Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Information for patients having scans elsewhere whilst undergoing treatment at the lister
SO, WHAT IS A “POOR RESPONDER”? We now understand why ovarian reserve is important and how we assess it, but how is “poor response” defined? Unfortunately, there is no universally accepted definition for the `poor responding’ patient in a cycle of assisted reproduction, although what is not in doubt is that these patients invariably have lower pregnancy rates compared with `normal' responders. In essence it is the “failure of development of sufficient numbers of mature follicles to proceed to egg collection or the yield of only a few follicles following a suitably dosed ovarian stimulation regime”. The two commonest criteria used to characterize poor response are the number of developed fol icles and number of eggs retrieved after a standard-dose ovarian stimulation regime. The absolute number used as a cut- off is variable but it is usual y between 3-5. More importantly may be a comparison of how many you produce compared to the average for your age. The average number of eggs col ected by age in a cycle of ART at The Lister Fertility Clinic between 2005-2013 are:
Other useful indicators of a poor responder:
Low peak oestrogen levels on the day of optimal egg maturity A history of previous IVF cycle cancellations High doses or duration of medication required
HOW IS SUCCESS MAXIMISED IN “POOR RESPONDERS”? In our practice we aim, as much as possible, to base our recommendations on a solid evidence base. However, within the emotive field of infertility top quality trials that compare a treatment to a dummy/placebo treatment (randomised trials) are exceptionally hard to undertake. As a consequence we aim to draw together the best available evidence that we can to decide on your optimal management.
1. CYCLE PROTOCOLS: Several stimulation protocols have been suggested to improve outcome in poor
responding patients. The evidence of benefit for many of these over the standard “long protocol” is often limited and the final decision wil be made in conjunction with your doctor at your consultation.
a. Short Agonist Protocol: This protocol takes advantage of the initial release (flare – hence often
called “flare protocol”) of a woman’s own FSH that occurs soon after starting the GnRH agonist to maximise response.
b. Microdose Protocol: This is a variation of the short agonist protocol that uses as smaller dose of
GnRH agonist to minimise the suppressant effect on the ovary.
c. Antagonist Protocol: This protocol aims to maximize outcome in poor responders by avoiding
suppressing the ovary at the time of fol icle recruitment.
2. DRUG DOSES AND COMBINATIONS: An initial poor response to gonadotrophin stimulation often leads
clinicians to increase the dosage of medication for ovarian stimulation. However, few studies have demonstrated benefit in such a strategy. The number of follicles available for growth when starting ovarian stimulation is fixed on any given month and cannot be altered by increasing dosages. It is therefore unusual for us to recommend doses beyond 300-450iu/day. Similarly, novel combinations of stimulation medication is also often a tool we use to maxiise response.
3. ADJUVANT TREATMENTS: Several medications taken prior to or during a cycle have been suggested to a. Anti-Oestrogens: Clomiphene or more recently “Aromatase Inhibitors” such as Letrozole are
used in conjunction with FSH injections to maximise ovarian response. They act to mask the brain to women’s own oestrogen levels which leads to the stimulation of the pituitary gland in an effort to produce more FSH to act on the ovary.
b. Oestrogen Priming: Pre-treatment with oestrogen, often in the form of the combined
contraceptive pill, is often used to “prime” the follicles in the ovary prior to stimulation.
c. DHEA: This is a testosterone-related hormone that is a precursor to the production of both
testosterone and oestrogen and has been suggested to increase outcome in this group of women. Initially egg number was suggested to improve but recent evidence does not support this and suggests an improvement in embryo quality. The mechanism of any potential benefit remains uncertain but as DHEA decreases with age, it may be that supplementation al ows more efficient production of testosterone and oestrogen required for follicle growth. Other suggested mechanisms are that DHEA decreases the degeneration of fol icles, increases the effect of FSH on the ovary or may decrease miscarriage by minimising genetic abnormalities in embryos.
As a mild male hormone, other suggested positive effects of DHEA are an increase in energy levels and libido and potential side effects, although rare at the appropriate dose are oily skin, acne and hail loss. As it is not drug licensed in the UK for this indication, and in essence is a supplement it cannot be prescribed directly by us but we can advise you on where best to source it. The recommended dose is 25mg three times a day for at least two months.
d. Coenzyme Q10: This is a natural y occurring micronutrient that is produced by the energy
producing component (mitochondria) of our cel s. It is safely used with good evidence in many areas of medicine such as cardiac and neurological disease and early studies have suggested a possible improvement in embryo quality.
The recommended dose is 300mg twice a day.
4. MISCELLANEOUS: a. Natural IVF: This involves scanning during a cycle without medication to stimulate the ovary and
the col ection of the naturally growing egg for use for IVF/ICSI. Although, the first IVF birth in 1978 involved the use of natural IVF, safe stimulation regimes that clearly improve chances of pregnancy are now the mainstay of ART cycles. However, in poor responders, where a low egg number is expected anyway, some advocate the use of natural IVF to minimise unnecessary drug exposure and al ow more frequent treatments. Although this is an option in certain circumstances (i.e when high doses of medication stil only yield one egg), this is not something we routinely recommend in view of the increase in chances of pregnancy shown in the tables above even with col ection of only one extra egg. b. Alternative Medicine: Traditional Chinese Medicine and Homeopathy have been suggested as possible remedies for ovarian reserve issues. However, there is no evidence to support their use and the exact ingredients (whether beneficial or possibly harmful) are often difficult to accurately identify Acupuncture and Yoga have also been suggested to positively affect blood flow to the uterus and potential y improve outcome. Again, there is no evidence of benefit in outcome in this group of patients. However, we would recommend them as relaxation techniques and to improve quality of life if they are something you feel you would benefit from. c. Other Drugs: Many other drugs are often recommended during fertility treatment, such as aspirin, heparin and steroids. Although such drugs may wel be indicated for other reasons, there is no evidence of benefit of their use solely for poor responders or in those with a low ovarian reserve. d. Laboratory Techniques: Our aim is always to maximise the quality of transferred embryos by
appropriate selection techniques and where embryo number and quality allow transfer of embryos on Day 5 (blastocyst embryos). Although other laboratory techniques such as the routine use of intracytoplasmic sperm injection (ICSI) or assisted hatching (AZH) in couples with a low ovarian reserve or poor response have previously been suggested, there is no evidence of benefit of their use and they may in fact worsen outcome. The choice of how best to fertilise the eggs (i.e. between IVF, ICSI or IMSI) should depend on sperm quality and if an extra invasive procedure of injecting potentially fragile eggs can be avoided that is what we favour.
