Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Drug-induced long qt syndrome
Hellenic J Cardiol 48: 296-299, 2007 Drug-Induced Long QT Syndrome K
ONSTANTINOS P. LETSAS , MICHALIS EFREMIDIS , GERASIMOS S. FILIPPATOS ,
1Second Department of Cardiology, Evangelismos General Hospital of Athens, 2Second Department of Cardiology,Atticon University Hospital of Athens, Athens, Greece.
Key words: Drugs, long QT, torsades de pointes, sudden cardiac A continuously growing number of ing drug-induced LQTS, as well as the
identification of easily recognised risk fac-
tors that predispose to this potentially life-
polarisation, predisposing to a certain type
of polymorphic ventricular tachycardiatermed torsades de pointes (TdP) and sud-
Measurement of the QT interval
den cardiac death.1-5 Drug-induced long QTsyndrome (LQTS) is considered the most
frequent cause of withdrawal or relabelling
of marketed drugs in the last decade.5 Drugs
with proven lengthening of the QT interval
gram (ECG). Despite the fact that there are
or a definite association with TdP are com-
insufficient data regarding which lead or
mon and are estimated to comprise approxi-
leads to use for QT interval measurement,
mately 2-3% of all prescriptions written.6 As
lead II is considered the appropriate one
because the vectors of repolarisation result
in a long single wave rather than discrete T
LQTS and, in the vast majority of cases, are
enced by the heart rate. Rate acceleration
prescribed by non-cardiologists.1,5,7 This list
bradycardia leads to QT lengthening.10 The
should be measured for rate correction.10,11
Several formulae may be used to correct the
25, 28th Octovriou St. 15235 Athens, Greece
used formulae are Fridericia’s cube root
k.letsas@mail.gr
prolonging agents has recently been asso-
ciated with a significantly increased risk of
square root formula (QTc = QT/RR1/2).
sudden cardiac death in the general popu-
Fridericia’s equation is preferred at ex-
Apart from heart rate, the duration of the
starters.8 However, the likelihood of drug-
QT interval is also influenced by sympatho-
induced TdP is difficult to predict in rou-
vagal activity, drugs, genetic abnormalities,
tine clinical practice. The present brief re-
electrolyte disorders, cardiac or metabolic
diseases and changes of cardiac afterload.11
296 ñ HJC (Hellenic Journal of Cardiology) Drug-Induced Long QT Syndrome Table 1. Drugs implicated in drug-induced long QT syndrome.
Disopyramide, procainamide, quinidine, mexiletine, propafenone, flecainide, d,l-sotalol, amiodarone,bretylium, dofetilide, ibutilide, azimilide, ajmaline
Erythromycin, clarithromycin, azithromycin, levofloxacin, moxifloxacin, sparfloxacin, gatifloxacin,grepafloxacin, trimethoprim-sulfamethoxazole, pentamidine, quinine, itraconazole, ketoconazole, flu-conazole, chloroquine, halofantrine, mefloquine, amantadine, spiramycin
Astemizole, diphenhydramine, ebastine, terfenadine, hydroxyzine
Doxepin, venlafaxine,fluoxetine, desipramine, imipramine, clomipramine, paroxetine, sertraline, citalo-pram
Chlorpromazine, prochlorperazine, trifluoperazine, fluphenazine, felbamate, haloperidol, thioridazine,droperidol, mesoridazine, pimozide, risperidone, quetiapine, ziprasidone, lithium, chloral hydrate, pericy-cline, sertindole, sultopride, zimeldine, maprotiline
Arsenic trioxide, aconitine, veratridine, vincamine, terodiline, budipine, tizanidine tiapride, cocaine,organophosphorus compounds
QTc values greater than 450 ms in men and 470 ms
ing oscillations in membrane voltage during phases 2
in women are considered abnormal. Values ranging
and 3 of the action potential.15-17 Early afterdepolar-
between 430-450 ms in men and 450-470 ms in
isations that reach the threshold voltage cause ven-
women are considered borderline.11 The QTc interval
tricular extrasystoles. These phenomena are more
is the best available predictor of TdP episodes.12 The
readily induced in the His-Purkinje network and also
majority of drug-induced TdP occur with QTc values
in M cells from the mid-ventricular myocardium.15-17
of more than 500 ms.13 Data from patients with con-
Compared to subendocardial or subepicardial cells,
genital LQTS have shown that a QTc interval greater
M cells show a much more pronounced action poten-
than 500 ms is associated with an increased risk for
tial prolongation in response to IKr blockade.15-17 The
arrhythmic events.14 However, there is no established
resultant heterogeneity in ventricular repolarisation
threshold below which prolongation of the QTc inter-
creates a zone of functional refractoriness in the mid
val is considered free of proarrhythmic events.
