Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
406_206_article_680-web 1.4
Eur Arch Psychiatry Clin Neurosci (2006) xx:1–4
Gabriele Ende Æ Traute Demirakca Æ Sigrid Walter Æ Tim Wokrina Æ Alexander SartoriusDirk Wildgruber Æ Fritz A. Henn
Subcortical and medial temporal MR-detectable metaboliteabnormalities in unipolar major depression
Received: 3 January 2006 / Accepted: 27 June 2006 / Published online: 16 August 2006
determine whether MR-detectable alterations of cho-line-containing compounds in two key neural systems
Mood-congruent processing biases are amongst the
involved in major depression disorder namely the
most robust research findings in neuropsychological
hippocampus and the basal ganglia can be detected.
studies of major depressive disorder (MDD). Func-
Multislice proton magnetic resonance spectroscopic
tional MR studies could demonstrate increased and
imaging was applied in 11 patients with major
decreased activity in depressed patients compared
depressive disorder (MDD) and ten matched healthy
to healthy controls as a response to emotional stim-
subjects. Voxels were selected from the left and right
side of the hippocampus and the putamen. Signifi-
The hippocampus is the focus for hypotheses
cantly lower choline-containing compounds in the
related to stress and its effects. A reduced hippo-
hippocampus and significantly higher choline-con-
campal serotonergic neurotransmission and im-
taining compounds in the putamen of patients with
paired neurogenesis and synaptogenesis in this
MDD compared to healthy subjects were found. No
brain region have been reported for MDD [
significant differences were found for the other
]. We previously observed a decreased signal
metabolites in the two regions evaluated. Abnormal
of MR-detectable hippocampal choline-containing
levels of choline-containing compounds most likely
compounds in patients with medication refractory
reflect altered membrane phospholipid metabolism.
A reduced level in the hippocampus and an increased
The basal ganglia are a complex of deep nuclei
level in the putamen suggest regionally opponent
that consist of the corpus striatum, globus pallidus,
and substantia nigra. The corpus striatum, whichincludes the caudate nucleus and the putamen, re-
ceives input from the cerebral cortex and the thal-
containing compounds Æ MR spectroscopic imaging Æ
amus and, in turn, projects to the globus pallidus.
The basal ganglia are not only involved in motorfunctions but also have important cognitive, ocu-lomotor, and limbic processing functions. They
Presented in part at the 13th annual meeting of the Society of
form a part of the brain neuroanatomic circuits that
Magnetic Resonance in Medicine, Miami 2005.
may be involved in mood regulation and have been
PD Dr. G. Ende (&) Æ T. Demirakca Æ S. Walter Æ T. Wokrina
increasingly implicated in the pathophysiology of
MRI and PET studies found the hippocampi and
Central Institute of Mental HealthJ5, 68159 Mannheim, Germany
the basal ganglia morphologically and functionally
altered in MDD compared to healthy subjects. For a
review see Ende et al. []. In three previous MRS/
MRSI studies of the basal ganglia in MDD contro- EA
versial results have been reported regarding the ratio PCN
Department of Psychiatry and Psychotherapy
of Cho to total creatine (tCr). While Renshaw et al.
] in a single voxel study and a fairly large patient
Table 1 Summary of patient and control characteristics, mean MRSI
metabolite values and standard deviations for the hippocampus and putamen
hippocampus basal ganglia
b Beck Depression Inventory at time of MRSI scan
c Hamilton Depression Score (21 items) at time of admission
group (n = 42) reported decreased Cho/tCr, Vythi-lingam et al. ] in a recent MRSI study of 17 MDDpatients and an early single voxel study by Charleset al. [reported increased Cho/tCr in a group of7 MDD patients compared to controls.
Our proton MRSI study aimed to corroborate
reported alterations in MR-detectable choline-con-taining compounds in depressed patients compared
Fig. 1 The location of the MRSI slices and the typical voxel position for the
to healthy controls in these two neural key regions of
evaluated subregions: (a) hippocampi and (b) putamen
MDD. We hypothesized that Cho would be founddecreased in the hippocampus in MDD patients,
whereas basal ganglia Cho would show an oppositealteration in comparison to healthy controls.
