Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Exbm-231-06-34 967.973
Bosentan, Sildenafil, and Their Combination
MARTINE CLOZEL,*,1 PATRICK HESS,* MARKUS REY,* MARC IGLARZ,*
CHRISTOPH BINKERT,* AND CHANGBIN QIU*,
*Actelion Pharmaceuticals Ltd, CH-4123 Allschwil, Switzerland; and Department of Pharmacology,
Shanghai Institute of Materia Medica, Chinese Academy of Sciences, Shanghai, China
The dual endothelin receptor antagonist, bosentan, and the
nary vascular resistance leading to right ventricular (RV)
phosphodiesterase inhibitor, sildenafil, are efficacious in ex-
failure (1). Two orally available agents have been shown to
perimental and clinical pulmonary hypertension (PHT). The
be clinically effective. Bosentan, a dual endothelin (ET)
effects of bosentan, sildenafil, and their combination wereevaluated in rats with monocrotaline (MCT)-induced PHT. A first
ETA/ETB receptor antagonist, improves hemodynamics,
group consisted of control rats with no MCT injection. Four
increases exercise capacity, and decreases the rate of clinical
other groups of rats received MCT subcutaneously and were
worsening in patients with World Health Organization Class
assigned to receive no treatment, 300 mg/kg/day bosentan as
III or IV PAH (2, 3). This is in agreement with a key
food admix, 100 mg/kg/day sildenafil in drinking water, or theircombination for 4 weeks. The doses of bosentan and sildenafil
pathogenic role of ET in PAH. Sildenafil, which enhances
were the maximally effective doses based on a dose-range–
nitric oxide (NO) signaling by inhibition of phosphodiester-
finding study. Mortality was 0%, 53%, 11%, 11%, and 0%,
ase Type 5 (PDE5), was shown to improve hemodynamics
respectively, in the five different groups. Bosentan and sildenafil
and exercise capacity in patients with PAH, without
significantly attenuated the increase in mean pulmonary arterialpressure, and the combination had an additional effect.
significantly affecting the rate of clinical worsening (4).
Similarly, bosentan, sildenafil, and, to a greater extent, their
Because bosentan and sildenafil act on different targets,
combination significantly reduced right ventricular (RV) hyper-
combining these two therapies might provide an added
trophy. Bosentan, but not sildenafil, decreased norepinephrine
benefit. However, the ET and NO systems interact (5);
and BNP plasma concentrations, reduced kidney weight, andnormalized systemic hemodynamics. In conclusion, bosentan
therefore, the combination of drugs affecting the two
and sildenafil are efficacious in rats with chronic PHT, and their
pathways might not be additive. We investigated the effects
combination shows an additional effect for decreasing pulmo-
of the combination using the rat model of monocrotaline
nary arterial pressure, reducing plasma catecholamines, main-
(MCT)-induced pulmonary hypertension (PHT).
taining body weight, and reducing mortality. Exp Biol Med231:967–973, 2006
MCT, a pyrrolizidine alkaloid of plant origin (6),
Key words: bosentan; endothelin; nitric oxide; pulmonary
induces progressive PHT in rats after a single subcutaneous
injection (7, 8). Rats exposed to MCT develop acutepulmonary vascular inflammation. Although this model maynot fully reflect the clinical situation of PAH (9), the ET
system is associated with the pathogenesis of the disease in
Pulmonary arterial hypertension (PAH) is an often-fatal
this rat PHT model as well as in human PAH (10–12). Both
disease characterized by a progressive increase in pulmo-
bosentan (13, 14) and sildenafil (15) have been shown toattenuate the development of PHT in rats treated with MCT. The objectives of this study were to compare thepharmacologic profiles of bosentan and sildenafil, and to
1 To whom correspondence should be addressed at Actelion Pharmaceuticals Ltd.,Gewerbestrasse 16, CH-4123 Allschwil, Switzerland. Email: martine.clozel@
evaluate the effects of their combination at maximally
effective doses on pulmonary arterial pressure, cardiac size,and endothelial function in MCT-induced PHT rats. The
Received September 29, 2005. Accepted November 17, 2005.
effects of the two drugs and their combination on plasmaconcentrations of ET-1, brain natriuretic peptide (BNP;
Refs. 16, 17), cGMP (15, 18), and catecholamines (19) were
Copyright Ó 2006 by the Society for Experimental Biology and Medicine
thermostatically controlled heating table to maintain body
Animals. Male Wistar rats were purchased from RCC
temperature at 368C–388C. A tracheotomy tube was put in
Ltd. (Fu¨llingsdorf, Switzerland) or from the Experimental
place and a catheter inserted into the right jugular vein for
Animal Center of the Chinese Academy of Sciences
measurement of MPAP, using the procedure previously
(Shanghai, China), and maintained under identical con-
described by Stinger et al. (20). Measurements were
ditions in accordance with local guidelines (Basel-Land-
recorded for 15 mins using a PowerLab data acquisitionsystem (IOX 1.7.0 Data acquisition; Emka Technologies,
schaft cantonal veterinary office or Animal Care and Use
Paris, France) connected to a Dell Optiplex GX 270
Committee of the Shanghai Institute of Materia Medica,
computer equipped with Datanalyst software (v.1.83.0;
Chinese Academy of Sciences). All rats were housed in
climate-controlled conditions with a 12:12-hr light:dark
Arterial Blood Pressure Measurements in Con-
cycle, and had free access to chow and water.
