravategastric ulcers. Although perhaps difficult to quantify, it is easy to appreciatethe fact that our veterinary patient population is also subjected to stress,whether it be from illness, surgery, hospitalization, or even more subtlefactors. The role of drugs in gastric ulceration has already been eluded to,and in 65% of the complications seen secondary to peptic ulcer disease inpeople (ie, hemorrhage, perforation), the episode can be linked to recentNSAID ingestion [71]. Altered gastric motility and disorganized myoelectriccomplex activity have been demonstrated secondary to indomethacin ad-ministration in dogs, resulting in gastric ulceration [72]. Although excessivecorticosteroids can damage the gastric mucosa, glucocorticoids have
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
a permissive role in the gastric mucosal protection induced by prostaglan-dins. This aspect of mucosal protection is lost in hypoadrenocorticism, andgastric ulceration is likely an attendant complication in many cases of canineAddison’s disease.
Although the presence of melena, hematemesis, positive fecal occult
blood, or an elevated blood urea nitrogen (BUN)/creatinine ratio suggeststhe presence of significant gastric ulceration, the definitive diagnosis relieson visualization (endoscopy) and histopathology. Once a presumptive ordefinitive diagnosis is made, treatment begins with the cessation of anypotentially ulcerogenic substances, followed by any number or combinationof medications described in the next section. The general goals of gastriculcer therapy are to eliminate any identified inciting agent or condition,protect already damaged mucosal tissue, decrease gastric acidity, and pro-mote rapid restitution of the normal mucosal barrier and defense functions.
Malignant gastric neoplasia in the dog includes carcinoma, leiomyosar-
coma, and lymphoma. Benign gastric tumors include adenomas andleiomyomas. The reader is referred to a recent excellent review for furtherinformation on neoplasia as a rule-out for gastritis in the dog [73].
The nematode Physaloptera is the classic parasitic rule-out for chronic
gastritis [74]. Intermediate hosts include beetles, crickets, and cockroaches. Adult worms usually occupy the fundus of the stomach or pyloric antrumand, unfortunately, are often diagnosed during the endoscopic search fora more ominous cause of vomition. Because Physaloptera eggs are difficultto find with examination of the feces, a single dose of pyrantel pamoate (4.5mg/lb) before endoscopy is a simple, inexpensive, and noninvasive strategyfor removing this parasite from the rule-out list. Pyrantel is also effectiveagainst roundworms, which may cause gastritis during their migratory trekthrough the stomach [75].
Lymphocytic/plasmacytic gastritis, eosinophilic gastritis, and granulo-
matous gastritis are best used as histologic descriptions of immune-mediatedgastric pathologic findings. Although the term idiopathic may be used ineach case to imply that the infiltrating inflammatory cells are the primarycausative agent, these cells are most often present in response to a distinctpathologic disturbance, such as neoplastic transformation, parasite in-festation, foreign antigens, or infectious agents. If no causative agent can beidentified and trial therapy has been attempted where appropriate (ie,treatment for parasites and allergies in eosinophilic gastritis), these cases aretreated as primary immune-mediated disturbances with nonspecific butoften effective immunosuppression.
Duodenal-gastric reflux (bilious vomiting syndrome) is a component
of a variety of human diseases often seen in children or after intestinalsurgery [76–78]. The syndrome is thought to result from abnormalities in the
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
motor function of the stomach and changes in the speed of gastric emptying[79]. In dogs, the diagnosis is one of exclusion to account for vomitingsecondary to bile-induced gastric inflammation. Bile salts acting asdetergents dissolve the mucosal lipids that help to form the gastric mucosalbarrier, allowing for back-diffusion of hydrogen ions and subsequentgastritis [80,81]. Dogs with the syndrome usually vomit in the morning afteran overnight fast and often respond to late night feedings, a prokinetic drug,an H2-receptor antagonist, or some combination thereof.
Amine precursor uptake and decarboxylation (APUD) tumors (ie,
gastrinoma), endocrinopathies, and organ failure can all result in gastrichyperacidity and inflammation.
