Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Malaria.gov.sd
Am. J. Trop. Med. Hyg., 68(2), 2003, pp. 153–158Copyright 2003 by The American Society of Tropical Medicine and Hygiene
DESCRIPTIVE STUDY ON THE EFFICACY AND SAFETY OF ARTESUNATE
SUPPOSITORY IN COMBINATION WITH OTHER ANTIMALARIALS IN THE
M. I. AWAD, A. M. Y. ALKADRU, R. H. BEHRENS, O. Z. BARAKA, AND I. B. ELTAYEB
Department of Pharmacology, Faculty of Pharmacy, and Department of Internal Medicine and Applied Therapeutics, Faculty ofMedicine, University of Khartoum, Khartoum, Sudan; Department of Infectious and Tropical Diseases, London School of Hygieneand Tropical Medicine, London, United Kingdom
Documentation on the efficacy of artesunate in Africa is limited, and no experience of artesunate use in
Sudan is documented. Severe malaria in rural areas of Sudan, where facilities for the safe and effective use of parenteralquinine are lacking, is a frequent problem. Early treatment with artesunate suppositories would provide asimple methodfor use by unskilled staff and would be an alternative approach to treat malaria in settings with poor resources. Wedescribe a hospital-based study of rectal artesunate in 100 adult patients with severe falciparum malaria with a dosederived from pharmacokinetic data (200 mg every 8 hours) over 3 days, which halted progression of severe disease andhad a low fatality rate. The dosage schedule led to a rapid clinical response and reduced parasite clearance and feversubsidence times of (31.5 ± 10.1 hours) and (31.4 ± 11.1 hours). The sequential treatment of rectal artesunate with eitherdoxycycline or pyrimethamine/sulfadoxine or mefloquine resulted in similar clinical cure rates of around 100%, and thecombination of artesunate with either doxycycline or pyrimethamine/sulfadoxine was equally effective as mefloquine inpreventing recrudescence. There were no significant adverse effects or signs of toxicity related to the treatment observedduring the 28-day follow-up. The combination regimens could be used in areas where there is limited access to parenteraltherapy for malaria.
Suppositories of artesunate have been developed for rectal
administration as an alternative to oral or parenteral therapy.
The increase in malaria disease burden in Africa is of great
Clinical studies of rectal administration of artesunate in the
concern nationally and internationally. An estimated 300–500
treatment of malaria have been undertaken in Thailand, My-
million new cases of malaria and an estimated 1.5–2.7 million
anmar, Ecuador, Kenya, and Gabon.11–16 Table 1 summarizes
deaths occur each year. The highest mortality (>90%) occurs
the doses used and the efficacy obtained in these studies.
in children <5 years old in Africa.1 Plasmodium falciparum
Suppositories are a major advance in the treatment of severe
malaria is associated with severe morbidity and mortality, and
malaria, especially in rural settings, where resources are mea-
in the absence of early diagnosis and effective treatment, it
ger and the referral of cases is not possible. It is recommended
that further studies be carried out for the quantification of the
Resistance to most antimalarial therapies is well docu-
efficacy of artesunate suppositories in the treatment of severe
mented worldwide. Multidrug resistance is an increasing
problem in Africa and poses a threat to the current manage-
In Sudan, there has been a rapid spread of chloroquine-
ment of malaria with inexpensive drugs such as chloroquine
resistant P. falciparum infections. Parenteral quinine is the
and pyrimethamine/sulfadoxine.3 Drugs derived from arte-
main drug widely used in the management of severe malaria.
misinin have been shown to be extremely effective against
It is available only in urban settings, where expertise and
multidrug-resistant P. falciparum malaria and severe ma-
equipment are available. The use of artesunate rectocaps
laria.4 Because their quantitative determination in biologic
(Mepha Pharmaceutical Research, Aesch-Basel, Switzerland)
fluid is a challenging problem, different dosage regimens have
in treatment of severe malaria may provide advantages.