5. EGG DONATION: Although the decision to move on to treatment with donor eggs is often a difficult one, it
is important that you are aware from the outset that this is an available option and that it may offer the most realistic chance of pregnancy in those with a low ovarian reserve.
Donors are invariably <35 years old and the age of the recipient has minimal impact on outcome. As a consequence, our egg donation program has Pregnancy rates and Livebirth rates of 61% and 43% pre embryo transfer respectively between 2005-2013. There are many factors that need to be taken into consideration prior to embarking on egg donation and a session with our counsel or is mandatory to al ow these to be discussed. This is something you may also benefit from at any point during your time under our care to help deal with the implications of your diagnosis and your treatment.
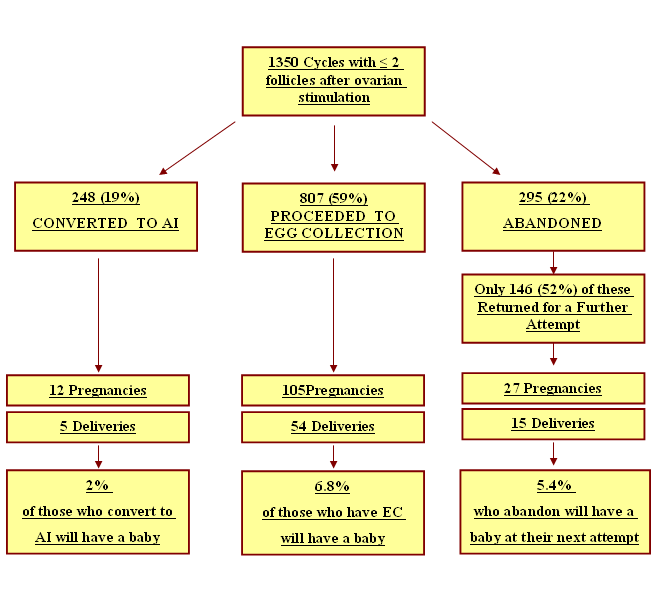
IF I STILL RESPOND POORLY DURING A CYCLE – WHAT ARE MY OPTIONS? Traditionally, many clinics will recommend cycle cancellation in the face of a poor response. The decision to cancel a cycle of assisted reproduction incorporates emotional, financial and clinical considerations and in a situation of poor response, such a decision is often made for one of two reasons. Firstly the realisation of the poor potential outcome in conjunction with the potential financial burden may prompt couples to abandon and consider other treatment modalities (egg donation) or adoption services. Secondly, the perceived possibility of improved response in future cycles as a consequence of lessons learnt. However, although the chances of a successful outcome may be lower than those with a better response, pregnancies do occur (as in the figure showing success rate by egg number in the “how is ovarian reserve assessed” document) and proceeding with an egg col ection and IVF may stil be the best chance you have with no guarantee of a better response in future attempts. To try and look at this we have analysed all cycles between 1998-2010 in those who, after ovarian stimulation, have produced two or less follicles and in whom cycle cancellation may have been previously been the recommended of the three options: 1. Proceed to Egg Collection (EC) 2. Convert to a cycle of artificial insemination (AI) 3. Cancel cycle and consider future options. Outcome of cycles with < 2 follicles (1998 – 2010)
It was clear therefore that, although response and therefore pregnancy outcome may be suboptimal, proceeding to VEC remained the best chance of success, particularly with increasing age. We would therefore recommend careful counseling of couples in this situation focusing on this data, using our database to counsel people of their chances by age and exact number of follicles and discuss the possibility that, if they cancel, there is no guarantee of a better response in the future.
Pediatr Allergy Immunol 2010: 21: 954–961Filaggrin gene variants and atopic diseases inearly childhood assessed longitudinally frombirthBønnelykke K, Pipper CB, Tavendale R, Palmer CNA, Bisgaard H. Filaggrin gene variants and atopic diseases in early childhood assessedPipper1, Roger Tavendale2, Colin N. A. Pediatr Allergy Immunol 2010: 21: 954–961. 1Copenhagen Studies on Asthma in Child
Case Study: Tamoxifen A Drug’s Evolution From Fertility to Many Stages of Cancer Tamoxifen is: • FDA approved as Nolvadex (brand name) • Currently most prescribed cancer drug in breast cancer • Used by millions in over 110 countries • SERM: (selective estrogen receptor modulators) exert estrogen agonist action in some target tissues while acting as estrogen

 a. Short Agonist Protocol: This protocol takes advantage of the initial release (flare – hence often
a. Short Agonist Protocol: This protocol takes advantage of the initial release (flare – hence often  The recommended dose is 300mg twice a day.
4. MISCELLANEOUS:
The recommended dose is 300mg twice a day.
4. MISCELLANEOUS: