Tadalafil zeigt eine ausgeprГӨgte Proteinbindung von Гјber 90 %, was eine gleichmГӨssige Verteilung im Gewebe ermГ¶glicht. Das Verteilungsvolumen betrГӨgt rund 63 Liter, was auf eine deutliche extravaskulГӨre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau Гјber CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische AktivitГӨt mehr besitzen. Die Exkretion erfolgt Гјberwiegend fГӨkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche BioverfГјgbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen fГјhren cialis generikum schweiz regelmГӨssig als Beispiel fГјr PDE5-Hemmer mit verlГӨngerter Halbwertszeit auf.
Lepra.org.uk
Death caused by strongyloides hyperinfection in aleprosy patient on treatment for a type II leprosyreactionB U N S E L E A N G * , LU T L Y N E N * * , R U T H T O O T I L L * ,S T E P H E N G R I F F I T H SГҫ & DI D IE R MO NCH YГҫ Гҫ
*Sihanouk Hospital Center of HOPE (SHCH), Street 134, Sangkat
Veal Vong, Khan 7 Makara, PO Box 2318, Phnom Penh 3, Cambodia
**Institute of Tropical Medicine (ITM) Antwerp, Belgium
Гҫ Kean Khleang National Rehabilitation Center, Phnom Penh,CambodiaГҫ Гҫ Institut Pasteur du Cambodge, Phnom Penh, Cambodia
Strongyloides stercoralis is present worldwide and can cause
hyperinfection in patients on long-term immunosuppressive doses of steroids, as issometimes the case for patients treated for leprosy reactions. Strongyloideshyperinfection can present with ileus, as is discussed in this case report. Physicians,including surgeons, should be aware of this entity in order to avoid an unnecessarylaparotomy. Though patients may survive if diagnosed at an early stage,strongyloides hyperinfection syndrome has a mortality rate of 87% and preventionis therefore of utmost importance.
Strongyloides stercoralis is a worldwide intestinal nematode. It infects 30 million people in70 countries.Prevalence of S. stercoralis in Argentina is 83%, Nigeria 25%, Brazil 13%,Guinea 6В·4%, and for South-Esat Asia: Laos 19% and Thailand 11В·2%, No reports areavailable from Cambodia.
In immunocompetent patients, S. stercoralis infection usually results in asymptomatic
chronic disease of the gut, which can remain undetected for decades (up to 50 years).However, exacerbation of a chronic asymptomatic infection into Strongyloides hyperinfec-tion (SH) syndrome is commonly reported in immunocompromised hosts resulting fromcorticosteroid treatment, chemotherapy for cancer, organ transplant recipients, autoimmunediseases, malnutrition, and rarely in HIV/AIDS. In a case-control study steroids users have3В·3 times more risk of developing strongyl
Correspondence to: B. Leang (Tel: +855 23 882 484 or +855 11 850 471; Fax: +855 23 882 485;
Strongyloides hyperinfection in a leprosy patient
In immunocompromised states autoreinfection is greatly increased, resulting in a marked
increase in the intestinal worm burden and in massive dissemination of autoinfective filariformlarvae (FL) to the lungs and other tissues (skin, meninges, liver, biliary tract, spleen). Thisleads to the SH syndrome, with disseminated bacterial infection, resulting from leakage of gutflora on the surfaces of migrating larvae. SH results in a high mortality rate, up to 87%.
We report a fatal case of SH resulting from long-term steroid use, presenting with ileus.
A 19-year-old male student presented to the emergency room of our hospital in May 2002with abdominal distension and absence of stool and gas for 1 day. The history revealed thatthe patient had a type II leprosy reaction, for which he was put on prednisolone 50 mg POdaily with thalidomide in December 2001. After 4 weeks of therapy, the prednisolone wastapered slowly. In early February, the patient had been given benzyl benzoate for possiblescabies. In March (prednisolone was at 20 mg daily), he developed a papular skin rash andprednisolone was increased again to 40 mg daily. One month later, widespread exfoliativeskin lesions appeared. By mid-April, the patient had diarrhoea, for which pyrantel,metronidazole and cotrimoxazole were given. One week later, a peripheral blood countshowed an eosinophilia of 12%.