In people, peptic ulcer formation following gastric hyperacidity secondary
to excessive gastrin production by a gastrinoma is known as Zollinger-Ellisonsyndrome. Gastrin not only stimulates excessive acid secretion but seems todecrease the tone of the pyloric sphincter, allowing for duodenal-gastric refluxof bile [82]. The first case report of the canine version of Zollinger-Ellisonsyndrome appeared in 1977 in a dog with esophagitis, gastritis, and a duodenalulcer [83]. Gastrinomas are rare in dogs and usually result in vomiting, weightloss, anorexia, and intermittent diarrhea. The biochemistry panel in these dogsmay be consistent with a pyloric outflow obstruction (ie, hypokalemia,hypochloremia, metabolic acidosis). Plasma gastrin levels can be measuredusing a radioimmunoassay kit, and the laboratory should be contacted forproper sample-handling ins tructions. A significant elevation in gastrin shouldprompt an effort toward tumor localization (eg, ultrasound, CT, MRI,radiolabeled-somatostatin analogues), although that effort may ultimatelydepend on intraoperative pancreatic palpation. A more complete discussionof the diagnosis and treatment of canine gastrinomas can be found in anexcellent recent review [84].
Liver disease can also result in hypergastrinemia, although not usually to
the degree seen with a gastrinoma. The loss of hepatic function also resultsin an increase in a variety of metabolic byproducts and toxins that maydirectly affect gastric function or stimulate symptoms of gastritis as a com-ponent of hepatic encephalopathy. People with chronic renal failure oftenbleed into their stomachs. Increased gastric mucosal permeability, a decreasein gastric mucosal blood flow, and mucosal ischemia lead to a more acidicintramucosal environment [85].
Gastric ulceration is a frequent complication in dogs with hypoadreno-
corticism, contributing to the symptoms of anorexia and vomiting. Systemichypovolemia with an attendant decrease in gastric mucosal blood flow,loss of the permissive effect of glucocorticoids on mucosal defense, andsignificant electrolyte abnormalities are all likely contributors to the gastritisseen with this endocrinopathy.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
Because of the established importance of H pylori in human beings, most
of the literature directed toward the treatment of gastritis in people ad-dresses the eradication of that causative agent [86]. Treatment of Helico-bacter spp in dogs usually entails a 2- to 3-week course of triple therapy:amoxicillin, metronidazole, and famotidine, with azithromycin, clarithro-mycin, omeprazole, or ranitidine as an alternative substitution. The treat-ment of bleeding gastric ulcers is also extensively researched but almostinvariably involves endoscopy and laser coagulation or similar therapy. Ironically, in one of the few studies looking specifically at the treatment ofcanine gastric ulceration secondary to neurosurgery and steroid adminis-tration, it was concluded that neither omeprazole nor misoprostol waseffective in healing or preventing the development of gastric mucosal lesions[87]. This is in contrast to the prevention of gastric ulceration in humanbeings using NSAIDs, where the use of either a prostaglandin analogueor proton pump inhibitor proved beneficial [88]. Thus, unfortunately,attempting to draw conclusions regarding the treatment of canine gastritisfrom the current literature is a precarious exercise at best. This is furthercomplicated by the inherent variability in what constitutes appropriatetreatment for the myriad of conditions falling under the heading of‘‘gastritis.’’ The correct therapy may range from emergency exploratorylaparotomy to simply the withholding of food on an outpatient basis. Assuming appropriate steps are taken to rule out gastrointestinal ob-struction, a brief period of gastric ‘‘rest’’ (withholding food but not waterfor 24–48 hours) is usually sufficient therapy for resolution in cases of simpleacute gastritis. If symptoms persist or worsen during the period of gastricrest or return shortly after the reintroduction of food, further treatmentshould be superseded by more extensive diagnostics (eg, complete bloodwork with appropriate ancillary tests, repeat radiographs, or more advancedimaging).