All MRSI studies were performed on a 1.5 T Siemens Vision system
With the long echo multislice MR spectroscopic
using a standard CP head coil (Magnetom VISION, Siemens,Erlangen, Germany). Three MRSI slices were acquired within one
imaging method used, spectra with non-overlapping
measurement. A selective lipid inversion pulse, TR = 1,500 ms,
resonances of for N-acetylasparte (NAA), a marker
TE = 135 ms, FOV = 300 mm, grid = 36 · 36, Slice thickness =
of neuronal function, choline-containing compounds
15 mm, nominal voxel size = 1.04 cm3 (0.8 · 0.8 · 1.5 cm) were
(Cho), possibly involved in membrane and myelin
used. In addition, a 3D magnetization prepared rapid gradient echo(MPRAGE) data set was acquired.
sheath metabolism and creatine- and phosphocrea-tine (tCr) reflecting cerebral energy metabolism
Postprocessing of the MRSI data included CSF correction of MRSIbrain data to increase sensitivity and decrease variance [
Voxels were selected from the left and right hippocampus and
left and right putamen. In addition to the metabolite signals thevoxel composition for each subregion was evaluated for differences
in GM, WM and CSF content. Per data set mean values of spectrafrom each subregion are reported.
Eleven inpatients diagnosed for MDD and ten healthy comparison
Absolute integral values for NAA, tCr, and Cho were evaluated
subjects were studied with 1H MRSI. All patients satisfied DSM IV
[, ]. In a first analysis all spectra indicated in Fig. were curve
criteria for MDD and were inpatients of the Department of Psy-
fitted. The operator was blinded to the subject’s status (patient or
chiatry and Psychotherapy at the time of the examination. All
control) but not to the research question. The operator chose
patients were on antidepressive medication and no restrictions
spectra by anatomical location, at this step blinded to spectral
were made regarding antidepressive co-medication like lorazepam.
appearance. Spectra were then filtered for further evaluation by
A summary of patient and control characteristics is given in the
objective quality criteria In a next step these criteria were
applied in an automated exclusion routine: linewidth had to be less
After complete description of the study to the subjects, written
than 10 Hz, voxel CSF content had to be less than 25%, for hip-
informed consent was obtained. The study was approved by the
pocampal voxels GM voxel content had to be higher than WM
Cho hippocampi Cho putamen GM voxel content hippocampi GM voxel content putamen
Fig. 2 Scatter plots of the Cho signal in patients (gray circles) and healthy controls (black circles) as a function of voxel GM content
A voxel-based-morphometry (VBM) analysis was performed
correlation analyses revealed a significant negative
with SPM2 using the 3D mprage data sets in order to detect mor-
correlation between hippocampal GM and the Cho
phometrical changes in those brain areas where metabolic changeswere hypothesized.
signal in the patient group (R = )0.81, P = 0.02).
In concordance with our previous results we could
corroborate a decreased Cho value in the hippocam-pus of patients with major depression (F = 5.73,
Hypothesis driven univariate as well as multivariate analyses based
on a general linear model were used for data analysis by the use of
In the spectra from the putamen we see a signifi-
SPSS for windows release 12.0. For the univariate analyses thedependent variable was the concentration estimates for Cho in
cant above normal Cho value in the patients com-
the two subregions (hippocampus, putamen) with group as the
pared to controls (F = 5.66, df = 1, 10, P = 0.039).