scious, Freely Moving Rats. For measurement of
MCT Treatment. MCT (Sigma Chemicals, St. Louis,
arterial blood pressure and heart rate, a subset of 25 rats
MO) was administered as a single subcutaneous (sc)
was surgically implanted with a pressure sensor/transmitter
injection (60 mg/kg) in a volume of 3 ml/kg, and control,
(model TA11PA-C40; Data Sciences, St. Paul, MN) in the
age-matched rats received an equal volume of saline. These
peritoneal cavity. The sensing catheter was placed in the
animals were randomly assigned into experimental groups,
descending aorta below the renal arteries, pointing up-
and treatment was initiated immediately after MCT
stream. A receiver platform (RPC-1, Data Sciences)
injection, for a duration of 4 weeks.
connected the radio signal to digitized input that was then
Test Compounds. Test compounds were supplied
sent to a dedicated personal computer (Compaq, Deskpro,
by Actelion Pharmaceuticals Ltd. (Shanghai, China and
Hewlett-Packard, Geneva, Switzerland). Arterial pressures
Allschwil, Switzerland). Bosentan was given as food admix,
were calibrated using input from an ambient-pressure
and sildenafil was given in drinking water.
reference (APR-1; Data Sciences). Two weeks after
Experimental Protocols. Dose-Finding Studies
implantation of the telemetry device, the rats were
for Bosentan and Sildenafil. In the first study, dose-
randomized into the five treatment groups (n ¼ 5 per
range–finding studies were conducted to determine the
group). Arterial blood pressure and heart rate measurements
maximally effective doses of bosentan and sildenafil on
were collected at 5-min intervals for 4 weeks.
mean pulmonary arterial pressure (MPAP) in MCT-treated
ET-1, BNP, cGMP, and Catecholamine Concen-
rats. Bosentan (0, 10, 30, 100, or 300 mg/kg/day as food
trations. At the end of the hemodynamic experiments in
admix; n ¼ 14 or 15 per dose) or sildenafil (0, 3, 10, 30, or
anesthetized rats, plasma samples in 5% EDTA were
100 mg/kg/day in drinking water; n ¼ 4 or 5 per dose) was
collected for determinations of ET-1, BNP, cGMP, and
given for 4 weeks, and MPAP determined in anesthetized
catecholamine concentrations. Plasma ET-1 concentration
rats, as described below in ‘‘Hemodynamic Study in
was measured using a human ET-1 immunoassay kit
Anesthetized Rats.’’ Doses of 300 mg/kg/day bosentan
(QuantiGlo, QET00; R&D Systems, Minneapolis, MN);
and of 100 mg/kg/day sildenafil were chosen for the next
BNP was measured using a rat BNP-32 enzyme immuno-
study, because they were maximally effective doses, that is,
assay (S-1192.001; Bachem, Heidelberg, Germany); cGMP
at the plateau of the respective dose-response curves, and
was measured using an enzyme immunoassay (DE0600;
R&D Systems); and epinephrine and norepinephrine were
Comparison and Combination of Bosentan and
measured using a CATCOMBI enzyme-linked immuno-
Sildenafil. After determination of maximally effective
sorbent assay kit (RE58242; IBL, Hamburg, Germany).
doses of bosentan and sildenafil, a second study was
Organ Weights. At the end of the study, rats were
performed. Male Wistar rats (210–240 g) were randomized
sacrificed. Heart, lungs, kidneys, and liver were removed
into five groups: Group 1 (control), sc injection of saline and
and weighed, and the ratio of organ weight to body weight
no treatment (n ¼ 15); Group 2, sc injection of MCT and no
(BW) was calculated. The RV and the left ventricle plus
treatment (n ¼ 19); Group 3, MCT plus 300 mg/kg/day
septum were separated and weighed; the ratio RV/BW was
bosentan as food admix (n ¼ 19); Group 4, MCT plus 100
mg/kg/day sildenafil in drinking water (n ¼ 19); and Group
Endothelial Function. Ring segments of aorta (one
5, MCT plus 300 mg/kg/day bosentan plus 100 mg/kg/day
per rat; n ¼ 8–10 per group), cleaned of fat and connective
tissues and 3 mm in length, were mounted between two
Hemodynamic Study in Anesthetized Rats. To
stainless-steel wires in 10-ml organ baths (Emka Technol-
evaluate the effects of bosentan and sildenafil on the
ogies). After a 30-min recovery period, stepwise increases in
development of PHT in both studies, hemodynamic
tension up to 2 g were applied to each segment. Two
measurements were performed in anesthetized rats. Four
consecutive administrations of 60 mM KCl were performed.