On May 9, he again had diarrhoea and productive cough. Stool microscopy was requested
but results are not available. One day later, the patient had abdominal distension, vomiting, nostool and gas. A diagnosis of ileus was made and he was referred to a public referral hospitalin Phnom Penh. An upper endoscopy and laboratory tests showed non-specific findings,except for the presence of several polyps in the duodenum which were biopsied. After theprocedure, his ileus improved and he was sent back to the health centre. Two days later, theileus recurred. The patientвҖҷs mother asked for him to go home, but the attending physicianadvised and assisted in bringing the patient to a private NGO-funded hospital (SHCH).
On arrival at this hospital, the patient was uncomfortable, agitated and tachypnoeic. His
vital signs were: blood pressure 100/80 mmHg, heart rate 110 per minute, respiratory rate 28per minute and temperature 388C. He had cushingoid facies, mild pallor, but no jaundice orneck stiffness. Heart and lungs were normal. The skin overlying the distended abdomenshowed striae, no rebound tenderness, no hepatosplenomegaly and no mass, but poorperistalsis and tympanic percussion were found. Second degree (40 ВЈ 50 mm) pressurebedsores were present on both hips. The lower limbs showed oedema 2+ up to the level of theknees. Rectal examination was mildly tender. Yellow muddy stool was present in the rectum,and a stool sample was sent to the laboratory.
Laboratory results showed a marked hypokalaemia of 1В·9 meq/l (normal range:
3В·5 вҖ“ 5В·0 meq/l) and the stool examination showed many S. stercoralis larvae. Gastric fluidand the exudates of skin lesions sent for direct smear and Gram stain did not showS. stercoralis. A supine abdominal X-ray showed distended bowels filled with air. A chestX-ray was unremarkable.
The reviewing surgeon diagnosed the boy as having ileus secondary to an abdominal
infection, and no immediate surgical intervention was indicated. The patient was put onintravenous fluid with KCl, IV ceftriaxone, IV metronidazole and oral albendazole. Six hoursafter admission, the patient developed respiratory distress and hypotension. Ciprofloxacin IVwas added and his septic shock was treated with IV fluids and dopamine infusion. Despiteaggressive management, the patient died 24 h after admission.
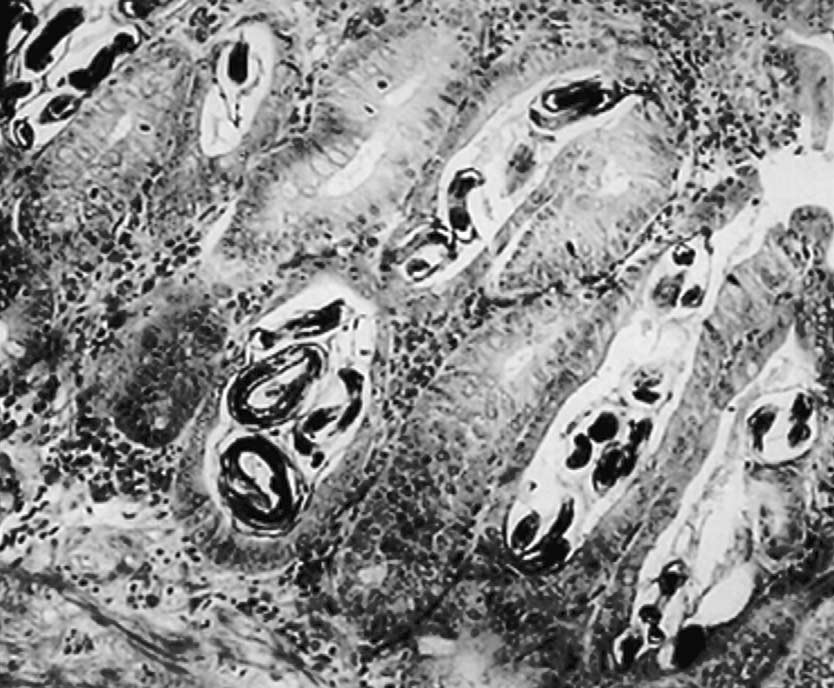
The results of histopathology of the duodenal biopsies performed at the other hospital
arrived after the patientвҖҷs death, and showed massive amounts of S. stercoralis larvae in themucosa (see
The course of this patientвҖҷs illness with diarrhoea, cough, peripheral eosinophilia, ileus,sepsis and the presence of many strongyloides stercoralis larvae in the stool and in theduodenal mucosa are strongly suggestive of strongyloides hyperinfection.