between-subject factor and with age and voxel GM content as
Statistics on the remaining metabolite signal values in
co-variates. Additionally, according multivariate analyses were
these two regions were above the P = 0.05 level (tCr,
conducted with the remaining metabolite measures (NAA, tCr) as
hippocampus: F = 3.10, df = 1, 12, P = 0.1; tCr, pu-
dependent variables. We used a paired t-test to determine intra-individual left–right metabolite differences. Correlations were
tamen: F = 3.11, df = 1, 10, P = 0.11; NAA, hippo-
assessed with the Spearman’s test. The criterion of significance level
campus: F = 1.35, df = 1, 12, P = 0.27 and NAA,
putamen: F = 2.73, df = 1, 10, P = 0.13). Meanmetabolite values, GM and CSF voxel contents are
VBM analysis did not reveal any significant dif-
ferences in neither hippocampal nor striatal volumina
The quality criteria based on spectral resolution
(spectral linewidth and voxel CSF content) were not
Due to the small sample size a co-analysis of
met by all spectra from all subjects. Therefore, the
medication effects (e.g. dosage or medication type)
group sizes for each evaluated region are less than the
total group of acquired data sets (see Table Wecould not detect a significant left–right hemispheredifference, neither for the hippocampi nor the putamen
in both groups (paired t-test P > 0.16, t < 1.5). GM,WM and CSF voxel contents were not significantly
The hippocampus is the focus for hypotheses related
different between patients and controls. A Spearman
to stress and its effects. A reduced hippocampal Cho
signal is in good accordance to reduced serotonergicneurotransmission and impaired neurogenesis/syna-
ptogenesis in this brain region, respectively [We
1. Charles HC, Lazeyras F, Krishnan KR, Boyko OB, Payne M,
previously observed a decreased Cho signal in the
Moore D (1994) Brain choline in depression: in vivo detection
hippocampus in MDD patients []. Additionally, two
of potential pharmacodynamic effects of antidepressant ther-apy using hydrogen localized spectroscopy. Prog Neuropsy-
previous MRSI studies of the basal ganglia in major
chopharmacol Biol Psychiatry 18:1121–1127
depression reported increased Cho/tCr in the puta-
2. Davidson RJ, Irwin W, Anderle MJ, Kalin NH (2003) The neural
men. This is in concordance with our finding of
substrates of affective processing in depressed patients treated
an increased striatal Cho signal with the tCr signal
with venlafaxine. Am J Psychiatry 160:64–75
3. Drevets WC (2000) Neuroimaging studies of mood disorders.
Patients of our earlier study were medication
4. Duman RS (2004) Depression: a case of neuronal life and death?
resistant and more severely ill. Their hippocampal
Cho levels increased to normal levels with electro-
5. Ende G, Braus DF, Walter S, Weber-Fahr W, Henn FA (2000)
convulsive therapy. Normal choline levels were also
The hippocampus in patients treated with electroconvulsivetherapy: a proton magnetic resonance spectroscopic imaging
observed in remitted patients treated with amitrip-
tyline Cho decreased again in our 12-month
6. Ende G, Braus DF, Walter S, Weber-Fahr W, Henn FA (2003)
follow-up study without patients necessarily relaps-
Multiregional 1H-MRSI of the hippocampus, thalamus, and basal
ganglia in schizophrenia. Eur Arch Psychiatry Clin Neurosci253:9–15
Structural or functional abnormalities of the
7. Ende G, Demirakca T, Tost H (2006) The biochemistry of dys-
limbic-cortical-striatal-pallidal-thalamic
functional emotions: proton MR spectroscopic findings in major
circuit have been reported and are associated with
depressive disorder. Progr Brain Res Volume 156, Chapter 27
an increased risk for major depression [Smaller
8. Henn F, Vollmayr B, Sartorius A (2004) Mechanisms of
hippocampal, caudate and putamen volumes have
depression: the role of neurogenesis. Drug Discov Today DisMech 1:407–411
been reported in several MRI studies of major
9. Henn FA, Vollmayr B (2004) Neurogenesis and depression:
depression []. Functional investigations stated uni-
etiology or epiphenomenon? Biol Psychiatry 56:146–150
directional alterations in striato-limbic areas. The
10. Husain MM, McDonald WM, Doraiswamy PM, Figiel GS, Na C,
Danish/PET depression project observed an in-
Escalona PR, Boyko OB, Nemeroff CB, Krishnan KR (1991) Amagnetic resonance imaging study of putamen nuclei in major
creased CBF (right sided) in MDD patients in hip-
pocampal and striatal regions []. Presentation of
11. Obergriesser T, Ende G, Braus DF, Henn FA (2001) Hippo-
sad and happy facial expressions showed fMRI
campal 1H-MRSI in ecstasy users. Eur Arch Psychiatry Clin
alterations of the same sign in parahippocampal and
12. Obergriesser T, Ende G, Braus DF, Henn FA (2003) Long-term
putaminal regions. A differential pattern of neural
follow-up of magnetic resonance-detectable choline signal
response toward sad versus happy facial expressions
changes in the hippocampus of patients treated with electro-
in MDD was observed by Surguladze et al. [
convulsive therapy. J Clin Psychiatry 64:775–780
These results do not necessarily contradict MRSI
13. Renshaw PF, Lafer B, Babb SM, Fava M, Stoll AL, Christensen
findings of regionally opposed cholinergic changes.
