Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Microsoft word - hip 2013 11 15~submitted
1. Cover Page a) Preliminary study grant b) D-Cycloserine and virtual reality exposure therapy delivered on an iPad: Increasing access to treatment for social anxiety disorder c) Page Anderson, Ph.D., Associate Professor of Psychology and Neuroscience Chair and Director of Clinical Training, Clinical Psychology Georgia State University panderson@gsu.edu Barbara Rothbaum, Ph.D. Professor of Psychiatry and Behavioral Sciences Associate Vice Chair of Clinical Research Emory University School of Medicine brothba@emory.edu Kerry Ressler, MD, Ph.D., Professor of Psychiatry and Behavioral Sciences Emory University School of Medicine Co-Director, Trauma Clinic, Fulton County Behavioral Sciences Investigator, Howard Hughes Medical Institute kressle@emory.edu Josh Spitalnick, Ph.D., ABPP Director of Clinical Services Virtually Better Spitalnick@virtuallybetter.com e) $25,000 (direct cost). 2. Abstract: The proposed project aims to increase accessibility of exposure therapy, an evidence based treatment for social anxiety disorder, by adapting a therapist-assisted computer-based program to be delivered in a self-guided manner on an iPad. A significant problem with self-guided treatment delivered via computer is compliance. The vast majority of users do not complete treatment, so achieving therapeutic benefit as quickly as possible is essential. D-cycloserine is a drug found to augment response to therapist-guided exposure therapy for anxiety disorders, but has never been tested with self-guided exposure. This study uses a randomized, double-blind methodology to compare D-cycloserine (50 mg; DCS) to placebo in combination with self-guided virtual reality exposure therapy (VRE) delivered via iPad to treat social anxiety disorder. The proposed study tests the hypothesis that patients who receive DCS in combination with the self-guided VRE will show more improvement than those who receive placebo in combination with VRE. Outcome measures include self-reported symptoms of social anxiety, behavioral avoidance, and diagnostic remission. Participants (N=34) are adults with a primary diagnosis of social anxiety disorder. Participants will complete a structured diagnostic interview, standardized self-report measures of social anxiety, and a behavioral avoidance task (i.e., giving a speech) and will be assessed at pre-treatment, at post-treatment and at 3 month follow-up. Hierarchical linear regression and chi-square analyses will be used to test differences between those randomized to DCS versus placebo on the following outcomes: post-treatment scores of self-reported social phobia symptoms, willingness to and anxiety while giving a speech at post-treatment, and diagnostic remission at 3 month follow-up. The proposed project combines technological advances with translational research to develop an innovative and accessible treatment for those with social anxiety disorder. The pilot data generated from this study will be appealing to a variety of funding agencies, including the National Institute of Mental Health’s call for exploratory clinical trials of novel interventions for mental illnesses, the Patient-Centered Outcomes Research Institute’s call for effectiveness studies aimed to overcome barriers to treatment, and the National Science Foundation’s call for innovation-technology translation research. Background: Social Anxiety Disorder (social phobia) is the most common psychiatric disorder in the US. It negatively impacts health-related quality of life, educational and economic achievement, and it leads to attempted suicide in as many as 21% of affected individuals1,2. A critical barrier to progress in reducing the negative impact of this disorder is that 75-92% of sufferers do not receive treatment2. Social phobia self-help programs delivered via computer are designed to increase access to treatment and can be effective3. Compliance and completion rates of such programs are, however, quite poor4, greatly limiting their impact and accessibility. Furthermore, self-help programs for social phobia do not directly administer a critical component of treatment - exposure therapy. The direct administration of self-guided exposure therapy, using virtual reality is an innovation that would increase the accessibility and impact of computer delivered treatment. Exposure therapy is based on well-researched fear extinction learning paradigms, where individuals confront what they fear in a therapeutic manner and learn that the feared outcome will not occur5. Ressler et al’s groundbreaking translational research showed that D-cycolserine (DCS), an analogue of D-alanine and a partial agonist at the NMDA receptor, facilitates the process of fear extinction. DCS is different from other pharmacological agents used to treat social phobia which are prescribed chronically (daily) over a period of months or years to maintain a therapeutic dose; one pill of DCS is taken immediately before exposure therapy sessions. This work sparked a flurry of research showing that DCS augments exposure therapy for a variety of anxiety disorders; people who take DCS show benefit from therapist-assisted exposure therapy more quickly than those who take placebo6. Two randomized double-blind, placebo-controlled studies of social phobia conclude that the combination of DCS and therapist-assisted exposure therapy improves treatment response when participants complete fewer exposure sessions7,8. The ability of DCS to speed up the response to exposure therapy is especially valuable for sufferers using self-guided treatment, because they are not generally compliant with the full exposure protocol. The combination of DCS and self-guided exposure therapy would increase access to effective treatment. The use of DCS with self-guided exposure, however, has never been tested. Specific Aims
1. Adapt an existing computer program to deliver self-guided VRE for social phobia via iPad, and 2. Test the comparative efficacy of DCS vs placebo plus self-guided VRE.
