Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Impact of the medicare prescription drug benefit on home- andcommunity- based services waiver programs
APRIL 2005
Impact of the Medicare PrescriptionDrug Benefit on Home- and Community-Based Services Waiver Programs
C har le s J. M i l l i gan, J r. , J. D. , M . P. H .
C e nte r f or H ealth P rog ram D eve lop m e nt and M anag e m e nt
U nive r sity of M ary land, Balti more C ounty
ABSTRACT: “Dual eligibles” is the term for the 6.4 million low-income, elderly, and
disabled Americans who are enrolled in both Medicare and Medicaid.With home- and
Charles J. Milligan, Jr., J.D., M.P. H.
community-based services waivers allowed under Section 1915(c) of the Social
Security Act, many of these individuals are able to live in a home or community set-
ting, thereby avoiding institutionalization. Surveying Maryland’s 3,180 dual eligibles
who are enrolled in home- and community-based waiver programs, the author finds
that the end-of-2005 transfer of prescription drug coverage from Medicaid to Medicare
under the Medicare Modernization Act of 2003 could put these beneficiaries in jeop-
ardy. Maryland’s experience is likely to be typical of what other states will face. Theauthor recommends a number of federal policy remedies, among them allowing 90-dayprescriptions, using open or shared formularies, and lengthening the enrollment period.
The term “dual eligibles” refers to those low-income, elderly people anddisabled individuals who are enrolled in both Medicare and Medicaid. InJanuary 2006, responsibility for providing prescription drug coverage for thenation’s 6.4 million dual eligibles will transfer from Medicaid to Medicare,
as stipulated by the Medicare Modernization Act of 2003. Those who are
nursing-home-certified and participating in home- and community-based
services (HCBS) waiver programs face particular challenges with the transi-
tion to the new Medicare Part D prescription benefit. This issue brief is based on a presentation at the October 2004 Invitational Summit for StatePolicymakers on Medicare Part D Implementation Issues, convened by AcademyHealth and theRutgers Center for State Health Policy and sponsored in part by The Commonwealth Fund.
HCBS waiver participants are receiving an
percent of Medicaid beneficiaries were dual eligi-
enriched Medicaid benefit package to help them
bles, they accounted for 42 percent of Medicaid
avoid institutionalization and remain in the commu-
spending. Eighteen percent of Medicare benefici-
nity. Participants typically receive a full complement
aries were dual eligibles, with per capita spending
of prescription drugs that, together with home-
of $18,100, more than twice that for other
maker services, case management, personal attendant
Medicare beneficiaries. In 2002, 65 percent ($58
services, and other care, enable these individuals to
billion) of Medicaid expenditures for dual eligibles
function in a home or community setting. Without
went for long-term care. Nationally, prescription
thoughtful planning and the elimination of admin-
drug spending for dual eligibles in 2002 totaled
istrative barriers, the changeover to Medicare Part D
$13 billion, or 14 percent of total Medicaid spend-
poses risks for dual eligibles in HCBS waiver programs.
ing, while state per capita spending on prescribed
This issue brief examines the likely impact
of the new prescription drug benefit on HCBSdual eligibles in the state of Maryland as these
individuals move from Medicaid to Medicare cov-
erage. In Maryland, access to needed medications
HCBS programs operate through waivers granted
may be impeded, both in the short and long term;
by the U.S. Department of Health and Human
case managers are likely to be overburdened; and a
Services under Section 1915(c) of the Social
nonalignment of incentives across Medicaid and
Security Act. Certain Medicaid requirements are
Medicare may compromise the basic premise of
waived under these programs to enable states to
HCBS waiver programs—to enable very sick and
provide a range of home-based services to individ-
disabled people to remain in a community setting.
uals who might otherwise be institutionalized,
The anticipated scenario in Maryland exemplifies
while continuing to receive federal matching funds.
the challenges all states will face in making the
To receive waiver approval, states must demon-
transition to Medicare Part D a smooth one.
strate cost neutrality—that is, waiver program costsmust be no greater than the cost of institutional
Dual Eligibles: Health Status and Spending
care. States are required to limit the number of par-
Of the nation’s 6.4 million dual eligibles, two-thirds
ticipant “slots,” and they have the discretion to set
are age 65 or older and one-third are nonelderly
medical and financial eligibility criteria, cap spend-
adults with disabilities. Dual eligibles tend to be
ing, and limit availability to certain population
sicker and more impoverished than other Medicare
groups or geographic areas. In 2001, the most recent
beneficiaries. Nationally, 71 percent of dual eligibles
year for which aggregate data are available, 49 states
live on annual incomes of $10,000 or less. Both
were operating 231 HCBS waiver programs with
elderly and nonelderly dual eligibles require more
843,000 participants.3 Of these, 94 waiver programs
assistance with activities of daily living (ADLs).
served 489,000 aged and disabled participants.4 No
Elderly dual eligibles report more chronic disease
reliable national estimates are available for the
and are more likely to be in a nursing facility.1
number of dual eligibles enrolled in HCBS pro-
grams for the elderly and disabled. However, extrap-
disabled and more often suffer from chronic and
olating Maryland’s experience to the national
debilitating health conditions, they consume pro-
enrollment data that are available suggests that some
portionately more medical care, prescription drugs,
425,000 HCBS participants are dual eligibles.
and support services. Combined Medicare andMedicaid spending on dual eligibles totaled $106
billion in 2000. In that same year, while only 16
In FY2004, 3,180 dual eligibles were enrolled intwo 1915(c) waiver programs in Maryland:
I m pac t of th e M e di care P re sc ri p ti on D ru g B e ne f it on H om e - and C om munity - Base d S e rvi c e s Waive r P rog ram s
Older Adults Waiver (OAW). Available to
Table 1. Dual Eligibles in Maryland’s HCBS
low-income adults who are at least 50 years old
and qualify for nursing facility level of care. In
Enrollees Eligibles
Maryland residents in FY2004. Ninety percent
of participants were dual eligibles (Table 1). The
benefit package includes case management, per-
sonal care, home health care, personal emergency
response systems, home-delivered meals, con-
Source: UMBC analysis of Maryland Medicaid data.
sumer and family training, nutritionist services,home modifications, and assistive devices.
was prescribed for one-third of waiver participants. Other drugs to lower blood pressure and high
Living at Home: Maryland Community Choices (LAH). Available to low-income peo-
cholesterol are frequently prescribed (Lisinopril,
ple with disabilities between the ages of 21 and
Norvasc, Lipitor), as are antibiotics (Cipro, Zithromax),
59 who qualify for nursing facility level of care.
Prevacid (for acid reflux disease), Zoloft (for
LAH began in 2001 and enrolled 446 individu-
depression), and Ambien (for sleep disorders).
als in FY2004. Sixty-three percent of partici-
Overall, Maryland’s 3,180 dual-eligible
pants were dual eligibles. Covered services are
waiver participants received a total of 220,884 pre-
similar to those for OAW, with the addition of
scriptions in FY2004, for an average of almost 70
training and supervision of attendants, occupa-
prescriptions per beneficiary. Seventy-one percent
tional therapy, speech and language services, and
of dual eligibles required four or more prescrip-
disposable medical supplies not normally cov-
tions per month, and almost 10 percent required
12 or more prescriptions per month (Figure 1).
Not only do these beneficiaries require a
large number of prescriptions, but the formulary
to meet their needs must include a wide range ofmedications. In FY2004, Maryland’s dually eligible
Drug Formularies
waiver participants required and received 1,645
Access to an extensive formulary of prescription
different (unduplicated) kinds of prescription
drugs is essential to enabling dual eligibles partici-pating in Maryland’s OAW and LAH programs to
Table 2. Top 10 Drugs Prescribed to Maryland’s
remain in the community. In FY2004, prescription
drug expenditures for dually eligible OAW and
LAH participants totaled $13.8 million, or 91 per-
Beneficiaries
cent of total prescription drug expenditures for
participants in these waiver programs. More indica-
tive of the importance of prescription drugs to this
population is the actual quantity and variety of
medications prescribed. Table 2 lists the 10 most
prescribed drugs in FY2004 and how many bene-
ficiaries received at least one prescription of each
drug. The most widely prescribed drug among
dual-eligible waiver participants was Furosemide.
This diuretic, which is used to treat hypertension,
Source: UMBC analysis of Maryland Medicaid data.