weeks after MCT injection, the rats were anesthetized by
Preconstriction of the aortic ring was achieved with a
intraperitoneal injection of 100 mg/kg thiobutabarbital-Na
concentration of phenylephrine (Sigma) sufficient to reach
(Inactin; Byk-Gulden, Konstanz, Germany) and placed on a
approximately 70% of the tissue maximum, as determined
BOSENTAN AND SILDENAFIL IN PULMONARY HYPERTENSIVE RATS
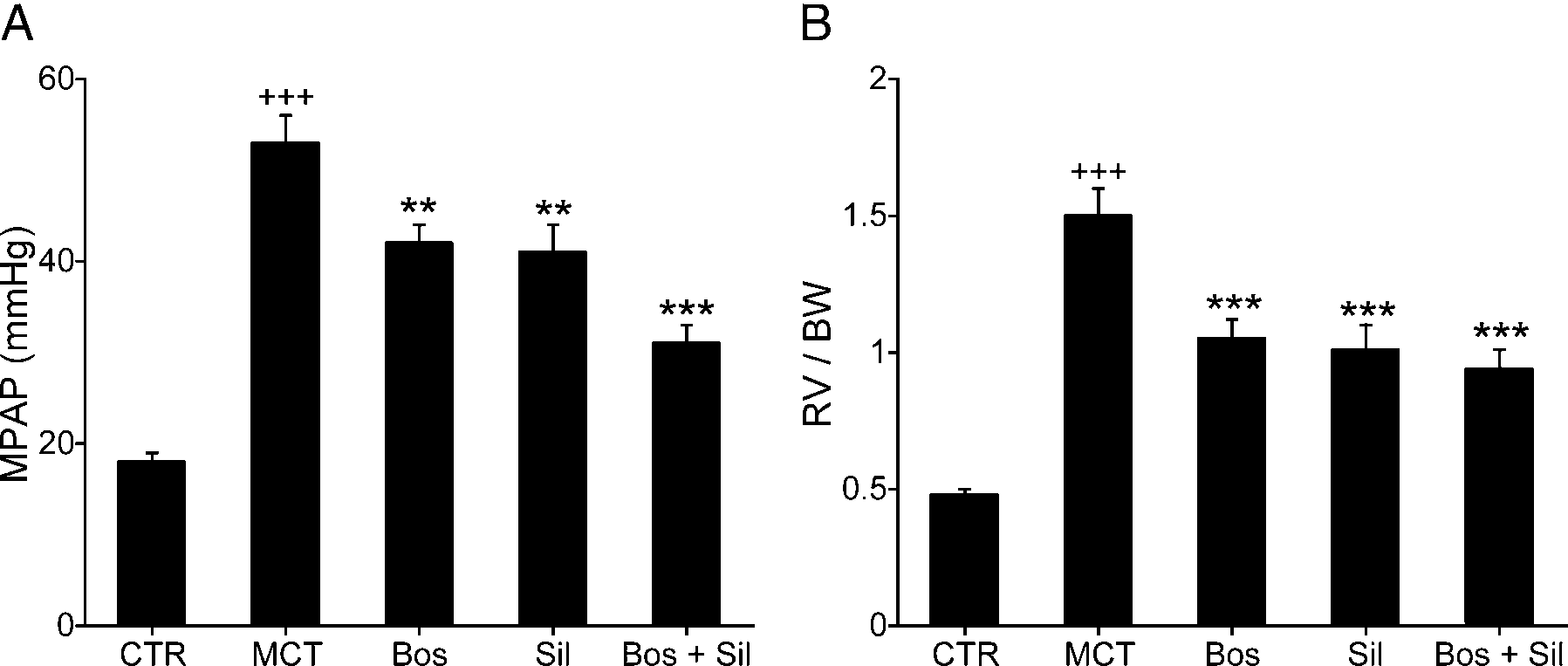
Figure 1. Effect of chronic oral administration of bosentan, sildenafil, and their combination on (A) MPAP in anesthetized rats; and (B) on RVhypertrophy, measured as the ratio of RV weight to BW, 4 weeks after MCT injection. CTR, control; MCT, MCT alone; Bos, bosentan; Sil,sildenafil. þþþP , 0.001 versus control; **P , 0.01 versus MCT alone; ***P , 0.001 versus MCT alone.
with KCl. Then, each segment was tested as follows: (i)
bosentan and 100 mg/kg/day sildenafil had similar effects
determination of concentration-response curve for 1 nM to
and decreased MPAP by 21% (42 6 2 mm Hg and 41 6 3
10 lM acetylcholine (Sigma); and (ii) determination of
mm Hg; P , 0.01, respectively). Combination treatment
concentration-response curve for 10 pM to 1 lM sodium
caused a further decrease and reduced MPAP by 42% (31 6
2 mm Hg; P , 0.001, as compared with untreated rats).
Statistical Analysis. All data are presented as mean
Arterial Blood Pressure Measurements in Con-
6 SEM. Statistical analyses were performed by analysis of
scious Rats. At baseline, neither mean arterial pressure
variance (ANOVA) using Statistica (StatSoft, Berikon,
nor heart rate differed among the various groups. Four
Switzerland) and Student-Newman-Keuls procedure for
weeks after MCT injection, there were no differences in
multiple comparisons. The null hypothesis was rejected
heart rate between the various groups. Untreated rats
when P , 0.05. To avoid a bias due to the death rate
showed a significant blood pressure decrease from baseline
observed in certain groups, all data missing because of early
(D, À9.7 6 2.3 mm Hg), as compared with control rats (D,
mortality were imputed using the worst value from each
À1.5 6 2.8 mm Hg; P , 0.05). Bosentan, but neither
sildenafil nor the combination, significantly prevented thisdecrease (D, À1.6 6 1.6 mm Hg; P , 0.05).
Endothelial Function. MCT-treated rats exhibited a
First Study: Dose Finding. PHT had developed in
marked endothelial dysfunction, characterized by a de-
untreated rats 4 weeks after MCT injection, and chronic oral
creased response to acetylcholine (maximal effect ¼ 71.7 6
administration of bosentan and of sildenafil dose-depend-
6.1% in MCT rats vs. 97.2 6 1.6% in controls; P , 0.001;
ently reduced the increase in MPAP. The maximally
and logEC50 ¼À6.94 6 0.11 in MCT rats vs. À7.44 6 0.03
effective dose of sildenafil, 100 mg/kg/day, reduced MPAP
in controls; P , 0.001; Fig. 2A) without any alteration of
to the same extent as 300 mg/kg/day bosentan (MPAP, 23.0
the response to sodium nitroprusside (Fig. 2B). Bosentan,
6 3.5 mm Hg and 19.8 6 1.4 mm Hg, respectively). These
sildenafil, or the combination increased endothelium-
doses were, therefore, chosen for the subsequent study.