Hypothesis: Participants who receive self-guided VRE plus DCS will show less self-reported social anxiety and less avoidance during a laboratory based behavioral test following a 5-week intervention than those who received self-guided VRE plus placebo. Innovation & Impact We seek to shift current clinical practice in the treatment of social phobia so that more people with the disorder receive exposure therapy. We will improve access to evidence-based treatment for social phobia with delivery of exposure via a computer – a modality that capitalizes on the fact that people with severe social phobia spend extensive hours on the computer9; exposure therapy can come to people with social phobia “where they are.” We also will be the first to test the delivery of exposure therapy on an iPad. We improve the approach of existing research on computer-delivered programs for social phobia by testing how treatment affects real behavior - existing research has relied exclusively on self-report measures and assessment of diagnostic status. No studies have assessed actual behavior – either in the lab or in the real-world. This study will improve scientific knowledge by answering the question of whether or not DCS augments self-guided exposure therapy. The combination of a self-help program with DCS addresses many of the obstacles to treatment with therapist- guided exposure therapy. For example, there are not enough mental health providers trained in exposure therapy. Furthermore, social anxiety disorder is characterized by the fear and avoidance of social situations, and psychotherapy is inherently a social encounter. The effective combination of DCS and self-guided virtual reality exposure is an avenue for treatment to any sufferer with access to a computer and a prescribing physician. When the proposed aims are achieved, an innovative treatment will exist that did not before – self- guided VRE delivered via computer. Preliminary Studies & Feasibility: The investigative team represents collaborators across academic institutions and disciplines, including a partnership with a State of Georgia incubated a small business. We are well positioned to complete the proposed project. Our team has extensive experience testing the use of virtual reality exposure for the treatment of social phobia, including in an open study (N=10) and a randomized clinical trial (N=75)10. We developed and tested a self-help program delivered via computer, with minimal therapist support11. The self-help program was tested in a small (N=10) uncontrolled trial of 8 sessions, and results showed decreases in scores on standardized self-report measures of social anxiety from pre- to post-treatment and follow-up. Large effect sizes were observed at post-treatment (d = 1.22-1.53) and follow-up (d = 1.41 - 2.39).
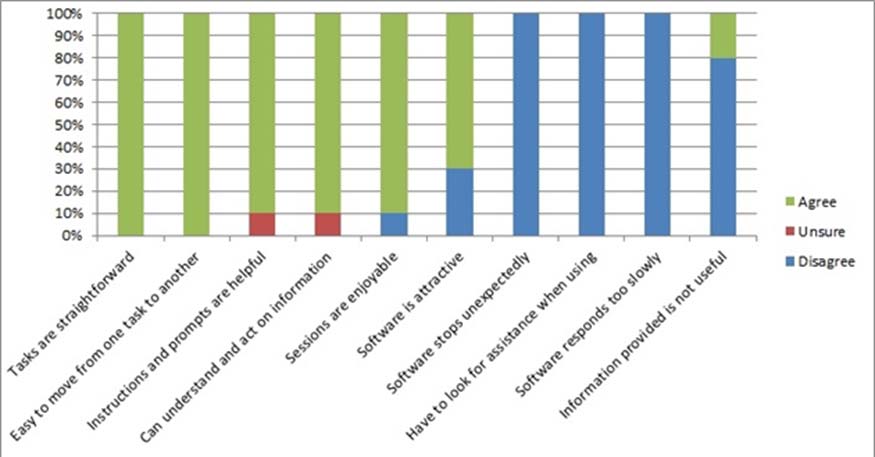
Using standardized measures of software usability, participants described the program as easy-to-use, including a participant who had never before used a computer11. Since this study, the program has been updated with new virtual environments, as well as shortening the treatment down. The proposed project will adapt an existing program for delivery via a tablet and to collect data via the computer.
Finally, the investigative team completed a double-blind, placebo controlled trial that tested the combination of DCS vs placebo combined with therapist-guided VRE for specific phobia12.