been proposed that are largely empirical.5 The selection of
Although artemisinin compounds are effective against mul-
optimal dosage regimens requires precise information on the
tidrug resistance, when administered alone, these agents have
led to recrudescence rates of 10–100%, depending on the
Artesunate is a semisynthetic derivative of artemisinin
dose and duration of treatment and severity of the disease.19
whose water solubility facilitates absorption7 and provides an
Current recommendations are that artemisinin derivatives
advantage over artemisinin because it can be formulated as
should be used only in combination with other antimalarials
oral, rectal, intramuscular, and intravenous preparations.
to reduce the development of resistant parasite strains. Me-
Artesunate is rapidly hydrolyzed to dihydroartemisinin,
floquine has been used widely in combination with artemisi-
which is the most active schizonticidal metabolite. Extravas-
nin derivatives and has produced radical cure rates of
cular administration of artesunate results in a more rapid sys-
>90%.11,12 White and Olliaro20 and White et al.3 recom-
temic availability of artesunate compared with intramuscular
mended that clinical studies are needed to assess the efficacy
artemether. This pharmacokinetic advantage may provide a
and safety of artemisinin compounds in combination with
clinical advantage in the treatment of severe malaria.8 Rectal
artesunate has been shown to be absorbed rapidly, with a
The objectives of this study were to investigate the efficacy
considerable interindividual variability.9,10 Artesunate is
and safety of rectal artesunate in combination with 3 other
highly effective against multidrug-resistant falciparum ma-
antimalarials in the treatment of severe malaria and to deter-
laria and severe malaria in Vietnam, Thailand, China, and
mine recrudescence rates after treatment of adult Sudanese
Myanmar7; however, limited studies have been carried out in
patients. The regimens evaluated were (1) artesunate sup-
positories for 3 days followed by doxycycline capsules for 4
Published results of clinical trials in the treatment of P. falciparum malaria by rectal artesunate
0,4,8,12,24,36,48,60 h(1,600 mg) + MF750 mg at 72 h,500 mg at 84 h
0,4,8,12,36,48,60 h (1,400 mg)+ MF 750 mg at72 h, 500 mg at84 h
0,12,24,36,48, 60 h(1,200 mg) + MF750 mg at 72 h,500 mg at 84 h
3 da ys, MF750 mg on day 4and 500 mg 12 hapart
200 mg/12 h onday 1, 200 mgon days 2 and3, MF 750 mgon day 4 and500 mg 12 hapart
day 1,200 mg/12 h ondays 2 and 3,then MF250 mg/8 hstarted on day 4
0,4,8,12,18,24,48,60 h, then MFTD 1,000 mg in2 doses 8 hapart
Note. Radical cure rate (%): Clinical cure without recrudescence by day 28. MF, mefloquine; P/S, Pyrimethamine/sulfadoxine; SD, single dose; TD, total dose.
days, (2) artesunate suppositories for 3 days followed by
The inclusion criteriafor apatient to enter the study were
single-dose pyrimethamine/sulfadoxine tablets, and (3) arte-
evidence of severe malaria with Ն1 of the WHO criteriaof
sunate suppositories for 3 days followed by mefloquine tab-
severe disease, age 18–60 years, and parasitemia of >10,000
lets divided into 2 equal doses 24 hours apart.