myocardial layer, which is probably the basis of there-entry that sustains the TdP.15-17 Many drugs blockmultiple cardiac ion channels (I
Mechanisms of drug-induced arrhythmia
a more complex shift of action potential morpho-
The majority of non-cardiac QT-prolonging agents
exhibit direct electrophysiological effects on the ra-
Furthermore, pharmacokinetic interactions with
pidly activating delayed rectifier (repolarising) po-
drugs known to inhibit cytochrome P450 isoenzymes
tassium current (IKr) encoded by the human ether-a-
(mainly CYP3A4) enhance the torsadogenic potential
go-go-related gene (HERG, now termed KCNH2).1,5
of these agents by decreasing their clearance.1,5,15
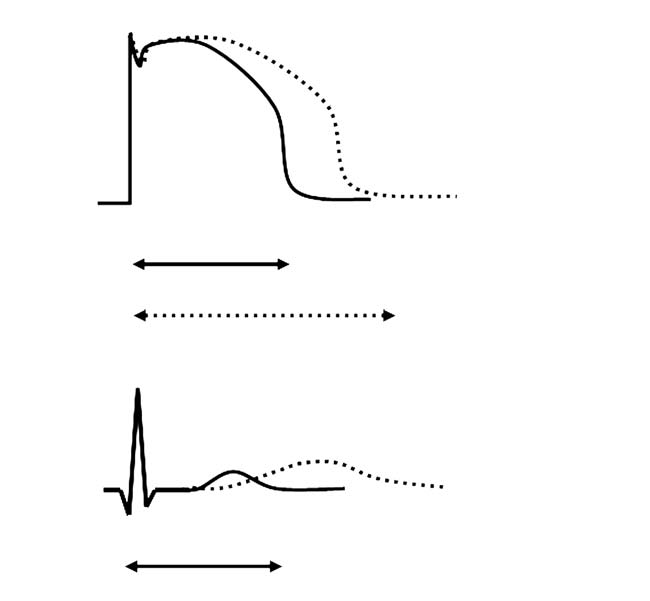
As shown in Figure 1, IKr blockade leads to a delay
CYP3A4 activity can be inhibited by a wide variety of
in phase 3 of repolarisation of the action potential
drugs including some macrolide antibiotics, ketocona-
(reflected as QT interval prolongation on the sur-
zole and related antifungals, cimetidine, fluoxetine,
face ECG). Activation of inward depolarising cur-
protease inhibitors, and amiodarone. In addition,
rents (most likely L-type calcium channels or sodi-
many non-drug factors, including age, smoking, he-
um-calcium exchange current) may then give rise to
patic disease, genetic polymorphisms and grapefruit
early afterdepolarisations that appear as depolaris-
(Hellenic Journal of Cardiology) HJC ñ 297 K.P. Letsas et al Figure 1. Relationship between the phases of ventricular transmembrane action potential (AP) and the surface electrocardiogram (ECG). A reduction of outward currents (IKr, IKs) during phases 2 and 3 of the AP leads to QT interval prolongation. Activation of in- ward depolarising currents (ICa, INa/Ca) may then give rise to early afterdepolar- isations (EADs). Risk factors for drug-induced long QT syndrome Table 2. Risk factors for drug-induced long QT syndrome.