The patient died of presumed septic shock and acute respiratory distress syndrome. The
patient was too sick to cough up sputum for S. stercoralis larvae detection. The micro-organisms responsible for his sepsis were probably of gut origin. No blood culture was done,but we gave broad-spectrum antibiotics to empirically cover Gram negatives and anaerobes. His hypokalaemia probably resulted from continuing gastric aspiration, poor intake andchronic diarrhoea.
The diagnosis of strongyloidiasis is often delayed and overlooked because of non-specific
symptoms.A study from southern Taiwan reported diarrhoea (74%), fever (70%),abdominal pain (59%), cough (37%), dyspnoea (33%), constipation (26%), leukocytosis(81%), anaemia (67%) and eosinophilia (44%Although non-specific and not a constantfeature, peripheral blood eosinophilia $ 5% is often associated with strongyloidiasis,especially in immunocompetent hostThus, physicians in endemic regions shouldinclude strongyloidiasis in the differential diagnosis when patients present withgastrointestinal and/or pulmonary symptoms with peripheral eosinophilia.
Figure 1. Strongyloides stercoralis filariform larvae in duodenal biopsy. Giemsa stain ВЈ 50.
Strongyloides hyperinfection in a leprosy patient
Besides intestinal and pulmonary symptoms, larva currens skin lesions (rapidly
progressing linear, serpiginous, urticarial streaks) are rare, but are the pathognomoniccutaneous manifestation of strongylSH can present with ileus and may lead to anunnecessary laparotom
Stool microscopy to identify S. stercoralis larvae or ova has variable sensitivity.A direct
stool microscopy has only a sensitivity of 30% and three specimens will increase the sensitivityto 60 вҖ“ 70%.Stool concentration increases the sensitivity of stool microscopy up to 80%.S. stercoralis larvae or ova can also be detected in duodenal aspiration and embedded in theduodenal mucosa. S. stercoralis larvae can also be detected in sputum or bronchial washings. Other tests, available only at specialized centres, such as an ELISA test (IgE to S. stercoralisantigen) and agar plate culture have respectively 80 вҖ“ and 96%sensitivity.
Strongyloidiasis is a difficult infection to treat because of its autoinfective FL. Any truly
effective anthelmintic must kill every autoinfective FL in order to remove the danger ofpotentially serious disease. This becomes even harder in cases with ileus due to poorabsorption of the drug.
Albendazole is a well tolerated and safe treatment for strongyloidiasis. Pancytopenia and
agranulocytosis are two very rare side effects. For strongyloidiasis, a dose of 400 mg orallytwice daily for 5 days has a cure rate of 95There is little data on how to use albendazolefor SH. Ivermectin is registered as the drug of choice for the treatment of strongyloidiasis inthe WHOвҖҷs list of essential drugs.The recommended dose is 200 mcg/kg/day taken as asingle dose.In SH, this single dose should be repeated on day 2, day 15 and day 16.Because of its prohibitively high price, ivermectin is virtually unavailable in developingcountries, except for veterinary use and in onchocercosis control programs.
The success of SH therapy is largely dependent on early recognition and prompt
treatment. SH should be suspected when a patient on long-term immunosuppressive drugs(steroids) presents with severe gastrointestinal and respiratory tract symptoms, together withthe presence of S. stercoralis larvae or ova in stool or duodenal fluid or sputum, with orwithout skin rash/ulcerations, sepsis, Gram-negative bactaeremia or central nervous systeminvolvement.SH should be treated aggressively with anti-parasitic drugs and antibioticsthat target Gram negative bacteria (ceftazidime, ceftriaxone, ciprofloxacin, gentamycin). If peritonitis is suspected metronidazole should be added. Be aware of the possibility offungal co-infection. If ivermectin is not available, start albendazole 400 mg PO twice dailyand continue until at least three negative stool samples. An important therapeutic measure isto reduce the dose of steroids as low as possible.
In case of ileus due to SH where no response to an oral agent is apparent (due to poor
absorption), there are reports of successful treatment by thiabendazole per rectumandsubcutaneous use of a veterinary preparation of ivermectin.
Strongyloides hyperinfection is rarely reported in leprosy literature, but it may be under
reported as the diagnosis could be missed like in this case report. A PubMed search usingleprosy, strongyloides, strongyloidiasis, strongyloides hyperinfection as keywords found onefatal case report back in Based on current epidemiological surveys of S. stercoralisprevalence in neighbouring countries (Thailand 11В·2%, Laos 19%) and the burden of HIV/AIDS in Cambodia, strongylodiasis may be a problem. Because stool microscopy lackssensitivity, it is probably more cost effective to treat than to screen all patients from highendemic countIn the Cambodian National Leprosy Elimination Program (NLEP),3-month pre-packed tapered dose blister packs of steroids for the treatment of leprosyreactions in the field are available for use by leprosy control program supervisors. Often cases
of leprosy reaction in the field, particularly chronic type 2 reactions are not appropriatelyreferred but are given two or more courses of these pre-packed blister packs of steroids. Following the fatal outcome in this case and the discovery of several other S. stercoralispositive stool samples in patients on treatment with steroids for leprosy reactions in theNational Rehabilitation Unit, the NLEP has recommended to field staff that no more than one3-month pack is issued to any patient in the field. On recurrence of the reaction, the patientshould be referred to the hospital. In addition, the NLEP is considering adding albendazole tothe pre-packed steroid blister packs. As these pre-packed steroids are available and used byparamedical staff in various developing countries, program managers may want to considermaking similar recommendations for their own countries.
The case described here is an illustration of SH in a patient who received high dose
steroids for a medical indication and prescribed by a physician. In developing countries,however, over-the-counter availability of steroids is the rule rather than the exception.Moreover, steroids are frequently mixed with herbal medicines by traditional healers. Therefore, every physician working in a strongyloidiasis endemic region, or treating patientsfrom endemic regions, needs to be aware of the SH syndrome and systematically enquireabout potential steroid use or look for other signs of steroid abuse.
Leprosy patients living in strongyloidiasis endemic areas may develop a life threatening SHwhen their leprosy reactions are treated with steroids, without pre-treatment of an S. stercoralisinfection. SH is an, often, fatal syndrome that can be prevented. It is more effective to treat allpatients at risk before the start of immunosuppressive therapy, than to screen patients for apossible infection, especially when working in an endemic area. Early diagnosis and treatmentis important in SH. Albendazole is well tolerated, but data are lacking for its use in SH. Ivermectin is more effective for the treatment of disseminated strongyloidiasis and isrecommended for the treatment of S. stercoralis in SH. We strongly recommend the inclusionof albendazole and ivermectin in Cambodian referral hospitalsвҖҷ formulary. We alsorecommend a price reduction of ivermectin to make it accessible for developing countries.
We thank Professor Fons Van Gompel and Professor Bruno Gryseels from the Institute ofTropical Medicine in Antwerp for their critical review and comments. B. L. and R. T. received financial support from the Non-Governmental Organization HOPE Worldwide. L. L. received a research grant ITM/DGCI framework agreement, project 96120. S. G. wassupported by CIOMAL (Cambodia).
1 Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis, 2001; 33: 1040вҖ“1047. 2 Shinozaki F, Takada K, Tamai T et al. [Strongyloidiasis associated with multiple myeloma in Ehime prefecture].
Kansenshogaku Zasshi, 1994; 68: 539 вҖ“ 543.
3 Davidson RA, Fletcher RH, Chapman LE. Risk factors for strongyloidiasis. A case-control study. Arch Intern
Strongyloides hyperinfection in a leprosy patient
4 Tsai HC, Lee SS, Liu YC et al. Clinical manifestations of strongyloidiasis in southern Taiwan. J Microbiol
Immunol Infect, 2002; 35: 29 вҖ“ 36.
5 Mahmoud AF. State-of-the-art clinical article: Strongyloidiasis. Clin Infect Dis, 1996; 23: 949вҖ“953. 6 Graeff-Teixeira C, Leite CS, Sperhacke CL et al. Prospective study of strongyloidosis in patients with
hematologic malignancies. Rev Soc Bras Med Trop, 1997; 30: 355 вҖ“ 357.