parasites/l with P. falciparum alone. The exclusion criteriaincluded pregnancy, breast-feeding, hemorrhoids, previousrectal surgery, diarrhea for Ն12 hours, and recent treatment
with an antimalarial over the previous 2 weeks. Patients whofulfilled the inclusion criteriawere selected randomly during
Patients. The study was conducted at Omdurman Teaching
their presentation at the Accident and Emergency Depart-
Hospital and the Tropical Disease Hospital in Khartoum
ment and sequentially entered into 1 of 3 groups. The
State. A total of 2,400 febrile patients were evaluated be-
Sudanese Ethical Committee (Federal Ministry of Health,
tween January 2000 and January 2001. Patients with micro-
National Health Laboratory) gave ethical approval for the
scopically diagnosed P. falciparum malaria were considered
study. A written consent was obtained from patients or rela-
for entry if they had clinical, biochemical, and parasitologic
evidence of severe malaria based on the World Health Orga-
Clinical procedures. A full clinical examination was under-
nization (WHO) criteria of severe diseases.2,21
taken by a general practitioner on admission. Comatose pa-
tients were graded using the Glasgow Coma Scale every 6
mained so for at least 48 hours), time to consciousness (time
hours until the patient recovered full consciousness with a
from the initiation of therapy until the Glasgow Coma Score
Glasgow Coma Scale of 15. Rectal temperature, blood pres-
ס 15), clinical cure rate (the percentage of patients who had
sure, pulse, and respiratory rate were measured every 6 hours
initial recovery with complete initial disappearance of para-
during the first 24 hours, then every 12 hours until day 4 and
sitemia within 7 days), and fatality rate (the percentage of
once daily to day 7, then on the follow-up days 7, 14, 21, and
patients who died after the initiation of therapy). Laboratory
28. The patients were evaluated for the evolution of the signs
measures included parasite clearance time (time from the ini-
and symptoms, and any new events elicited during treatment
tiation of therapy until the first negative blood film that re-
daily for 7 days and weekly till day 28 were recorded.
mained negative for 48 hours), radical cure rate (the percent-
Laboratory procedures. The species differentiation was ob-
age of patients who had clinical cure without recrudescence
tained from thin smears. A parasite count was obtained using
by day 28), and recrudescence rate (defined according to
thick blood films, counted as the number of parasites per 200
WHO classification during 28-day follow-up). Improvement
white blood cells. Parasite clearance was monitored using
of impaired biochemical and hematologic parameters (time
thick blood films every 6 hours during the first 24 hours, then
from the initiation of therapy until the improvement of the
every 12 hours to day 4 and daily to day 7. Follow-up films
impaired biochemical and hematologic parameters to normal
were taken on days 14, 21, and 28. The thick blood films were
considered negative if no parasites were seen in 200 oil im-
Safety assessment. Side effects were defined as signs and
symptoms that first occurred or became more severe after
Biochemical and hematologic tests included hemoglobin,
treatment was started. Any new events elicited during the
hematocrit, reticulocyte count, white blood cell total and dif-
treatment also were considered as side effects. Biochemical
ferential counts, plasma glucose, plasma total bilirubin, serum
and hematologic parameters were evaluated before and after
urea, creatinine, and liver function tests. These tests were
initiation of therapy to detect any drug-associated effects.
done on admission and repeated on days 7, 14, 21, and 28. Data analysis. The demographic, clinical, and laboratory
More tests were performed as necessary for the management
data for each patient were entered in a form, then entered in
SPSS V9 for the performance of the descriptive and compara-
Management of patients. Patients with severe malaria re-
tive statistical analysis. The comparison of data within the
ceived nonspecific treatment according to the guidelines pub-
groups was carried out by paired Student t-test for normally
lished by Gilles2 and WHO.21 The specific treatment included
distributed data and by Wilcoxon signed rank test for data
the use of the following antimalarial drugs: artesunate sup-
that were not normally distributed. One-way analysis of vari-
positories, 200 mg (Plasmotrim-200 Rectocaps-Mepha), me-
ance was used for the comparison between the groups.