dependent relaxation to acetylcholine (Fig. 2A) without
modifying the response to sodium nitroprusside (Fig. 2B).
of Bosentan and Sildenafil. Mortality. Because of the
ET-1, BNP, cGMP, and Catecholamine Concen-
severity of the animal model, mortality was significantly
trations. Four weeks after MCT injection, the mean plasma
higher in the untreated MCT rats compared with the control
ET-1 concentration was significantly increased as compared
rats. During the 4-week treatment period and during
with control rats (Table 1). Bosentan increased the mean
anesthesia at the end of the treatment period, mortality
plasma ET-1 concentration by 5-fold as compared with
was 0%, 53%, 11%, 11%, and 0%, respectively, in the five
untreated MCT rats. In contrast, sildenafil decreased the
mean plasma ET-1 concentration by 50% compared with
Hemodynamics. Four weeks after MCT injection,
untreated MCT rats. The combination of bosentan and
untreated rats exhibited higher MPAP as compared with
sildenafil increased plasma ET-1 concentration, but to a
controls (53 6 3 mm Hg vs. 18 6 1 mm Hg; P , 0.001;
lesser extent (93% increase) than with bosentan alone. The
Fig. 1). As expected, administration of 300 mg/kg/day
plasma BNP concentration increased by 21% and the
Figure 2. Effect of chronic oral administration of bosentan, sildenafil, and their combination on endothelium-dependent and independentrelaxation, measured in aortic ring segments isolated from rats 4 weeks after MCT injection. (A) The concentration-response curves in responseto acetylcholine (endothelium-dependent relaxation). (B) The concentration-response curves in response to sodium nitroprusside (endothelium-independent relaxation). CTR, control; MCT, MCT alone; Bos, bosentan; Sil, sildenafil. þþþP , 0.001 versus control; **P , 0.01 versus MCTalone; ***P , 0.001 versus MCT alone.
plasma cGMP concentration increased by 73% in MCT rats
injection, the mean BW of untreated animals was 25% less
compared with control rats (Table 1); these increases were
than that of control rats (267 6 11 g vs. 357 6 9 g; P ,
significantly inhibited by bosentan. No significant changes
0.001). Bosentan or sildenafil significantly attenuated the
in plasma BNP or cGMP concentrations were observed in
decrease in BW (297 6 12 g and 304 6 7 g, respectively)
rats treated with sildenafil or with sildenafil plus bosentan as
and the combination had an additional effect (327 6 7 g; P
compared with untreated MCT rats. Catecholamines
, 0.001). Right ventricular weight expressed per BW
increased in PHT rats, as shown by a 147% increase in
increased significantly in MCT rats compared with control
plasma epinephrine and a 41% increase in plasma
rats (1.50 6 0.1 g vs. 0.48 6 0.02 g; P , 0.001). Bosentan,
norepinephrine compared with control rats (Table 1).
sildenafil, or their combination for 4 weeks significantly
Bosentan markedly reduced plasma norepinephrine concen-
reduced RV/BW by 30%, 33%, and 37%, respectively (P ,
trations to values even lower than in control rats, and a
0.001 for all vs. no treatment). Similar results were obtained
further decrease was observed in MCT rats treated with
using the ratio RV/(LV þ septum). The ratio of lung weight
bosentan plus sildenafil. There was no effect of sildenafil
(LW) to BW significantly increased in MCT rats (7.5 6 0.6
alone on plasma norepinephrine concentration. The increase
vs. 4.2 6 0.1; P , 0.001). Bosentan or sildenafil had no
in plasma epinephrine was significantly attenuated by
statistically significant effect, but the combination signifi-
bosentan or the combination, but, again, sildenafil alone
cantly decreased the LW (LW/BW ¼ 6.0 6 0.3; P , 0.05 as
compared with untreated MCT rats). Liver weight normal-
Body and Organ Weights. Baseline BW was similar
ized for BW was similar to that of control rats in both
in each experimental group. At 4 weeks after MCT
untreated MCT rats and bosentan-treated rats. In rats treated
Effect of Bosentan, Sildenafil, and Their Combination on Plasma ET-1, BNP, cGMP, and
a Data are mean 6 SEM. All missing data were imputed using the worst value from each group.
þþP , 0.01; þþþP , 0.001 versus control.
*P , 0.05; **P , 0.01; ***P , 0.001 versus MCT alone.
BOSENTAN AND SILDENAFIL IN PULMONARY HYPERTENSIVE RATS
with sildenafil or the combination, liver weight increased
ETA/ETB antagonists (25, 26); this is not the case with
(39.0 6 1.1 and 41.6 6 0.6; P , 0.001). The kidney weight
selective ETA receptor antagonists (27). In contrast,
(KW) to BW ratio increased in MCT-treated rats (6.84 6
sildenafil, similar to PDE5 inhibitors in general, has been
0.21 vs. 6.11 6 0.15; P , 0.01). The increase in KW was
shown to stimulate sympathetic activity and increase
prevented in part by bosentan (KW/BW ¼ 6.35 6 0.16; P ¼
norepinephrine concentrations (28). Both epinephrine and
0.07), but sildenafil or the combination had no effect on KW
norepinephrine were further reduced when bosentan and
sildenafil were combined, suggesting a further neuro-hormonal inhibition, which could possibly contribute to
the survival benefit brought by the bosentan plus sildenafil
The goal of this study was 2-fold: to compare the
combination. Bosentan, but not sildenafil, prevented the
effects of sildenafil and bosentan, and to evaluate whether
decrease in mean arterial blood pressure observed in MCT-
the combination of bosentan and sildenafil confers an
treated rats, and the effect was partially negated by co-
additional benefit for treatment of PHT. Our results show
administration of sildenafil. The reductions of KW and
that combination therapy may be more effective, particularly
plasma BNP concentrations caused by bosentan were also
for decreasing MPAP, than either agent given alone at the
hindered by sildenafil co-administration. Liver weight was
maximally effective dose. Our results also show that
increased only in sildenafil-treated rats; this is a known
bosentan and sildenafil differ in their profiles, and that
species-specific effect of sildenafil (29).