In summary, the team has worked together to develop and test VRE for social phobia, recruited and retained clinical samples of adults with social phobia and retained them through follow-up. They have also worked together to test the combination of DCS and VRE for people with anxiety disorders. Thus, the investigative team is well-positioned to complete the specific aims of adapting a computer program that delivers self-guided exposure therapy for social phobia via a tablet and testing following hypothesis: Participants who receive self- guided exposure therapy plus DCS will show less self-reported social anxiety and less avoidance during a laboratory based behavioral test following a 5-week intervention than those who received self-guided exposure therapy plus placebo. Methodology
The proposed research uses a randomized, double-blind, placebo-controlled, parallel-group methodology to compare two treatments: DCS and placebo in combination with self-guided VRE delivered on a computer. Participants: Participants will be 34 (17 per condition) adults meeting criteria for a DSM-V primary diagnosis of SAD that includes public speaking fears recruited from the community, using public service announcements, referrals from the community, and advertisements. Other inclusion/exclusion criteria include: Inclusion Criteria: Exclusion Criteria:
Understand and provide written informed consent prior to
Participation in clinical trial within the past 12 months
or treatment with DCS in a previous study
Be able to communicate in English with study personnel
History of mania, schizophrenia, or other psychoses
Be able to manipulate the computer interface to interact with
Any unstable medical condition; Seizure disorders,
with the exception of a childhood history of isolated, non-recurrent febrile seizures
If female, must have a negative pregnancy test prior to
Current or past substance (except nicotine, caffeine)
treatment and be maintained on an acceptable method of
or alcohol dependence based on DSM-V criteria
If using psychotropic medication, stable on medication and
Liebowitz Social Anxiety Scale (LSAS) score of < 50
Clinician Administered Measure: Structured Clinical Interview for the DSM-IV Axis I Disorders – Patient Edition (SCID I/P)13. The SCID will be administered to determine eligibility status and the diagnostic status of a variety of Axis I conditions falling within the mood, alcohol/substance use, and anxiety disorders modules. Twenty percent of administered SCIDs will be rated by an independent rater to establish inter-rater reliability.
Self-report Measures of Social Anxiety, Depression, Disability, Quality of Life, and Improvement:
The Liebowitz Social Anxiety Scale-self report version (LSAS-SR)14 is the primary outcome measure for the study. The LSAS-SR measures fear in and avoidance of 24 social situations, demonstrates good psychometric properties15,16. The Social Phobia Scale and Social Interaction Anxiety Scale17are secondary measures of social anxiety, assessing fears of being scrutinized during performance situations and the cognitive, affective, and behavioral reactions to social interactions, respectively. Depressive symptoms will be tracked using the Patient Health Questionnaire-9-item18. The Sheehan Disability Scale19 assesses functional impairment across work, social life, and family life, and the Quality of Life Inventory assesses the degree of satisfaction across important life domains. The Clinical Global Improvement Scale, Patient Report 20 is a face valid self-report global measure of improvement. All self-report measures show good psychometric properties when administered via the computer 21.
Behavioral Avoidance Tests (BAT):
Participants will complete two social interaction tasks. The Unstructured Conversation Task22 and an Impromptu Speech Task23. In each task, participants will rate their anxiety using a 9-point Likert scale (0= no distress to 8=extreme distress). The assessments will be video recorded and the amount of eye contact and time spent speaking by participants will be rated by research assistants who are blind to condition.
Interview / Double-blind Screening treatment period treatment Study Day
Demographics, Medical Hx, Inclusion/Exclusion
Administer study drug, assess adverse events
Treatment:Participants in both conditions will complete self-guided VRE11 administered completely by computer (with no clinician contact) for exposure. Treatment will consist of 5 weekly visits. The first visit will last 60 minutes and will be off study medication. The participant will be familiarized with computer, and the self- help program will introduce the basic treatment rationale, psychoeducation about social phobia and anxiety management techniques. Participants will be randomly assigned to treatment condition after the first session. The next four visits will be 30-minute exposure sessions, an “underdosing” of exposure therapy24. A predetermined fear hierarchy will be used such that participants will start with less threatening social situations (i.e., small setting with friendly people vs. a large bored audience) which will be controlled by the computer program. Participants will complete all treatment sessions alone on the computer in a laboratory room. They will be asked to complete only one session at a time during each visit and remain in the room for a standard length of time (30 minutes for each exposure session). Medication:Participants will be randomized in a double-blind fashion (using a computer-generated randomization code) to receive a single oral 50-mg dose of DCS or placebo 30 minutes prior to each exposure session (four total doses). This dosage and timing is based on previous studies utilizing DCS to enhance exposure therapy7,12,25. Study medications will be administered in the clinic supervised by study personnel to ensure compliance. DCS shows excellent central bioavailability, reaching peak cerebrospinal fluid levels within 1 to 2 hours, and is primarily excreted renally with a half-life of 10 hours. No significant adverse effects have been described in any of the recent clinical studies examining DCS for cognitive enhancement6. Data Analysis: To test the hypothesis that participants who receive DCS in combination with VRE will improve more than participants who receive placebo in combination with VRE, a hierarchical regression model will be used to compare post-treatment scores on the primary outcome measure (LSAS-SR) between groups. Pre- treatment scores will be entered in the first block as a covariate. A coded variable representing treatment group will be entered in the second block. A power analysis assuming power of .8 and a significance level of .05 and using estimated effect sizes from prior work comparing DCS to placebo6,12 and our own work with VRE11, yielded a recommended sample size of N=34 for these analyses.