floquine tablets, 250 mg (Mephaquin-Mepha), doxycyclinecapsules, 100 mg (Zadorin-Mepha), and pyrimethamine/sulfadoxine, 25 mg/500 mg (Fansidar Roche). Therapeutic regimens used. All patients were treated with
rectal artesunate, 200 mg every 8 hours for 3 days (total dose,
A total of 2,400 adult patients who presented with fever or
1,800 mg), then entered into an open-label design to receive
ahistory of fever to the trial site were screened with blood
films during January 2000 to January 2001. Of patients, 420(17.5%) were found to have positive blood films, 404 (96.2%)
1. Group A (35 patients): Doxycycline capsules, 100 mg ev-
had P. falciparum, and the rest had P. vivax. Of the 404 cases,
ery 12 hours for 4 days, started 12 hours after the last dose
73.3% were considered to have uncomplicated P. falciparum
malaria, and 26.7% (n ס 108) had criteria ascribed by WHO
2. Group B (35 patients): A single dose (3 tablets) of pyri-
methamine/sulfadoxine, 12 hours after the last dose of
A total of 100 patients (79 men and 21 women) agreed to
participate in the study and received an initial treatment with
3. Group C (30 patients): Mefloquine tablets (total dose, 15
artesunate rectocaps for 3 days. For the second drug, the
mg/kg body weight), split in 2 equal doses 24 hours apart,
patients were divided into 1 of the 3 treatment groups (35 in
started 12 hours after the last dose of artesunate
group A, 35 in group B, and 30 in group C). Age range was18–65 years with a mean (SD) of 30.5 (11.7) years, and weight
A pharmacokinetic study of oral and rectally administered
range was 42–97 kg with a mean (SD) of 64.9 (9.1) kg. The 3
artesunate in Sudanese healthy volunteers was used to devise
groups were comparable in demographic data, clinical char-
the suggested dosage regimen of rectal artesunate, 200-mg
acteristics, and laboratory findings (Table 2).
rectocaps every 8 hours.10 Patients were laid in a left lateral
After the treatment regimens, surviving patients were fol-
position, and an artesunate rectocap was inserted into the
lowed for 28 days. Home visits were conducted for patients
rectum beyond the anal verge by a trained nurse. The patients
who failed to show for the follow-up. One patient died 7 hours
were confined to bed for at least 1 hour after the insertion; if
after the first dose of artesunate. Fourteen patients had cere-
the rectocap was expelled within 1 hour of administration,
bral malaria with a mean (SD) Glasgow Coma Scale of 6 (1);
49 patients were jaundiced with a plasma total bilirubin
Evaluation criteria for the treatment efficacy and safety Effi-
greater than twice-normal laboratory range. All patients had
cacy assessment. The following laboratory and clinical end
a parasitemia of >10,000 parasites/l, 19 patients had hyper-
points were used to measure response to treatment objec-
pyrexia (>40.1°C), and 37 patients were hypoglycemic. Seven
tively: fever clearance time (time from the initiation of
patients had algid malaria with systolic blood pressure <80
therapy until body temperature decreased to 37°C and re-
mm Hg, and 12 patients had elevated serum creatinine and
Mean ± SD of the clinical, hematologic, and biochemical parameters at admission of the 3 second-drug treatment groups
Hemoglobin (g/dl) (men, 13–17 g/dl; women, 12–15 g/dl)
Serum creatinine (mg/dl) (0.5–1.5 mg/dl)
Note. Values in parentheses are laboratory normal range.