bosentan, but not sildenafil, decreases catecholamines and
MCT-induced PHT was associated with a decrease in
BNP, reduces KW, and normalizes systemic hemodynam-
endothelium-dependent but not endothelium-independent
relaxation. This is in contrast with the report by Prie´ et al.
The combination of bosentan and sildenafil had
(30) of decreased smooth-muscle responsiveness to NO
additive effects on a number of variables, reflecting their
with maintained endothelium-dependent vasodilator ca-
different mechanism of action: bosentan antagonizes bind-
pacity. The study by Prie´ et al., however, was performed
in isolated lung preparations, which may explain the
A and ETB receptors; sildenafil increases cGMP
by PDE5 inhibition. Doses of bosentan and sildenafil that
discrepancy. Bosentan and sildenafil had favorable effects
moderately lowered MPAP, when given separately, further
on endothelial function assessed ex vivo, and their
lowered MPAP when given in combination. There was no
combination fully normalized endothelium-dependent re-
death in the combination group, whereas both bosentan and
laxation. ET-1 overexpression causes endothelial dysfunc-
sildenafil partially reduced the death rate as compared with
tion (31), and bosentan improves endothelium-dependent
untreated PHT rats. Although the study was not designed to
relaxation in various animal models (32, 33), human vessels
be a mortality study, these data suggest that combination
(34), and clinical situations (35, 36). Sildenafil increases NO
therapy was associated with a maximal survival rate. Both
signaling and increases endothelium-dependent relaxation in
bosentan and sildenafil inhibited the development of RV
hypertrophy, and there was a nonstatistically significant
Plasma concentrations of ET-1 increased in MCT rats,
trend for an added benefit of combined therapy. Bosentan is
consistent with a role of ET in the pathophysiology of PHT.
a potent inhibitor of cardiomyocyte hypertrophy in vitro and
They further increased in bosentan-treated rats because of
in vivo (21, 22), and sildenafil decreases cardiac hyper-
lack of binding of ET-1, in particular to the ETB receptor,
trophy by increasing cardiac cGMP content (23).
which is known to contribute to ET-1 clearance (40).
The current data with bosentan in MCT-induced PHT
However, the increase in circulating ET-1 by dual receptor
are in agreement with previous data obtained with bosentan
antagonists is not associated with any negative effects,
(13) and with another dual ET receptor antagonist,
because both ETA and ETB receptors are blocked. Sildenafil,
BSF420627 (14), which were shown to improve survival
by enhancing NO sensitivity, may modulate ET-1 production.
and decrease RV hypertrophy in MCT-treated rats. Studies
In conclusion, the results of the present study show
using PDE5 inhibitors also showed a survival benefit in an
additive effects of the combination bosentan plus sildenafil
for decreasing MPAP, reducing plasma catecholamines,
Neither bosentan nor sildenafil alone significantly
maintaining BW, ameliorating lung inflammation, and
reduced relative LW; however, a reduction in LW was
reducing mortality. These results suggest that combination
observed with the combination. The study, however, did not
therapy may have added beneficial effects. In the clinical
evaluate whether this effect was caused by a reduction in
setting, preliminary data indicate that combining bosentan
pulmonary edema, or by a decrease in pulmonary vascular
and sildenafil in idiopathic PAH patients is safe and
hypertrophy. Finally, there was a major effect of the
effective (41). Further studies will evaluate whether
combination on plasma concentrations of catecholamines,
combining sildenafil with bosentan brings additional clinical
norepinephrine in particular. Bosentan alone had a major
effect on norepinephrine concentration. This decrease incatecholamines has been described previously with dual
We thank Daniel Wanner, Hakim Hadana, Pauline Loriette, Virginie
Sippel, Shuangshuang Ding, and Josiane Rein for expert technical
levels increase in proportion to the extent of right ventricular
assistance, and Susan Flores for her editorial support.
dysfunction in pulmonary hypertension. J Am Coll Cardiol 31:202–208, 1998.
18. Weimann J, Ullrich R, Hromi J, Fujino Y, Clark MW, Bloch KD, Zapol
1. Rubin LJ. Primary pulmonary hypertension. N Engl J Med 336:111–
WM. Sildenafil is a pulmonary vasodilator in awake lambs with acute
pulmonary hypertension. Anesthesiology 92:1702–1712, 2000.
2. Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, Pulido
19. Nootens M, Kaufmann E, Rector T, Toher C, Judd D, Francis GS, Rich
T, Frost A, Roux S, Leconte I, Landzberg M, Simonneau G. Bosentan
S. Neurohormonal activation in patients with right ventricular failure
therapy for pulmonary arterial hypertension. N Engl J Med 346:896–
from pulmonary hypertension: relation to hemodynamic variables and
endothelin levels. J Am Coll Cardiol 26:1581–1585, 1995.