Another primary outcome is willingness to complete the behavioral avoidance test at post-treatment,
which will be compared across treatment groups using Chi square analysis. Analysis of variance will be used to compare differences in anxiety ratings at post treatment and follow-up. Secondary analyses will examine the proportion of participants achieving remission, defined as LSAS total score 30 and the proportion of participants who no longer meet criteria for social anxiety disorder across groups at 3 month follow-up, as defined by the SCID.
Potential for External Funding The proposed project’s technological innovation and aim to improve accessibility of an effective treatment to an underserved population is in line with current missions of external funding institutions. Potential funding mechanisms include: the National Institute of Mental Health (NIMH)’s call for exploratory clinical trials of novel interventions for mental illnesses, http://grants.nih.gov/grants/guide/notice-files/NOT-MH-13-022.html and the Patient-Centered Outcomes Research Institute (PCORI)’s call for effectiveness studies aimed to overcome barriers to treatment, http://www.pcori.org/funding-opportunities/funding-announcements/addressing- disparities-spring-2014-cycle/ . The proposal’s partnership with a small business concern is relevant to the National Science Foundation (NSF)’s call for innovation-technology translation research, http://www.nsf.gov/pubs/2013/nsf13575/nsf13575.htm. Budget Justification: Equipment: $1200
IPads ($500) with protection plan ($100) for a total of $600/each. One tablet will be used for development and support purposes. Two tablets will be used for data collection – one of which will be purchased by Georgia State University as a cost sharing measure. One of these tablets will be raffled to a participant completing the follow-up.
50mg DCS or placebo, 4 doses per participant ($1050) and 20 urine pregnancy tests ($250)
Advertising in local media outlet for study participants ($1000) and participant payment ($1700), $50 for completion of treatment
To reimburse participants for study session visits ($5.00/pass)
To assume day-to-day responsibility for coordination of the study. Study assessments and treatment will be conducted by doctoral level clinical psychology graduate students within Dr. Anderson’s lab.
Matching/Cost sharing: Georgia State University: $6600
Georgia State University will pay $6000 in graduate student support for this study. These funds will be combined with the $1500 allocated in the proposed budget to ensure sufficient support for the day-to-day running of the study. Georgia State University will purchase the iPad with technical support to be used for the intervention (~600)
Virtually Better is matching $ 9,000 in development cost. The cost of adapting the software for use on a tablet is approximately $27,000; we have allocated 2/3 of the cost in the budget and VBI will cost share the rest.