blood urea greater than twice normal. Of patients, 49 had >1
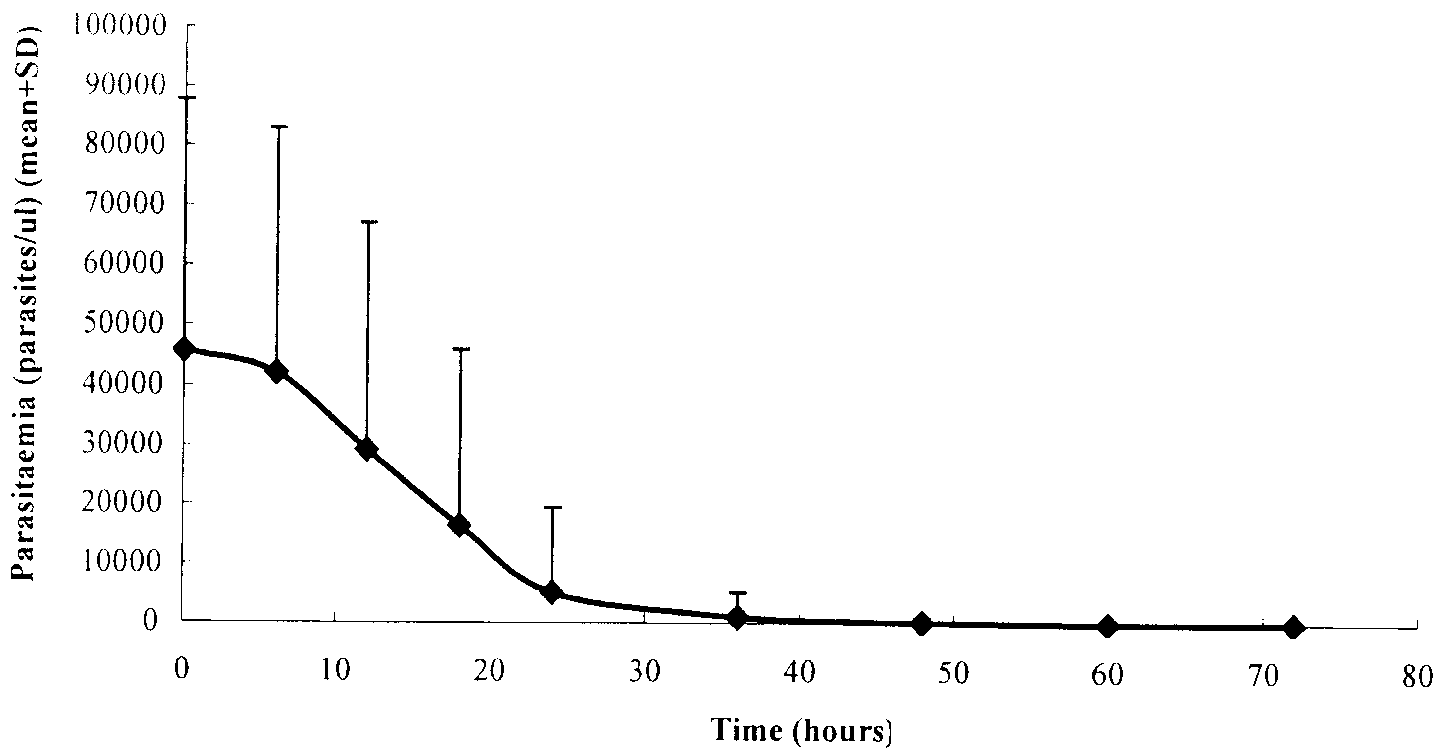
parasitemia by 24 hours was 88.8% (11.2%) and by 36 hours
criteria of severe malaria as ascribed by WHO (Table 3).21
was 99.8% (0.2%). At baseline enrollment, gametocytes were
All patients clinically improved within 3 days of starting
detected in 5 patients. No new gametocytemia was detected
treatment with artesunate rectocaps. Parasitemia clearance
during the treatment or follow-up. The mean (SD) clearance
and fever clearance times are shown in Figures 1 and 2. The
time of gametocytes was 4.2 (1.6) days, supporting the evi-
(mean ± SD) of initial parasitemia was 45,683 ± 42,068 para-
dence that artesunate clears gametocytes, preventing further
sites/l (range, 13,133–25,0000 parasites/l). In 87 patients,
parasitemia ranged from 13,133–100,000 parasites/l, and 13
Figure 2 shows the clearance of fever. The overall mean
patients had parasitaemia >100,000–250,000 parasites/l.