3. Channick RN, Simonneau G, Sitbon O, Robbins IM, Frost A, Tapson
20. Stinger RB, Iacopino VJ, Alter I, Fitzpatrick TM, Rose JC, Kot PA.
VF, Badesch DB, Roux S, Rainisio M, Bodin F, Rubin LJ. Effects of
Catheterization of the pulmonary artery in the closed-chest rat. J Appl
the dual endothelin-receptor antagonist bosentan in patients with
pulmonary hypertension: a randomised placebo-controlled study.
21. Harada M, Itoh H, Nakagawa O, Ogawa Y, Miyamoto Y, Kuwahara K,
Ogawa E, Igaki T, Yamashita J, Masuda I, Yoshimasa T, Tanaka I,
4. Ghofrani HA. The SUPER-1 study. Presented at: Late-breaking clinical
Saito Y, Nakao K. Significance of ventricular myocytes and non-
trial session. CHEST 2004, The 70th annual meeting of the American
myocytes interaction during cardiocyte hypertrophy: evidence for
College of Chest Physicians, Seattle, Washington, Oct. 27, 2004.
endothelin-1 as a paracrine hypertrophic factor from cardiac non-
5. Rossi GP, Seccia TM, Nussdorfer GG. Reciprocal regulation of
myocytes. Circulation 96:3737–3744, 1997.
endothelin-1 and nitric oxide: relevance in the physiology and
22. Kaddoura S, Firth JD, Boheler KR, Sugden PH, Poole-Wilson PA.
pathology of the cardiovascular system. Int Rev Cytol 209:241–272,
Endothelin-1 is involved in norepinephrine-induced ventricular hyper-
trophy in vivo. Acute effects of bosentan, an orally active, mixed
6. Meyrick B, Gamble W, Reid L. Development of Crotalaria pulmonary
endothelin ETA and ETB receptor antagonist. Circulation 93:2068–
hypertension: hemodynamic and structural study. Am J Physiol 239:
23. Hassan MA, Ketat AF. Sildenafil citrate increases myocardial cGMP
7. Hilliker KS, Bell TG, Roth RA. Pneumotoxicity and thrombocytopenia
content in rat heart, decreases its hypertrophic response to isoproterenol
after single injection of monocrotaline. Am J Physiol 242:H573–579,
and decreases myocardial leak of creatine kinase and troponin T. BMC
8. Lai YL, Olson JW, Gillespie MN. Ventilatory dysfunction precedes
24. Kodama K, Adachi H. Improvement of mortality by long-term E4010
pulmonary vascular changes in monocrotaline-treated rats. J Appl
treatment in monocrotaline-induced pulmonary hypertensive rats. J
Pharmacol Exp Ther 290:748–752, 1999.
9. Humbert M, Simonneau G. Sildenafil for pulmonary arterial hyper-
25. Mulder P, Richard V, Derumeaux G, Hogie M, Henry JP, Lallemand F,
tension: still waiting for evidence. Am J Respir Crit Care Med 169:6–7,
Compagnon P, Mace B, Comoy E, Letac B, Thuillez C. Role of
endogenous endothelin in chronic heart failure: effect of long-term
10. Miyauchi T, Yorikane R, Sakai S, Sakurai T, Okada M, Nishikibe M,
treatment with an endothelin antagonist on survival, hemodynamics,
Yano M, Yamaguchi I, Sugishita Y, Goto K. Contribution of
and cardiac remodeling. Circulation 96:1976–1982, 1997.
endogenous endothelin-1 to the progression of cardiopulmonary
26. Schalcher C, Cotter G, Reisin L, Bertel O, Kobrin I, Guyene TT,
alterations in rats with monocrotaline-induced pulmonary hypertension.
Kiowski W. The dual endothelin receptor antagonist tezosentan acutely
improves hemodynamic parameters in patients with advanced heart
11. Giaid A, Yanagisawa M, Langleben D, Michel RP, Levy R, Shennib H,
failure. Am Heart J 142:340–349, 2001.
Kimura S, Masaki T, Duguid WP, Stewart DJ. Expression of
27. Spieker LE, Mitrovic V, Noll G, Pacher R, Schulze MR, Muntwyler J,
endothelin-1 in the lungs of patients with pulmonary hypertension. N
Schalcher C, Kiowski W, Luscher TF. Acute hemodynamic and
neurohumoral effects of selective ET(A) receptor blockade in patients
12. Yoshibayashi M, Nishioka K, Nakao K, Saito Y, Matsumura M, Ueda
with congestive heart failure. ET 003 Investigators. J Am Coll Cardiol
T, Temma S, Shirakami G, Imura H, Mikawa H. Plasma endothelin
concentrations in patients with pulmonary hypertension associated with
28. Phillips BG, Kato M, Pesek CA, Winnicki M, Narkiewicz K, Davison
congenital heart defects. Evidence for increased production of
D, Somers VK. Sympathetic activation by sildenafil. Circulation 102:
endothelin in pulmonary circulation. Circulation 84:2280–2285, 1991.
13. Hess P, Clozel M, Clozel JP. Telemetry monitoring of pulmonary
arterial pressure in freely moving rats. J Appl Physiol 81:1027–1032,
29. Abbott D, Comby P, Charuel C, Graepel P, Hanton G, Leblanc B,
Lodola A, Longeart L, Paulus G, Peters C, Stadler J. Preclinical safetyprofile of sildenafil. Int J Impot Res 16:498–504, 2004.