The most effective treatment for canine gastritis is quite obviously that
treatment directed toward a specific identified cause (eg, antiparasiticagents, surgical removal of a gastrinoma, discontinuation of an offendingdrug, removal of an inciting allergen). In lieu of or in addition to specifictreatments, there are a large number of agents that can be used ina nonspecific manner, all directed toward the relief of gastritis and itssymptoms. Table 1 is a brief summary of those treatments used mostcommonly in veterinary medicine. The appropriate choice of medicationis based on knowledge of the derangement most likely underlyingthe symptoms (eg, increased gastric acidity in uremic gastritis, gastrichypomotility in bilious vomiting syndrome) and an understanding of themechanism of action for each drug.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
[1] Guilford WG, Center SA, Strombeck DR, Williams DA, Meyer DJ, editors.
Strombeck’s small animal gastroenterology. 3rd edition. Philadelphia: WB Saunders;1996. p. 261–302.
[2] Neiger R, Simpson KW. Helicobacter infection in dogs and cats: fact and fiction. J Vet
[3] Simpson KW, Strauss-Avali D, McDonough PL, et al. Gastric function in dogs with
naturally acquired Helicobacter spp. infection. J Vet Intern Med 1999;13:507–15.
[4] Cattoli G, van Vugt R, Zanoni RG, et al. Occurrence and characterization of gastric
Helicobacter spp. in naturally infected dogs. Vet Microbiol 1999;70:239–50.
[5] Baba AL, Catoi C, Basea I, et al. Canine gastritis, associated with Helicobacter spp.
infection. Buletinul Universitatii de Stiinte Agricole Cluj Napoca Seria Zootehnie siMedicina Veterinara 1995;49:527–31.
[6] Haziroglu R, Diker KS, Guyenc T, et al. Canine gastritis associated with Helicobacter felis.
Deutsche Tieraztliche Wochenschrift 1995;102:474–6.
[7] Lee A, Krakowka S, Fox JG, et al. Role of Helicobacter felis in chronic canine gastritis.
[8] Patra PC, Tripathy SB. Gastritis in dogs and its therapy. Indian Vet J 1986;63:940–3. [9] Burrows CF. Diseases of the canine stomach. Vet Annu 1986;26:270–82.
[10] Clark WA. Canine gastric hyperplasia. Vet Annu 1985;25:245–7. [11] Happe RP, van den Brom WE, van der Gaag I, et al. Duodenogastric reflux in the dog,
a clinicopathological study. Res Vet Sci 1982;33:280–6.
[12] English RE, Breitschwerdt EB, Grindem CB, et al. Zollinger-Ellison syndrome and
myelofibrosis in a dog. JAVMA 1988;192:1430–4.
[13] Eaton KA, Paola JP, Johnson SE. Gastritis associated with gastric bacteria in
asymptomatic, random source dogs [abstract]. Vet Pathol 1992;29:454.
[14] Lee A, Krakowka S, Fox JG, et al. Role of Helicobacter felis in chronic canine gastritis. Vet
[15] Chung SC, Sung JY, Suen MW, et al. Endoscopic assessment of mucosal hemodynamic
changes in a canine model of gastric ulcer. Gastrointest Endosc 1991;37:310–3.
[16] Whitford GM, Gashley DH, Garman RH. Effects of fluoride on structure and function of
canine gastric mucosa. Dig Dis Sci 1997;42:2146–55.
[17] Nagamine K, Inokuchi K, Sakata H, et al. Development of erosive gastritis in a canine
model of esophageal varices. Jpn J Surg 1986;16:218–24.
[18] Duane WC, McHale AP, Sievert CE. Lysolecithin-lipid interactions in disruption of the
canine gastric mucosal barrier. Am J Physiol 1986;250:G275–79.
[19] Sullivan TR Jr, Dempsey DT, Milner R, et al. Effect of local acid-base status on gastric
mucosal blood flow and surface cell injury by bile acid. J Surg Res 1994;56:112–6.
[20] Gana TJ, MacPherson BR, Koo J. Gastric mucosal blood flow in misoprostol pretreated
aspirin-induced ulceration. Ann Surg 1988;207:327–34.
[21] Abdel-Salam OM, Czimmer J, Debreceni A, et al. Gastric mucosal integrity: gastric
mucosal blood flow and microcirculation. An overview. J Physiol (Paris) 2001;95:105–27.