JD, Moore CM, Yurgelun-Todd DA, Bonello CM, Pillay SS,Rothschild AJ, Nierenberg AA, Rosenbaum JF, Cohen BM
It can be speculated, that deficits in hippocampal
(1997) Basal ganglia choline levels in depression and response
synaptogenesis as predicted by the neurotrophin
to fluoxetine treatment: an in vivo proton magnetic resonance
hypothesis lead to compensatory functional altera-
spectroscopy study. Biol Psychiatry 41:837–843
tions in other regions within the LCSPT circuit.
14. Sapolsky RM (2004) Is impaired neurogenesis relevant to the
affective symptoms of depression. Biol Psychiatry 56:137–139
Striatal synaptic and/or membrane alterations (here:
15. Surguladze S, Brammer MJ, Keedwell P, Giampietro V, Young AW,
possibly an increased membrane turnover) are then
Travis MJ, Williams SC, Phillips ML (2005) A differential pattern of
neural response toward sad versus happy facial expressions inmajor depressive disorder. Biol Psychiatry 57:201–209
16. Videbech P, Ravnkilde B, Pedersen TH, Hartvig H, Egander A,
Clemmensen K, Rasmussen NA, Andersen F, Gjedde A,
Rosenberg R (2002) The Danish PET/depression project: clin-ical symptoms and cerebral blood flow. A regions-of-interestanalysis. Acta Psychiatr Scand 106:35–44
Overall, abnormal Cho signals most likely reflect al-
17. Vythilingam M, Charles HC, Tupler LA, Blitchington T, Kelly L,
tered membrane phospholipid metabolism. A reduced
Krishnan KR (2003) Focal and lateralized subcortical abnor-
level in the hippocampus and an increased level in the
malities in unipolar major depressive disorder: an automated
putamen suggest regionally opponent membrane
multivoxel proton magnetic resonance spectroscopy study. BiolPsychiatry 54:744–750
18. Weber-Fahr W, Ende G, Braus DF, Bachert P, Soher BJ, Henn
FA, Buchel C (2002) A fully automated method for tissue seg-mentation and CSF-correction of proton MRSI metabolites
We thank Dr. Norbert Schuff for providing
corroborates abnormal hippocampal NAA in schizophrenia.
the multislice spherical k-space sampling MRSI sequence and
Drs. Andrew Maudsley and Brian Soher (NIH/NIA Grant #
19. Wokrina T, Ende G (2004) Quality maps facilitate MRSI eval-
R01AG12119) for providing the automated spectral fitting routine.
uation with automated spectral analysis. Proceedings of the
This study was supported by a grant from the Heidelberg Academy
European Society for Magnetic Resonance in Medicine and
IMPORTANT SAFETY INFORMATION ABOUT SPRIX® (ketorolac tromethamine) Nasal Spray WARNING: LIMITATIONS OF USE, GASTROINTESTINAL, BLEEDING, CARDIOVASCULAR, and RENAL RISK Limitations of Use – The total duration of use of SPRIX® and other ketorolac formulations should not exceed 5 days Gastrointestinal (GI) Risk – Ketorolac can cause peptic ulcers, GI bleeding, and/or perforation of the sto
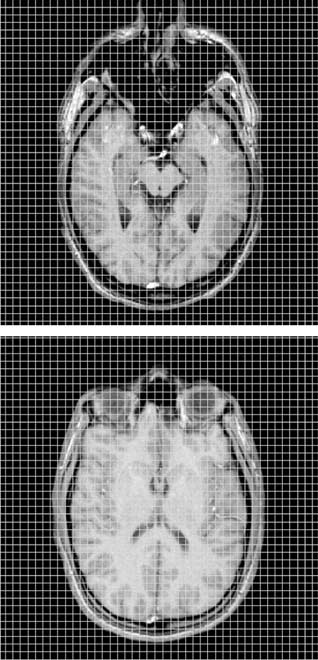 Table 1 Summary of patient and control characteristics, mean MRSI
metabolite values and standard deviations for the hippocampus and putamen
hippocampus
Table 1 Summary of patient and control characteristics, mean MRSI
metabolite values and standard deviations for the hippocampus and putamen
hippocampus