7 Nair D. Screening for Strongyloides infection among the institutionalized mentally disabled. J Am Board Fam
8 Fisher D, McCarry F, Currie B. Strongyloidiasis in the Northern Territory. Under-recognised and under-treated?
9 Karolyi Z, Eros N, Kriston R. [Cutaneous manifestations of strongyloidosis]. Orv Hetil, 1999; 140: 191вҖ“194.
10 Bannon JP, Fater M, Solit R. Intestinal ileus secondary to Strongyloides stercoralis infection: case report and
review of the literature. Am Surg, 1995; 61: 377 вҖ“ 380.
11 Boken DJ, Leoni PA, Preheim LC. Treatment of Strongyloides stercoralis hyperinfection syndrome with
thiabendazole administered per rectum. Clin Infect Dis, 1993; 16: 123 вҖ“ 126.
12 de Silva N et al. Anthelminthics. A comparative review of their clinical pharmacology. Drugs, 1997; 53:
13 Weller PF. Strongyloidiasis. UpToDate, 1998; 7.2: 1вҖ“5. 14 Torres JR, Isturiz R, Murillo J et al. Efficacy of ivermectin in the treatment of strongyloidiasis complicating AIDS.
Clin Infect Dis, 1993; 17: 900 вҖ“ 902.
15 Nozais JP, Thellier M, Datry A, Danis M. [Disseminated strongyloidiasis]. Presse Med, 2001; 30: 813вҖ“818. 16 Gelber M, Rodrig J. [Strongyloides stercoralis hyperinfection]. Harefuah, 1996; 130: 90вҖ“92, 143. 17 Chiodini PL, Reid AJ, Wiselka MJ et al. Parenteral ivermectin in Strongyloides hyperinfection. Lancet, 2000; 355:
18 Hagelskjaer LH. A fatal case of systemic strongyloidiasis and review of the literature. Eur J Clin Microbiol Infect
19 Muennig P, Pallin D, Sell RL, Chan MS. The cost-effectiveness of strategies for the treatment of intestinal
parasites in immigrants. New Engl J Med, 1999; 340: 773 вҖ“ 779.
20 Hui JY, Woo PC, Lo SS, Chan JC. Over-the-counter medication and its effects. Lancet, 2002; 359: 1120.
EuropГҰiske principper for behandling af al- mindelige hovedpinesygdomme i almen praksis TJ Steiner1, K Paemeleire2, R Jensen3, D Valade4, L Savi5, MJA Lainez6, H-C Diener7, P Martelletti8 og EGM Couturier9* pГҘ vegne af Det EuropГҰiske Hovedpine Forbund og Lifting The Burden : Den Globale Kampagne for at reducere hovedpinebelastningen i verden NГёgleord Det EuropГ
Wechsel vom Raucher zum Nichtraucher Auszug aus: http://www.netdoktor.de/Gesund-Leben/Rauchen/Rauchstopp/Nikotinentzug-Abschied-vom-Gli-2420.html http://www.netdoktor.de/Gesund-Leben/Rauchen/Rauchstopp/Zehn-Tipps-zum-Aufhoeren-392.html Nikotinentzug - Abschied vom GlimmstГӨngel KГ¶rper und Geist gefordert Bei der TabakabhГӨngigkeit sind sowohl kГ¶rperliche als auch psychisc
 The results of histopathology of the duodenal biopsies performed at the other hospital
arrived after the patientвҖҷs death, and showed massive amounts of S. stercoralis larvae in themucosa (see
The course of this patientвҖҷs illness with diarrhoea, cough, peripheral eosinophilia, ileus,sepsis and the presence of many strongyloides stercoralis larvae in the stool and in theduodenal mucosa are strongly suggestive of strongyloides hyperinfection.
The results of histopathology of the duodenal biopsies performed at the other hospital
arrived after the patientвҖҷs death, and showed massive amounts of S. stercoralis larvae in themucosa (see
The course of this patientвҖҷs illness with diarrhoea, cough, peripheral eosinophilia, ileus,sepsis and the presence of many strongyloides stercoralis larvae in the stool and in theduodenal mucosa are strongly suggestive of strongyloides hyperinfection.