[22] Kawano S, Tsuji S. Role of mucosal blood flow: a conceptional review in gastric mucosal
injury and protection. J Gastroenterol Hepatol 2000;15(Suppl):D1–6.
[23] Sorbye H, Svanes K. The role of blood flow in gastric mucosal defense, damage and
[24] Wallace JL, Granger DN. The cellular and molecular basis of gastric mucosal defence.
[25] Paimela H, Goddard PJ, Silen W. Present views on restitution of gastrointestinal epi-
thelium. Dig Dis Sci 1995;40:2495–6.
[26] Szabo S, Nagy L. Pathways, mediators and mechanisms of gastroduodenal mucosal injury.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
[27] Szabo S. Mechanisms of gastric mucosal injury and protection. J Clin Gastroenterol
[28] Wallace JL, Ma L. Inflammatory mediators in gastrointestinal defense and injury. Exp Biol
[29] Perry MA, Wadhwa S, Parks DA. Role of oxygen radicals in ischemia-induced lesions in
the cat stomach. Gastroenterology 1986;90:362–7.
[30] Jacobson ED. Circulatory mechanisms of gastric mucosal damage and protection.
Gastroenterology 1992;102:1788–800.
[31] Guilford WG, Jones BR, Markwell PJ, et al. Food sensitivity in cats with chronic
idiopathic gastrointestinal problems. J Vet Intern Med 2001;15:7–13.
[32] Bartuzi Z, Korenkiewicz J, Romanski B. Correlation between Helicobacter pylori infection
and food allergy in chronic gastritis. Med Sci Monit 2000;6:530–8.
[33] Kokkonen J, Ruuska T, Karttunen TJ, et al. Mucosal pathology of the foregut
associated with food allergy and recurrent abdominal pains in children. Acta Paediatr2001;90:16–21.
[34] Bartuzi Z, Gawronska-Ukleja E, Romanski B. Macroscopic picture of gastric mucosa in
endoscopic examination of patients with chronic gastritis and food allergy. Med Sci Monit2000;6:1203–8.
[35] Proujansky R, Winter HS, Walker WA. Gastrointestinal syndromes associated with food
sensitivity. Adv Pediatr 1988;35:219–37.
[36] Bischoff SC, Mayer JH, Manns MP. Allergy and the gut. Int Arch Allergy Immunol
[37] Blakemore JC. Gastrointestinal allergy. Vet Clin North Am Small Anim Pract 1994;24:655–95. [38] LeVeen HH, LeVeen EG, LeVeen RF. Awakenings to the pathogenicity of urease and the
requirement for continuous long term therapy. Biomed Pharmacother 1994;48:157–66.
[39] Hawkey CJ. NSAID toxicity: where are we and how do we go forward? J Rheumatol
[40] Jones RD, Baynes RE, Nimitz CT. Nonsteroidal anti-inflammatory drug toxicosis in dogs
and cats: 240 cases (1989–1990). JAVMA 1992;201:475–7.
[41] Nicoloff DM. Indomethacin. Effect on gastric secretion, parietal cell populations, and ulcer
provocation in the dog. Arch Surg 1968;97:809–15.
[42] Shorrock CJ, Rees WD. Mechanisms of gastric damage by non-steroidal anti-
inflammatory drugs. Scand J Rheumatol Suppl 1989;78:5–11.
[43] Konturek JW, Dembinski A, Stoll R, et al. Gastric mucosal blood flow and neutrophil
activation in aspirin-induced gastric mucosal damage in man. Scand J Gastroenterol1993;28:767–71.
[44] Dow SW, Rosychuck AW, McChesney AE, et al. Effects of flunixin and flunixin plus
prednisone on the gastrointestinal tract of dogs. Am J Vet Res 1990;51:1131–8.
[45] Green GA. Understanding NSAIDs: from aspirin to COX-2. Clin Cornerstone 2001;3:50–60. [46] Wallace JL, Ma L. Inflammatory mediators in gastrointestinal defense and injury. Exp Biol
[47] Nishihara K, Kikuchi H, Kanno T, et al. Comparison of the upper gastrointestinal effects
of etodolac and aspirin in healthy dogs. J Vet Med Sci 2001;63:1131–3.
[48] Reimer ME, Johnston SA, Leib MS, et al. The gastroduodenal effects of buffered aspirin,
carprofen, and etodolac in healthy dogs. J Vet Intern Med 1999;13:472–7.
[49] Forsyth SF, Guilford WG, Haslett SJ, et al. Endoscopy of the gastroduodenal mucosa
after carprofen, meloxicam and ketoprofen administration in dogs. J Small Anim Pract1998;39:421–4.
[50] Kay-Mugford P, Benn SJ, LaMarre J, et al. In vitro effects of nonsteroidal anti-
inflammatory drugs on cyclooxygenase activity in dogs. Am J Vet Res 2000;61:802–10.
[51] Ricketts AP, Lundy KM, Seibel SB. Evaluation of selective inhibition of canine cyclo-
oxygenase 1 and 2 by carprofen and other nonsteroidal anti-inflammatory drugs. Am J VetRes 1998;59:1441–6.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
[52] Peskar BM, Maricic N, Gretzera B, et al. Role of cyclooxygenase-2 in gastric mucosal
defense. Life Sci 2001;69:2993–3003.
[53] Bjorkman DJ. One hundred years of NSAID gastropathy: are coxibs the answer? Rev
Gastroenterol Disord 2001;1:121–7.
[54] Dow SW, Rosychuk RAW, McChesney AE, et al. Effects of flunixin and flunixin plus
prednisone on the gastrointestinal tract of dogs. Am J Vet Res 1990;51:1131–8.
[55] Sorjonen DC, Dillon AR, Powers RD, et al. Effects of dexamethasone and surgical
hypotension on the stomach of dogs: clinical, endoscopic, and pathologic evaluations. AmJ Vet Res 1983;44:1233–7.
[56] McDonough PL, Simpson KW. Diagnosing emerging bacterial infections: salmonellosis,
campylobacteriosis, clostridial toxicosis, and helicobacteriosis. Semin Vet Med Surg1996;11:187–97.
[57] Covacci A, Telford JL, Del Giudice G, et al. Helicobacter pylori virulence and genetic
geography. Science 1999;284:1328–33.
[58] Cave DR. Chronic gastritis and Helicobacter pylori. Semin Gastrointest Dis 2001;12:196–
[59] Jalava K, Kaartinen M, Utriainen M, et al. Helicobacter salomonis sp. nov., a canine
gastric Helicobacter sp. related to Helicobacter felis and Helicobacter bizzozeronii. Int J SystBacteriol 1997;47:975–82.
[60] Strauss-Ayali D, Simpson KW, Schein AH, et al. Serological discrimination of dogs
infected with gastric Helicobacter spp. and uninfected dogs. J Clin Micro 1999;37:1280–7.
[61] Eaton KA, Dewhirst FE, Paster BJ, et al. Prevalence and varieties of Helicobacter species
in dogs from random sources and pet dogs: animal and public health implications. J ClinMicrobiol 1996;34:3165–70.
[62] Hermanns W, Kregel K, Breuer W, et al. Helicobacter-like organisms: histopathological
examination of gastric biopsies from dogs and cats. J Comp Path 1995;112:307–18.
[63] Yamasaki K, Suematsu H, Takahashi T. Comparison of gastric lesions in dogs and cats
with and without gastric spiral organisms. JAVMA 1998;212:529–33.
[64] Simpson KW, Strauss-Ayali D, McDonough PL, et al. Gastric function in dogs with
naturally acquired gastric Helicobacter spp. infection. J Vet Intern Med 1999;13:507–15.
[65] Walsh JH, Peterson WL. The treatment of Helicobacter pylori infection in the management
of peptic ulcer disease. N Engl J Med 1995;333:984–91.
[66] Simpson K, Neiger R, DeNovo R, et al. The relationship of Helicobacter spp. infection to
gastric disease in dogs and cats. J Vet Intern Med 2000;14:223–7.
[67] Pollock RVH, Coyne MJ. Canine parvovirus. Vet Clin North Am Small Anim Pract 1993;
[68] Hernandez DE, Walker CH, Mason GA. Influence of thyroid states on stress gastric ulcer
formation. Life Sci 1988;42:1757–64.