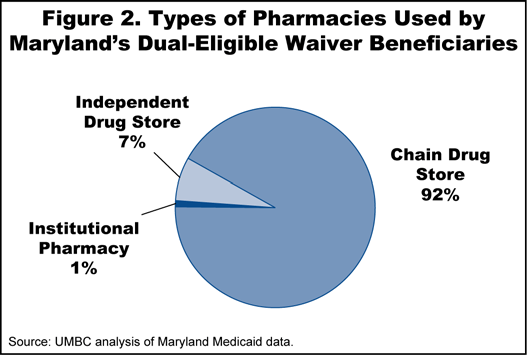
a way to provide access to that drug during theappeal process or until which time the patient’sneeds can be reassessed by a Medicare-approvedphysician and alternative, formulary-approveddrugs can be prescribed? If not, community-baseddual eligibles whose drugs have not been approvedmay be at risk of medical complications and evenhospitalization or institutionalization. Prescription Drug Distribution Channels Under Medicare Part D, it is possible that Medicare-approved drug plans will contract with a more limited network of pharmacies than what is currently available to Maryland’s dual-eligible waiver participants. This may impede the ability of infirm and disabled dual eligibles to continue obtaining prescription drugs from their neighbor- hood pharmacy. As shown in Figure 2, Maryland’s
medications. Moreover, 400 of these 1,645 med-
dual-eligible waiver beneficiaries receive prescrip-
ications were prescribed for one beneficiary only.
tions from a variety of outlets—chain drug stores,
To ensure a smooth transition to Medicare
independent drug stores, and institutional pharma-
Part D prescription drug coverage, Medicare drug
cies—and virtually all the pharmacies in the state
plans must be prepared to offer dual eligibles a for-
participate in the Medicaid program. Under a new
mulary of drugs that is equivalent to the Medicaid
Medicare prescription drug plan, waiver partici-
formulary. The Medicare Modernization Act of
pants may be forced to establish accounts with
2003 anticipates that drug plans will include the
new pharmacies, possibly having to travel further
use of formularies to manage drug benefits, and
Medicare will establish a therapeutic classification
In addition, Medicare drug plans are likely
system to serve as the basis for plan formularies.
to encourage filling prescriptions by mail because
The law also requires that the plan and in particu-
the law allows plans lower cost-sharing for mail-
lar its formulary cannot discourage enrollment of
order drugs. Overreliance on mail-order for main-
certain beneficiaries.5 However, the extent to
tenance medications could prove problematic for
which drug plan formularies will meet the needsof HCBS waiver participants remains to be seen.
Services now plans to auto-enroll dual eligibles ina drug plan by mid-December 2005. This isintended to give the Medicare drug plans leadtime to approve medications by January 1, 2006,and guarantee continuity of coverage. However,given the number of medications required bywaiver participants, will this be adequate time?What if an individual is using a drug that isexcluded from the drug plan’s formulary? Is there
I m pac t of th e M e di care P re sc ri p ti on D ru g B e ne f it on H om e - and C om munity - Base d S e rvi c e s Waive r P rog ram s
waiver participants. It is well documented that
coordinating benefits among multiple providers
Medicaid beneficiaries move frequently, are more
and formularies, and negotiating timely receipt of
likely to rent than own a home or apartment, and
medications from diverse vendors. After the transi-
oftentimes are without a permanent mailing
tion to Medicare Part D, case managers will retain
address. As a result, automatic monthly drug mail-
responsibility for dual eligibles but no longer have
ings risk not reaching the beneficiary.
access to dual eligibles’ drug records from theMedicare prescription drug provider, making it more
Transportation to the Pharmacy
difficult for case managers to coordinate long-term
In Maryland, Medicaid covers beneficiary trans-
supports and services. All of this is likely to signifi-
portation costs for nonemergency transportation to
cantly increase case manager workloads, putting
obtain Medicaid-covered benefits. This means that
pressure on HCBS programs to reduce caseload
HCBS waiver participants are currently provided
ratios, which would in turn place upward pressure
with transportation to the pharmacy to pick up
on Medicaid payment rates for HCBS programs.