The susceptibility to drug-induced LQTS varies signif-
icantly among individuals. The unifying concept of
“reduced cardiac repolarisation reserve” has been
proposed to explain the mechanism by which some pa-
Electrolyte imbalances (hypokalaemia, hypomagnesaemia, hypo-calcaemia)
tients are rendered more susceptible than others to
the QT-prolonging effects of drugs.5,15,16 Silent muta-
tions and/or polymorphisms in genes encoding cardiac
ion channels leading to a reduced cardiac repolarisa-
Cardiac hypertrophyAnorexia nervosa, starvation
tion reserve hold the key to understanding why heal-
thy individuals will be exposed to risk for LQTS when
taking medication for unrelated causes.5,15,16,18-20 Ge-
netic analyses have identified the subclinical congenital
Cytochrome P450 isoenzyme CYP3A4 inhibitors Baseline QT interval prolongation
form in 5-10% of patients with drug-induced LQTS.19
Mutations have been reported in KCNQ1, KCNH2,
KCNE1, KCNE2 and SCN5A genes.5,15,16,18-20 There-fore, the administration of an IKr current blockingagent may significantly prolong the QT interval in
diomyopathies, bradycardia, electrolyte imbalance
these silent carriers, predisposing them to TdP and
(hypokalaemia, hypomagnesaemia, hypocalcaemia),
digitalis therapy, hypothermia, and hypothyroi-
The likelihood of drug-induced LQTS is difficult
dism.1,5,7,10,11,15,16 The vast majority of patients with
to predict in routine clinical practice. However, clini-
drug-induced TdP display at least one of these risk
cal history may reveal well-established risk factors
factors. It has been estimated that approximately 70%
that act as “effect amplifiers”, making an otherwise
of cases of drug-induced TdP occur in females.21 A
relatively safe drug dangerous with regard to risk for
reduced cardiac repolarisation reserve closely related
TdP (Table 2). These risk factors include female gen-
to sex steroids has been proposed to explain the in-
der, cardiac hypertrophy, chronic heart failure, car-
creased propensity of women to develop drug-in-
298 ñ HJC (Hellenic Journal of Cardiology) Drug-Induced Long QT Syndrome
duced TdP.21 Testosterone, by increasing I
5. Roden DM: Drug-induced prolongation of the QT interval.
currents, shortens the QT interval and reduces the
6. De Ponti F, Poluzzi E, Montanaro N, Ferguson J: QTc and
risk of TdP in males.22 Polypharmacy should also be
psychotropic drugs. Lancet 2000; 356: 75-76.
considered as a risk factor for drug-induced LQTS.
7. Heist EK, Ruskin JN: Drug-induced proarrhythmia and use
An analysis of medication lists from 1.1 million pa-
of QTc-prolonging agents: clues for clinicians. Heart Rhythm
tients showed that 22.8% were taking at least one
8. Straus SM, Sturkenboom MC, Bleumink GS, et al: Non-car-
medication with potential for QT prolongation, 9.4%
diac QTc-prolonging drugs and the risk of sudden cardiac
were taking two such medications, and 0.7% were
death. Eur Heart J 2005; 26: 2007-2012.
taking three or more QT-prolonging drugs. Psy-
9. Garson A Jr: How to measure the QT interval - what is nor-
chotropic drugs were involved in 50% of cases.23
10. Viskin S, Justo D, Halkin A, Zeltser D: Long QT syndrome
caused by noncardiac drugs. Prog Cardiovasc Dis 2003; 45:415-427. Conclusions
11. Yap YG, Camm AJ: Drug induced QT prolongation and tor-
Drug-induced LQTS should always be considered as
sades de pointes. Heart 2003; 89: 1363-1372.
12. Algra A, Tijssen JG, Roelandt JR, Pool J, Lubsen J: QTc
a predictor of sudden cardiac death, and should thus
prolongation measured by standard 12-lead electrocardiogra-
prompt a critical revaluation of the risks and benefits
phy is an independent risk factor for sudden death due to car-
of the suspicious medication. In clinical practice, ad-
diac arrest. Circulation 1991; 83: 1888-1894.
verse effects of QT-prolonging drugs can be prevent-
13. Bednar MM, Harrigan EP, Ruskin JN: Torsades de pointes
associated with nonantiarrhythmic drugs and observations on
ed by not exceeding the recommended dose, by re-
gender and QTc. Am J Cardiol 2002; 89: 1316-1319.
stricting the dose in patients with pre-existing risk fac-
14. Priori SG, Schwartz PJ, Napolitano C, et al: Risk stratifica-
tors, and by avoiding the concomitant administration
tion in the long-QT syndrome. N Engl J Med 2003; 348: 1866-
of agents that inhibit the metabolism of known drugs
that prolong the QT interval. Survivors of drug-in-
15. Gupta A, Lawrence AT, Krishnan K, Kavinsky CJ, Trohman
RG: Current concepts in the mechanisms and management
duced TdP and family members of drug-induced TdP
of drug-induced QT prolongation and torsade de pointes.
fatalities require careful examination and possibly ge-
netic testing for the presence of an LQTS-associated
16. Kannankeril PJ, Roden DM: Drug-induced long QT and tor-
channelopathy. The field of pharmacogenetics may
sade de pointes: recent advances. Curr Opin Cardiol 2007;22: 39-43.
provide further insight into how mutations and poly-
17. Antzelevitch C: Role of transmural dispersion of repolariza-
morphisms in genes encoding cardiac ion channels
tion in the genesis of drug-induced torsades de pointes. Heart
modulate the response to certain therapeutic agents.
18. Priori SG, Napolitano C, Schwartz PJ: Low penetrance in the
long-QT syndrome: clinical impact. Circulation 1999; 99: 529-533. References
19. Yang P, Kanki H, Drolet B, et al: Allelic variants in long-QT
disease genes in patients with drug-associated torsades de
1. Gowda RM, Khan IA, Wilbur SL, Vasavada BC, Sacchi TJ:
pointes. Circulation 2002; 105: 1943-1948.
Torsade de pointes: the clinical considerations. Int J Cardiol
20. Priori SG, Cerrone M: Molecular genetics: is it making an
impact in the management of inherited arrhythmogenic syn-
2. Letsas KP, Filippatos GS, Kounas SP, Efremidis M, Sideris
dromes? Hellenic J Cardiol 2005; 46: 83-87.
A, Kardaras F: QT interval prolongation and torsades de
21. Zeltser D, Justo D, Halkin A, Prokhorov V, Heller K, Viskin
pointes in a patient receiving zolpidem and amiodarone. Car-
S: Torsade de pointes due to noncardiac drugs: most patients
have easily identifiable risk factors. Medicine (Baltimore)
3. Kounas SP, Letsas KP, Sideris A, Efraimidis M, Kardaras F:
QT interval prolongation and torsades de pointes due to a
22. Arya A: Gender-related differences in ventricular repolariza-
coadministration of metronidazole and amiodarone. Pacing
tion: beyond gonadal steroids. J Cardiovasc Electrophysiol
Clin Electrophysiol 2005; 28: 472-473.
4. Letsas K, Korantzopoulos P, Pappas L, Evangelou D, Efre-
23. Curtis LH, Ostbye T, Sendersky V, et al: Prescription of QT-
midis M, Kardaras F: QT interval prolongation associated with
prolonging drugs in a cohort of about 5 million outpatients.
venlafaxine administration. Int J Cardiol 2006; 109: 116-117.
(Hellenic Journal of Cardiology) HJC ñ 299
Chapter Two Most undergraduate research papers, and many graduate andprofessional research papers as well, are based upon libraryresearch. Library research can proceed smoothly if you follow a se-quence of simple steps. Your first task is to decide upon a topic for a paper. This is, in a sense,the most important task because the paper can be no better than thetopic. I have found five mista
CON DIO, CONTRO DIO, MAI SENZA DIO “.Ai miei studenti, per valutare lo scenario teologico, io suggerisco un criterio estremamente semplice ma anche davvero esigente: chiedetevi se la teologia che state imparando possa rimanere la stessa sia prima che dopo Auschwitz. Se la risposta è affermativa, state in guardia” (Johann Baptist Metz) Di fronte al problema del male che nella s
 K.P. Letsas et al
K.P. Letsas et al