[69] Cho CH, Koo MWL, Garg GP, et al. Stress-induced gastric ulceration: its aetiology and
clinical implications. Scand J Gastroenterol 1992;27:257–62.
[70] Konturek PK, Brzozowski TZ, Konturek SJ, et al. Role of epidermal growth factor,
prostaglandin, and sulfhydryls in stress-induced gastric lesions. Gastroenterology1990;99:1607–15.
[71] Wallace JL. Gastric ulceration: critical events at the neutrophil-endothelium interface. Can
J Physiol Pharmacol 1993;71:98–102.
[72] Fioramonti J, Bueno L. Gastrointestinal myoelectric activity disturbances in gastric ulcer
disease in rats and dogs. Dig Dis Sci 1980;25:575–80.
[73] Gualtieri M, Monzeglio MG, Scanziani E. Gastric neoplasia. Vet Clin North Am Small
[74] Burrows CF. Infection with the stomach worm Physaloptera as a cause of chronic vomiting
in the dog. J Am Anim Hosp Assoc 1983;19:947–50.
[75] Hall JA. Diseases of the stomach. In: Ettinger SJ, Feldman EC, editors. Textbook of
veterinary internal medicine. 5th edition. Philadelphia: WB Saunders; 2000. p. 1154–82.
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
[76] Philip PA. Superior mesenteric artery syndrome: an unusual cause of intestinal obstruction
in brain-injured children. Brain Inj 1992;6:351–8.
[77] Fang SB, Lee HC, Huang FY, et al. Intestinal pseudo-obstruction followed by major
clinical features of Kawasaki disease: report of one case. Acta Paediatr Taiwan 2001;42:111–4.
[78] Bondurant FJ, Maull KI, Nelson HS, et al. Bile reflux gastritis. South Med J 1987;80:
[79] Eagon JC, Miedema BW, Kelly KA. Postgastrectomy syndromes. Surg Clin North Am
[80] Duane WC, Wiegand DM. Mechanism by which bile salt disrupts the gastric mucosal
barrier in the dog. J Clin Invest 1980;66:1044–9.
[81] Ritchie WP Jr. Alkaline reflux gastritis. Late results on a controlled trial of diagnosis and
treatment. Ann Surg 1986;203:537–44.
[82] McGuigan JE. The endocrine ulcer concept. Dig Dis 1976;21:144–7. [83] Straus E, Johnson GF, Yalow RS. Canine Zollinger-Ellison syndrome. Gastroenterology
[84] Simpson KW. Gastrinoma in dogs. In: Bonagura JD, editor. Current veterinary therapy
XIII. Philadelphia: WB Saunders; 2000. p. 617–21.
[85] Diebel L, Kozol R, Wilson RF, et al. Gastric intramucosal acidosis in patients with chronic
kidney failure. Surgery 1993;113:520–6.
[86] Ruggiero P, Peppoloni S, Berti D, et al. New strategies for the prevention and treatment of
Helicobacter pylori infection. Expert Opin Invest Drugs 2002;11:1127–38.
[87] Neiger R, Gaschen F, Jaggy A. Gastric mucosal lesions in dogs with acute intervertebral
disc disease: characterization and effects of omeprazole or misoprostol. J Vet Intern Med2000;14:33–6.
[88] Graham DY, Agrawal NM, Roth SH. Prevention of NSAID-induced gastric ulcer with
misoprostol: multicentre, double-blind, placebo-controlled trial. Lancet 1988;2:1277–80.
EDITORIAL science and trust in the public arena picked up a bottle of echinacea, an herbal remedy purported tocure upper respiratory infections. For several days I religiously swallowed the recommendeddosage. By the fifth day, I felt worse. As I struggled to concentrateon work, I took a break by Googling echinacea to look for reportsof its effectiveness. I discovered echinacea has bee
Qu’est-ce que la grippe ? La grippe est une infection respiratoire aiguë fréquente, contagieuse et d’origine virale due aux virus Influenzae . Elle est à l’origine d’épidémies annuelles. Les virus grippaux se répartissent entre différents types : A, B et C. Les virus A et B sont à l’origine des épidémies saisonnières, mais seul le virus A peut être responsable de p
 Craig Webb, DVM, PhD*, David C. Twedt, DVM
College of Veterinary Medicine and Biomedical Sciences, Colorado State University,
Gastritis—inflammation of the stomach—is a frequently cited differential
yet rarely characterized diagnosis in cases of canine anorexia and vomit-ing. Although the list of rule-outs for acute or chronic gastritis is extensive(Box 1) [1], a review of the veterinary literature reveals fewer than 15 articlesthat have focused on clinical cases of canine gastritis over the last 25 years[2–14]. The dog frequently appears in the human literature as an ex-perimentally manipulated model for the study of endoscopic techniques orthe effect of medications on gastric mucosa [15–20]. In the veterinarypatient, cases of acute gastritis are rarely pursued with the complete di-agnostic armamentarium, and cases of chronic gastritis are rarely found tooccur as an entity isolated from the rest of the gastrointestinal tract. Thisarticle focuses on those findings most clinically relevant to cases of caninegastritis in veterinary medicine.
Craig Webb, DVM, PhD*, David C. Twedt, DVM
College of Veterinary Medicine and Biomedical Sciences, Colorado State University,
Gastritis—inflammation of the stomach—is a frequently cited differential
yet rarely characterized diagnosis in cases of canine anorexia and vomit-ing. Although the list of rule-outs for acute or chronic gastritis is extensive(Box 1) [1], a review of the veterinary literature reveals fewer than 15 articlesthat have focused on clinical cases of canine gastritis over the last 25 years[2–14]. The dog frequently appears in the human literature as an ex-perimentally manipulated model for the study of endoscopic techniques orthe effect of medications on gastric mucosa [15–20]. In the veterinarypatient, cases of acute gastritis are rarely pursued with the complete di-agnostic armamentarium, and cases of chronic gastritis are rarely found tooccur as an entity isolated from the rest of the gastrointestinal tract. Thisarticle focuses on those findings most clinically relevant to cases of caninegastritis in veterinary medicine.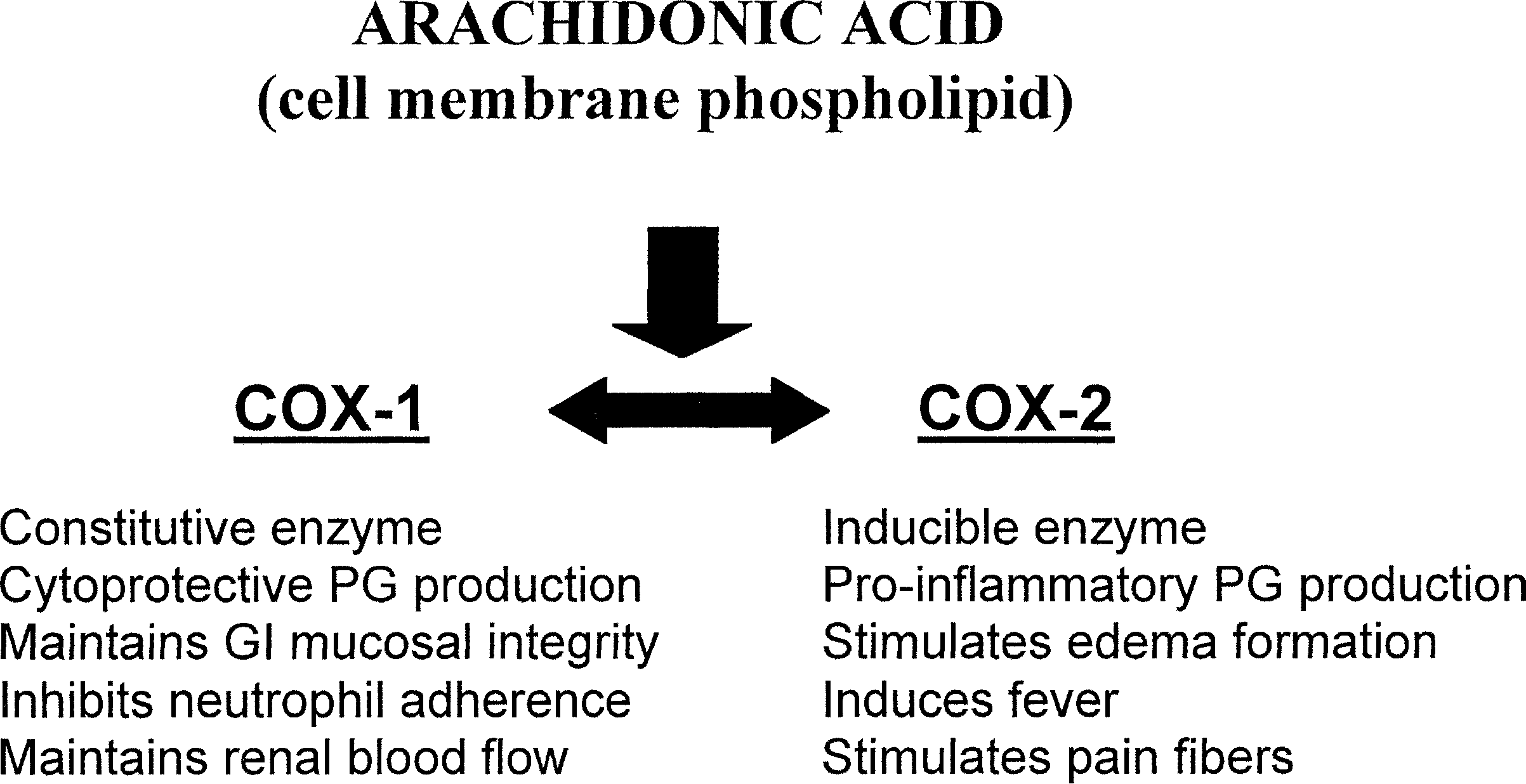 C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
Because of the prevalence of NSAID-induced gastric ulceration, the
development of increasingly specific COX-2 inhibitors has burgeoned intoa multibillion dollar pharmaceutic industry, and COX-2 selective inhibitorsare now some of the most frequently prescribed drugs in human medicine[45]. The theory behind the use of COX-2 inhibitors is illustrated in Fig. 1[46]. Although not entirely COX-2 selective, Rimadyl and Etogesic are twoNSAIDs approved for use in dogs and designed to reduce ulcer formationrelative to aspirin. Endoscopic examination used to compare the gastricmucosa of dogs given aspirin with that of dogs treated with etodolac foundthat dogs given aspirin invariably had mucosal erosions by day 17 oftreatment, whereas none of the dogs given etodolac were found to have anygastric lesions [47]. Regardless of the NSAID administered, none of the dogsin this study were found to have any biochemical abnormalities, vomiting,anorexia, or melena. Other similar studies have confirmed the ubiquity ofgastric lesions in dogs receiving aspirin as well as illustrating only the mostminor changes in dogs receiving either etodolac or carprofen [48,49].
C. Webb, D.C. Twedt / Vet Clin Small Anim 33 (2003) 969–985
Because of the prevalence of NSAID-induced gastric ulceration, the
development of increasingly specific COX-2 inhibitors has burgeoned intoa multibillion dollar pharmaceutic industry, and COX-2 selective inhibitorsare now some of the most frequently prescribed drugs in human medicine[45]. The theory behind the use of COX-2 inhibitors is illustrated in Fig. 1[46]. Although not entirely COX-2 selective, Rimadyl and Etogesic are twoNSAIDs approved for use in dogs and designed to reduce ulcer formationrelative to aspirin. Endoscopic examination used to compare the gastricmucosa of dogs given aspirin with that of dogs treated with etodolac foundthat dogs given aspirin invariably had mucosal erosions by day 17 oftreatment, whereas none of the dogs given etodolac were found to have anygastric lesions [47]. Regardless of the NSAID administered, none of the dogsin this study were found to have any biochemical abnormalities, vomiting,anorexia, or melena. Other similar studies have confirmed the ubiquity ofgastric lesions in dogs receiving aspirin as well as illustrating only the mostminor changes in dogs receiving either etodolac or carprofen [48,49].