14. Jasmin JF, Lucas M, Cernacek P, Dupuis J. Effectiveness of a
nonselective ET(A/B) and a selective ET(A) antagonist in rats with
30. Prie´ S, Stewart DJ, Dupuis J. Endothelin A receptor blockade improves
monocrotaline-induced pulmonary hypertension. Circulation 103:314–
nitric oxide-mediated vasodilation in monocrotaline-induced pulmo-
nary hypertension. Circulation 97:2169–2174, 1998.
15. Schermuly RT, Kreisselmeier KP, Ghofrani HA, Yilmaz H, Butrous G,
31. Amiri F, Virdis A, Neves MF, Iglarz M, Seidah NG, Touyz RM,
Ermert L, Ermert M, Weissmann N, Rose F, Guenther A, Walmrath D,
Reudelhuber TL, Schiffrin EL. Endothelium-restricted overexpression
Seeger W, Grimminger F. Chronic sildenafil treatment inhibits
of human endothelin-1 causes vascular remodeling and endothelial
monocrotaline-induced pulmonary hypertension in rats. Am J Respir
dysfunction. Circulation 110:2233–2240, 2004.
32. Wang QD, Li XS, Pernow J. The nonpeptide endothelin receptor
16. Yap LB. B-type natriuretic Peptide and the right heart. Heart Fail Rev
antagonist bosentan enhances myocardial recovery and endothelial
function during reperfusion of the ischemic rat heart. J Cardiovasc
17. Nagaya N, Nishikimi T, Okano Y, Uematsu M, Satoh T, Kyotani S,
Pharmacol 26(Suppl 3):S445–447, 1995.
Kuribayashi S, Hamada S, Kakishita M, Nakanishi N, Takamiya M,
33. Li XS, Wang QD, Pernow J. Beneficial effects of the endothelin
Kunieda T, Matsuo H, Kangawa K. Plasma brain natriuretic peptide
receptor antagonist bosentan on myocardial and endothelial injury
BOSENTAN AND SILDENAFIL IN PULMONARY HYPERTENSIVE RATS
following ischaemia/reperfusion in the rat. Eur J Pharmacol 283:161–
mediated vasodilation in patients with chronic heart failure. J Am Coll
34. Verma S, Lovren F, Dumont AS, Mather KJ, Maitland A, Kieser TM,
38. Halcox JP, Nour KR, Zalos G, Mincemoyer RA, Waclawiw M, Rivera
Kidd W, McNeill JH, Stewart DJ, Triggle CR, Anderson TJ.
CE, Willie G, Ellahham S, Quyyumi AA. The effect of sildenafil on
Endothelin receptor blockade improves endothelial function in human
human vascular function, platelet activation, and myocardial ischemia.
internal mammary arteries. Cardiovasc Res 49:146–151, 2001.
J Am Coll Cardiol 40:1232–1240, 2002.
39. Gori T, Sicuro S, Dragoni S, Donati G, Forconi S, Parker JD. Sildenafil
35. Bo¨hm F, Settergren M, Gonon AT, Pernow J. The endothelin-1
prevents endothelial dysfunction induced by ischemia and reperfusion
receptor antagonist bosentan protects against ischaemia/reperfusion-
via opening of adenosine triphosphate-sensitive potassium channels: a
induced endothelial dysfunction in humans. Clin Sci (Lond) 108:357–
human in vivo study. Circulation 111:742–746, 2005.
40. Lo¨ffler BM, Breu V, Clozel M. Effect of different endothelin receptor
36. Girgis RE, Champion HC, Diette GB, Johns RA, Permutt S, Sylvester
antagonists and of the novel non-peptide antagonist Ro 46–2005 on
JT. Decreased exhaled nitric oxide in pulmonary arterial hypertension:
endothelin levels in rat plasma. FEBS Lett 333:108–110, 1993.
response to bosentan therapy. Am J Respir Crit Care Med, 172:352–
41. Hoeper MM, Faulenbach C, Golpon H, Winkler J, Welte T,
Niedermeyer J. Combination therapy with bosentan and sildenafil in
37. Katz SD, Balidemaj K, Homma S, Wu H, Wang J, Maybaum S. Acute
idiopathic pulmonary arterial hypertension. Eur Respir J 24:1007–
type 5 phosphodiesterase inhibition with sildenafil enhances flow-
RESUMEN DE LAS CARACTERÍSTICAS DEL PRODUCTO NOMBRE DEL MEDICAMENTO Qlaira comprimidos recubiertos con película. COMPOSICIÓN CUALITATIVA Y CUANTITATIVA Cada envase calendario contiene 28 comprimidos recubiertos con película, en el siguiente orden: - 2 comprimidos de color amarillo oscuro. Cada comprimido contiene 3 mg de valerato de estradiol - 5 comprimidos de color rojo intermedi
AIRPORTS AUTHORITY OF INDIA (A Mini Ratna – Category – 1 Public Sector Enterprise) Advt.No. 2/2012 Airports Authority of India invites applications from the eligible candidates to apply ON-LINE through AAI’s website www.aai.aero for the following posts (NO APPLICATION THROUGH OTHER MODE WILL BE ACCEPTED. Event Date Opening date for On-line Registration Last date of receipt
 BOSENTAN AND SILDENAFIL IN PULMONARY HYPERTENSIVE RATS
Figure 1. Effect of chronic oral administration of bosentan, sildenafil, and their combination on (A) MPAP in anesthetized rats; and (B) on RVhypertrophy, measured as the ratio of RV weight to BW, 4 weeks after MCT injection. CTR, control; MCT, MCT alone; Bos, bosentan; Sil,sildenafil. þþþP , 0.001 versus control; **P , 0.01 versus MCT alone; ***P , 0.001 versus MCT alone.
BOSENTAN AND SILDENAFIL IN PULMONARY HYPERTENSIVE RATS
Figure 1. Effect of chronic oral administration of bosentan, sildenafil, and their combination on (A) MPAP in anesthetized rats; and (B) on RVhypertrophy, measured as the ratio of RV weight to BW, 4 weeks after MCT injection. CTR, control; MCT, MCT alone; Bos, bosentan; Sil,sildenafil. þþþP , 0.001 versus control; **P , 0.01 versus MCT alone; ***P , 0.001 versus MCT alone.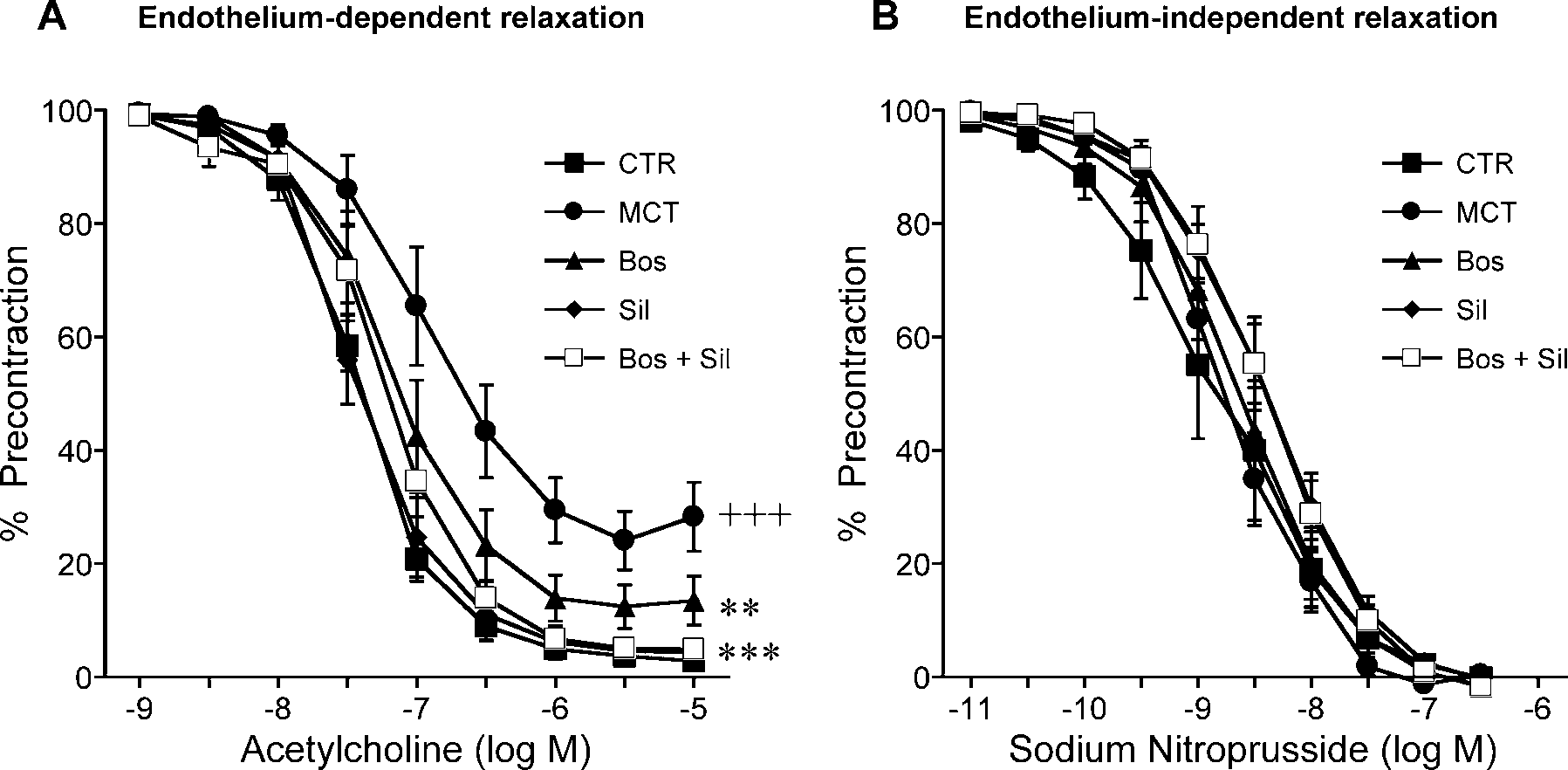 Figure 2. Effect of chronic oral administration of bosentan, sildenafil, and their combination on endothelium-dependent and independentrelaxation, measured in aortic ring segments isolated from rats 4 weeks after MCT injection. (A) The concentration-response curves in responseto acetylcholine (endothelium-dependent relaxation). (B) The concentration-response curves in response to sodium nitroprusside (endothelium-independent relaxation). CTR, control; MCT, MCT alone; Bos, bosentan; Sil, sildenafil. þþþP , 0.001 versus control; **P , 0.01 versus MCTalone; ***P , 0.001 versus MCT alone.
Figure 2. Effect of chronic oral administration of bosentan, sildenafil, and their combination on endothelium-dependent and independentrelaxation, measured in aortic ring segments isolated from rats 4 weeks after MCT injection. (A) The concentration-response curves in responseto acetylcholine (endothelium-dependent relaxation). (B) The concentration-response curves in response to sodium nitroprusside (endothelium-independent relaxation). CTR, control; MCT, MCT alone; Bos, bosentan; Sil, sildenafil. þþþP , 0.001 versus control; **P , 0.01 versus MCTalone; ***P , 0.001 versus MCT alone.