(SD) initial rectal temperature before treatment was 39°C
There was a highly statistically significant reduction in the
(1.3°C) (range, 34–40.6°C). There was a highly significant re-
mean parasitemia at 6 hours and thereafter following artesu-
duction from the initial elevated temperatures achieved by 6
nate rectocaps administration (P < 0.001). The mean (SD)
hours after starting treatment (P < 0.001). The combined
decrease in parasitemia was 36.2% (2.5%) by 12 hours and
mean (SD) fever clearance time was 31.4 (11.1) hours (range,
After the insertion of artesunate rectocaps, the overall
The mean resolution time for the signs and symptoms
mean (SD) parasitemia clearance time was 31.5 hours (10.1
ranged from 24–58.3 hours. All patients had excellent initial
hours) (range, 18–72 hours). The mean (SD) reduction of
clinical improvement, and 87% of the patients were asymp-tomatic within 3 days of starting treatment. Full consciousnesswas gained by 78.6% of comatose patients at 24 hours, and
the remaining patients regained normal higher function by 36
Patients with more than one criteria of severe malaria
Hematologic parameters recovered with no evidence of
marrow suppression during artesunate treatment or after thesecond drug in all treatment groups. Liver function, renal
Cerebral malaria (GCS Յ 6) + hyperpyrexia
function, and blood glucose were comparable at presentation
Cerebral malaria (GCS > 6 Յ 8) + plasma total biliru-
within the 3 treatment groups. All patients recovered except
for 1 death at 7 hours after the first artesunate dose. There
Cerebral malaria (GCS Յ 6) + hyperpyrexia
were no recrudescences in any patient by day 28 (radical cure
(>40.1°C) + plasma total bilirubin >3 mg/dl
Hyperparasitemia (>100.000 P/l) + plasma total bili-
rubin >6 mg/dl + hyperpyrexia(>40.1°C) + general-ized convulsions + hemoglobin <8.5 g/dl
Hyperparasitemia (>100.000 P/l) + plasma total bili-
rubin >3 mg/dl + hypoglycemia<40 mg/dl + gener-alized convulsions + serum creatinine >3 mg/dl
Algid malaria (SBP < 80 mmHg) + plasma total bili-
Algid malaria (SBP < 80 mmHg) + plasma total bili-
rubin >3 mg/dl + serum creatinine >3 mg/dl
Hyperpyrexia(>40.1°C) + generalized convulsions +
Serum creatinine >3 mg/dl + urine output <400 ml /24
h + hypoglycemia<40 mg/dl + plasmatotal biliru-bin >3 mg/dl
Hypoglycemia<40 mg/dl + generalized convulsions +
* One fatal outcome. The criteria of severe falciparum malaria as ascribed by WHO, 2000.
tory, cultural objection to the use of suppositories needed tobe considered. Cultural acceptance is variable and respondsto education. There was little resistance to the use of thesuppositories by patients or their relatives.
The clinical and laboratory findings during and after the
treatment showed no evidence of toxicity or side effects to the3 combination regimens during treatment and the 28-day fol-low-up. In group B, there was an increase in the number ofpatients with hemoglobin and hematocrit below normal atdays 7 and 14, which suggested that this combination mayhave an adverse effect. Previous studies using pyrimethamine/sulfadoxine combined with artesunate in the treatment of un-complicated falciparum malaria reported that there were noadverse effects on laboratory parameters.24 The clinical sig-
nificance of this finding remains to be confirmed in a largernumber of patients.