Under Medicare Part D, dual-eligible waiver
Incentive Nonalignment Across Payers
participants will no longer be eligible to receive
Successfully managing very sick individuals at
transportation to the pharmacy because they will
home or in the community as HCBS programs
no longer be traveling to the drug store to obtain a
strive to do requires a full complement of pre-
Medicaid benefit. This may be especially problem-
scription drugs. Unlike HCBS programs, however,
atic for waiver participants if their Medicare drug-
the Medicare program as currently structured
plan-approved pharmacies are farther from home.
offers few incentives to avoid long-term institu-
Consequently, waiver participants may delay pick-
tionalization. Medicare pays only for short-term,
ing up prescriptions until they can afford a taxi or
post-hospital discharge stays in skilled nursing
arrange for a ride from a family member or friend.
facilities. Private insurance, the patient’s own funds,
State Medicaid programs will have the option of
or Medicaid finance other long-term expenditures.
retaining the transportation benefit for dual eligi-
Consequently, Medicare prescription drug plans
bles, but without federal cost-sharing.
may be less inclined to approve drugs that benefi-ciaries need to remain in the community, and it is
Pressure on HCBS Case Managers
possible that formularies will not even include all
Case managers who arrange for and monitor ser-
of the drugs that HCBS participants require. Even
vices received by HCBS waiver participants in
if certain drugs are included in the prescription
Maryland generally do not have to coordinate
drug plan’s formulary, dosage form restrictions
access to prescription drugs across multiple health
(e.g., a tablet versus a liquid) may limit access for
plans and formularies. During the transition to
HCBS beneficiaries. Moreover, in addition to pre-
Medicare Part D, these Medicaid case managers will
scription drugs, HCBS waiver participants typically
find themselves dealing not just with Medicaid, but
require a number of over-the-counter drugs,
also with a number of Medicare drug plans, each
which are currently covered by Medicaid. The
with its own formulary, distribution channels, and
new Medicare Part D prescription drug benefit
cost-sharing requirements. Case managers will be
does not cover over-the-counter drugs.
on the front lines, ensuring continuity of prescrip-tion drug coverage for their clients during the
transition from Medicaid to Medicare. They will be
Clearly, the drug formularies offered by Medicare
thrust into the role of educating clients and their
prescription drug plans will matter if dual eligibles
caregivers about the new Medicare drug benefit,
participating in HCBS waiver programs are to
receive the prescription drugs they need to remain
Require Medicare prescription drug plans
at home or in the community. The networks of
to offer dual eligibles open formularies or
pharmacies participating in Medicare prescription
Medicaid-equivalent formularies during
drug plans must be broad enough to ensure easy
the first six months to a year. This would in
access to an approved pharmacy, particularly if
essence lengthen the transition period for dual
waiver participants are to lose their Medicaid trans-
eligibles, allowing more time to consult with an
portation benefit after the transition to Medicare.
in-network Medicare physician, align prescrip-
HCBS case managers will require training and other
tion needs, and acquire approvals under the
supports to see them through the transition period.
Thereafter, caseloads will require careful monitoring
Require Medicare prescription drug plans
to guard against case manager stress and overload. to honor a beneficiary’s existing pharmacy regimen until an in-network physician
shortcomings and administrative holdups during
develops a new care plan. In effect, if
the transition period, the Centers for Medicare and
Medicare is obligated to approve a beneficiary’s
Medicaid Services has included in the rules for the
drug regimen until the beneficiary is seen by a
new Medicare law “formulary review for certain
physician, the beneficiary will be insulated from
diseases, medical necessity coverage of nonformu-
some of the transition effects. This form of
lary drugs, and plan-specific transition procedures
“grandparent” protection is necessary.
to further ensure that dual-eligible beneficiarieswill get the drugs they need.”6
Allow states to pick up the cost of noncov-
But states and beneficiaries are demanding
ered drugs with full federal matching funds
more. The following interim measures, together or
and be eligible for a credit to the state
in part, would serve to further ease the transition
“clawback.” The rules issued by the Centers for
for dual eligibles as they move from Medicaid to
Medicare and Medicaid Services in January 2005
state that “states may continue to cover drugs fordual eligibles not covered by the Medicare pre-
Allow states to dispense 90-day prescrip-
scription drug benefit and receive Federal Financial
tions in December 2005 with full federal
Participation under Medicaid.”7 At the same time,
matching funds. This would ensure that HCBS
states are required to contribute a portion of the
waiver participants have the supplies they need to
cost of Medicare coverage for dual eligibles accord-
give them a two-month head start into 2006 and
ing to a complex formula based on prior per
the transition to Medicare. Because this authori-
capita drug expenditures for dual eligibles (the
zation would involve Medicaid expenditures for a
“clawback”). The Congressional Budget Office
time frame that is outside Medicaid’s responsibil-
estimates that the new Medicare drug law will
ity (January 2006 forward), special rules are required
actually increase state Medicaid spending by $1.2
to ensure it is not considered to be fraudulent.
billion between FY2004 and FY2006, primarilydue to clawback payments.8 Without clawback
Allow Medicaid to share drug information
relief, “wrap around” Medicaid drug coverage
with the Medicare prescription drug plan
may be prohibitively expensive for states. as soon as auto-enrollment is finalized. This would allow case managers more time to Lengthen the period for auto-enrollment.
guide dual eligibles through the transition
Many states have pushed for auto-enrollment of
process and help beneficiaries secure prescription
dual eligibles into a Medicare prescription drug
plan so that enrollment will not be dependent
I m pac t of th e M e di care P re sc ri p ti on D ru g B e ne f it on H om e - and C om munity - Base d S e rvi c e s Waive r P rog ram s
on action by individual beneficiaries. The final
rules issued by the Centers for Medicare and
Kaiser Commission on Medicaid and the Uninsured,
Medicaid Services on January 21, 2005, do in
“Dual Eligibles: Medicaid’s Role in Filling Medicare’s
fact include auto-enrollment. Auto-enrollment is
Gaps,” The Henry J. Kaiser Family Foundation,
slated to begin in fall 2005, “as soon as eligible
Part D plans are known,”9 and “those who do
Kaiser Commission on Medicaid and the Uninsured,
not sign up for a drug plan by the middle of
“Dual Eligibles: Enrollment and Spending, by State,
December will be auto-enrolled by Medicare.”10
2002,” The Henry J. Kaiser Family Foundation,
2005, for a benefit scheduled to begin on
All states except Arizona operate 1915(c) waivers;
January 1, 2006, simply does not allow enough
time to ensure that all dual eligibles are enrolled
Martin Kitchener, Terence Ng, Nancy Miller, andCharlene Harrington, “Medicaid Home and
Moreover, for continued coverage of prescrip-
Community-Based Services: National Program
tion drugs, beneficiaries will have just a few
Trends,” Health Affairs 24 (Jan/Feb 2005): 206–212.
short weeks to (a) see an in-network Medicare
Jack Hoadley, “The Effect of Formularies and Other
physician to have prescriptions written by that
Cost Management Tools on Access to Medications: An
in-network provider, and (b) receive prior
Analysis of the MMA and Proposed Regulations.”
authorization from the Medicare prescription
The Henry J. Kaiser Family Foundation, September2004.
drug plan for those newly written prescriptions. Finalizing auto-enrollment at least 60 days prior
Centers for Medicare and Medicaid Services, “Final
to January 1, 2006, would provide a more rea-
Rules Implementing the New Medicare Law: A
sonable time period for beneficiaries to com-
New Prescription Drug Benefit for All MedicareBeneficiaries, Improvements to Medicare Health
Plans and Establishing Options for Retirees,”
Medicare Fact Sheet, January 21, 2005.
keeping very sick, frail, and disabled dual eligibles
Centers for Medicare and Medicaid Services,
in the community, out of nursing facilities. Many
“Principal Changes in New Medicare from Proposed
states have long waiting lists for these programs, as
Rules to Final Rules: New Rules Establish New
enrollment is limited per federal statute.Yet the lit-
Prescription Drug Benefit, Improvements toMedicare Health Plans and Options for Retirees,”
erature documents overwhelming evidence that
Medicare Fact Sheet, January 21, 2005.
beneficiaries and their caretakers are exceedingly
more satisfied with community-based care.
Congressional Budget Office, “A DetailedDescription of CBO’s Cost Estimate for the
Medicare Prescription Drug Benefit,” July 2004.
smooth transition for HCBS dual eligibles from
Medicaid to Medicare drug coverage are typical of
Centers for Medicare and Medicaid Services,
what other states will confront. The remedies sug-
“Overview of the Medicare Prescription DrugBenefit: MMA Title I Summary,” January 21, 2005.
gested here should receive careful consideration bypolicymakers. Otherwise, a turbulent transition
10 Centers for Medicare and Medicaid Services, “Final
stands to hurt most the very people the programs
Rules Implementing the New Medicare Law: ANew Prescription Drug Benefit for All Medicare
serve, compromise the ability of states to effectively
Beneficiaries, Improvements to Medicare Health
operate and finance HCBS programs, and tarnish
Plans and Establishing Options for Retirees,”
the future of public health insurance programs.
Medicare Fact Sheet, January 21, 2005.
Charles J. Milligan, Jr., J.D., M.P.H., is executive director of the Center for Health Program Develop-ment and Management at the University of Maryland, Baltimore County (UMBC). Formerly, he wasvice president of The Lewin Group and Medicaid director for the State of New Mexico. He holds alaw degree from Harvard Law School and a master of public health degree from the University ofCalifornia, Berkeley.
is a private foundation supporting independent research on health andsocial issues. The views presented here are those of the author and should not be attributed toThe Commonwealth Fund or its directors, officers, or staff.
Daily aspirin therapy: Understand the benefits and risks Is an aspirin a day the right thing for you? It's not as easy a decision as it sounds. Know the benefits and risks before considering daily aspirin therapy. Source: by Mayo Clinic Daily aspirin therapy may lower your risk of heart attack, but daily aspirin therapy isn't for You should a daily aspirin only if your doctor advises you
RAFEL NADAL SALAS- L’INDIÀ D’ESPORLES III. Alçament militar i Guerra Civil, 1936-39. L’arròs va a “grumallons” A mesura que arribàvem als darrers dies de la Segona República, l’ambient polític s’enterbolia. La Falange, que no havia aconseguit cap diputat a les darreres eleccions a les quaranta províncies on s’havia presentat, va augmentar la seva pressió social.
 APRIL 2005
APRIL 2005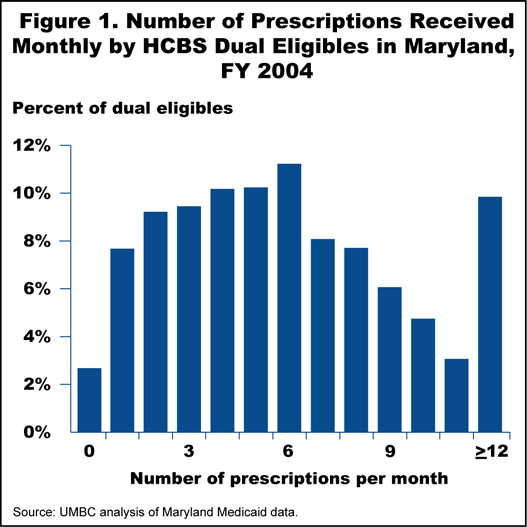
 a way to provide access to that drug during theappeal process or until which time the patient’sneeds can be reassessed by a Medicare-approvedphysician and alternative, formulary-approveddrugs can be prescribed? If not, community-baseddual eligibles whose drugs have not been approvedmay be at risk of medical complications and evenhospitalization or institutionalization.
a way to provide access to that drug during theappeal process or until which time the patient’sneeds can be reassessed by a Medicare-approvedphysician and alternative, formulary-approveddrugs can be prescribed? If not, community-baseddual eligibles whose drugs have not been approvedmay be at risk of medical complications and evenhospitalization or institutionalization. Charles J. Milligan, Jr., J.D., M.P.H., is executive director of the Center for Health Program Develop-ment and Management at the University of Maryland, Baltimore County (UMBC). Formerly, he wasvice president of The Lewin Group and Medicaid director for the State of New Mexico. He holds alaw degree from Harvard Law School and a master of public health degree from the University ofCalifornia, Berkeley.
Charles J. Milligan, Jr., J.D., M.P.H., is executive director of the Center for Health Program Develop-ment and Management at the University of Maryland, Baltimore County (UMBC). Formerly, he wasvice president of The Lewin Group and Medicaid director for the State of New Mexico. He holds alaw degree from Harvard Law School and a master of public health degree from the University ofCalifornia, Berkeley.