References 1. Schneier FR, Heckelman LR, Garfinkel R, Campeas R, others. Functional impairment in social phobia. Journal of Clinical Psychiatry. 1994. 2. Schneier FR, Johnson J, Hornig CD, Liebowitz MR, Weissman MM. Social phobia: comorbidity and morbidity in an epidemiologic sample. Archives of General Psychiatry. 1992;49(4):282. 3. Andrews G, Cuijpers P, Craske MG, McEvoy P, Titov N. Computer Therapy for the Anxiety and Depressive Disorders Is Effective, Acceptable and Practical Health Care: A Meta-Analysis. PLoS ONE. 2010;5(10):e13196. 4. Christensen H, Griffiths KM, Jorm AF. Delivering interventions for depression by using the internet: randomised controlled trial. BMJ. 2004;328(7434):265. 5. Kroenke K, Spitzer RL, Williams JB., Monahan PO, L\öwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Annals of Internal Medicine. 2007;146(5):317. 6. Hofmann SG, Sawyer AT, Asnaani A. D-cycloserine as an augmentation strategy for cognitive behavioral therapy for anxiety disorders: an update. Curr. Pharm. Des. 2012;18(35):5659–5662. 7. Hofmann SG, Meuret AE, Smits JA., et al. Augmentation of exposure therapy with D-cycloserine for social anxiety disorder. Archives of general psychiatry. 2006;63(3):298. 8. Guastella AJ, Richardson R, Lovibond PF, et al. A randomized controlled trial of D-cycloserine enhancement of exposure therapy for social anxiety disorder. Biological psychiatry. 2008;63(6):544–549. 9. Caplan SE. Relations among loneliness, social anxiety, and problematic Internet use. Cyberpsychol Behav. 2007;10(2):234–242. 10. Anderson PL, Price M, Edwards SM, et al. Virtual reality exposure therapy for social anxiety disorder: A randomized controlled trial. Journal of consulting and clinical psychology. 2013;81(5):751. 11. Anderson P, Zimand E, Schmertz SK, Ferrer M. Usability and utility of a computerized cognitive-behavioral self-help program for public speaking anxiety. Cognitive and Behavioral Practice. 2007;14(2):198–207. 12. Ressler KJ, Rothbaum BO, Tannenbaum L, et al. Cognitive enhancers as adjuncts to psychotherapy: use of D-cycloserine in phobic individuals to facilitate extinction of fear. Archives of General Psychiatry. 2004;61(11):1136. 13. First M, Spitzer R, Gibbon M, Williams J. Structured clinical interview for DSM-IV axis I disorders: research version: Non-patient edition (SCID-I/NP). Structured clinical interview for DSM-IV axis I disorders: research version: Non-patient edition (SCID-I/NP). 2002. 14. Liebowitz MR. Social phobia. Modern problems of pharmacopsychiatry. 1987. Available at: http://doi.apa.org/psycinfo/1988-23625-001. Accessed November 14, 2013. 15. Heimberg RG, Horner KJ, Juster HR, et al. Psychometric properties of the Liebowitz social anxiety scale. Psychological Medicine. 1999;29(1):199–212. 16. Safren SA, Heimberg RG, Horner KJ, et al. Factor structure of social fears: the Liebowitz Social Anxiety Scale. Journal of Anxiety Disorders. 1999;13(3):253–270. 17. Mattick RP, Clarke JC. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behav Res Ther. 1998;36(4):455–470. 18. Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282(18):1737–1744. 19. Sheehan DV. The anxiety disease. Scribner New York; 1983. Available at: http://www.getcited.org/pub/102295405. Accessed November 14, 2013. 20. Kadouri A, Corruble E, Falissard B. The improved Clinical Global Impression Scale (iCGI): development and validation in depression. BMC Psychiatry. 2007;7:7. 21. Hirai M, Vernon LL, Clum GA, Skidmore ST. Psychometric Properties and Administration Measurement Invariance of Social Phobia Symptom Measures: Paper-Pencil vs. Internet Administrations. Journal of Psychopathology and Behavioral Assessment. 2011;33(4):470–479. 22. Turner SM, Beidel DC, Cooley MR, Woody SR, Messer SC. A multicomponent behavioral treatment for social phobia: Social effectiveness therapy. Behaviour Research and Therapy. 1994;32(4):381–390. 23. Beidel DC, Turner SM, Jacob RG, Cooley MR. Assessment of social phobia: Reliability of an impromptu speech task. Journal of Anxiety Disorders. 1989;3(3):149–158. 24. Deveney CM, McHugh RK, Tolin DF, Pollack MH, Otto MW. Combining D-cycloserine and exposure-based CBT for the anxiety disorders. Clin Neuropsychiatry. 2009;6(2):75–82. 25. Hofmann SG. Enhancing exposure-based therapy from a translational research perspective. Behaviour research and therapy. 2007;45(9):1987–2001.
Curriculum dell’attività scientifica e didattica Federica Fabrizzi Formazione agosto 2010: vincitrice di concorso a Ricercatore a tempo indeterminato nel settore disciplinare IUS 09 (Istituzioni di diritto pubblico) presso la facoltà di giurisprudenza dell’Università Telematica Internazionale Uninettuno; da novembre 2007: dottoranda di ricerca in Teoria dello Stato e
ANAESTHESIA AND ANALGESIA: CONTRIBUTION TO SURGERY,Department of Anaesthesia, Christchurch School of Medicine, University of Otago, Christchurch, New ZealandAnaesthetists provide comprehensive perioperative medical care to patients undergoing surgical and diagnostic procedures, includingpostoperative intensive care when needed. They are involved in the management of perioperative acute pain as w
 Hypothesis: Participants who receive self-guided VRE plus DCS will show less self-reported social anxiety
Hypothesis: Participants who receive self-guided VRE plus DCS will show less self-reported social anxiety  Interview /
Interview /