In studies in which artemisinin compounds were adminis-
tered alone, recrudescence rates varied from 10% to 100%depending on the dose, duration of treatment, and severity of
The present study investigated a larger number of patients
the disease.19 These drugs often are combined with meflo-
than reported in other studies. Using pharmacokinetic data
quine to reduce the rate of recrudescence. Limited studies
from healthy volunteers, an appropriate dose of artesunate
reported the efficacy of doxycycline or pyrimethamine/
was selected for administration per rectum that would be ex-
sulfadoxine combined with artesunate in treatment of uncom-
pected to provide blood levels of dihydroartemesinin above
plicated malaria. The present results indicate that sequential
the minimum inhibitory concentration that eliminates 90% of
treatment of severe malaria with artesunate rectocaps fol-
the parasites (MIC ) for 5.3 ± 2.1 hours.10 The rapid parasite
lowed by either doxycycline (100 mg every 12 hours for 4
clearance and deffervescence of fever in all 99 patients con-
days) or a single dose of pyrimethamine/sulfadoxine was
firms the dosing schedule in this group of patients was entirely
equally effective to that followed by mefloquine in preventing
appropriate. The parasitemia and fever clearance times in this
recrudescence. The dosage regimen of mefloquine (total dose
study were significantly shorter than that reported by Looa-
15 mg/kg body weight) divided in 2 equal doses 24 hours apart
reesuwan et al.11,12 and Thwe et al.13 but not significantly
used in this study improved its tolerability because no serious
different from that reported by Eduardo and Gomez14 and
Artesunate rectocaps in treatment of severe malaria have
The choice of second agent was made based on available
many advantages in rural settings in developing countries
data of mefloquine from Southeast Asia and cost because
such as Sudan. Their administration does not require sophis-
pyrimethamine/sulfadoxine and doxycycline are inexpensive
ticated facilities and skilled personnel, and they can be used as
and widely available. All 3 drugs proved equally effective,
an alternative to parenteral quinine with all its known side
producing radical cure rates of 100%. The only death in the
effects. The use of artesunate rectocaps in rural areas where
study was a 50-year-old man, who despite a reduction in par-
malaria transmission is higher and the disease is more preva-
asitemia at 6 hours from 160,000 to 142,000 parasites/l died
lent is more appropriate for the type of health facilities avail-
suddenly 7 hours after starting treatment. Previous studies
able. The early administration of treatment to patients where
reported fatality rates of 40% in severely ill malaria pa-
referral is not possible, especially for children, could reduce
tients.23 The mortality rates reported in 2 other studies using
complications and reduce mortality. The use of a single dose
artesunate rectocaps for the treatment of severe malaria were
of pyrimethamine/sulfadoxine or 2 doses of mefloquine in
2.5% and 13.6%.14,15 In these 2 studies, the number of pa-
adults and children would improve compliance to the impor-
tients and the total dose of rectal artesunate were less than in
tant second drug necessary to prevent resistance. Doxycycline
our study (Table 1). We accept that not all subjects meet
can be used as an alternative in adults.
similar criteria to those published studies, but this study was
The main goal of this study was to evaluate the efficacy and
not intended to show a reduction in mortality as an outcome
safety of an alternative therapy to parenteral quinine in areas
measure, but this was noted, and we comment on it as a
where there is poor access to well-structured health facilities,
such as exist in Sudan and many other parts of the Third
The selection criteriaused the WHO21 definition of severe
World and where patient referral is impractical. A novel dos-
malaria to include hyperparasitemia, jaundice, hyperpyrexia,
age regimen of artesunate rectocaps (200 mg every 8 hours for
cerebral involvement, renal impairment, and prostration, and
3 days) achieved substantial and rapid decreases in parasit-
these were used for selecting patients for the study. Because
emia and fever in patients presenting with severe falciparum
many of these criteria are clinical and subjective, comparison
malaria. The drug regimen was well tolerated and produced a
of disease severity with other studies is difficult. About one
clinical cure in most patients by day 3. The addition of 1 of 3
quarter of all 404 cases diagnosed as P. falciparum (26.7%)
second-line drugs prevented recrudescence of malaria. The
were considered severe, however, and recruited into the
regimen was designed for use in settings with poor resources
study. It is of note that only 1 death occurred, and recovery
and limited expertise, and its ease of use may have a signifi-
occurred in more than three quarters with 3 days of artesu-
cant impact and effectiveness that may reduce complications
nate treatment. Because the formulation was a rectal supposi-
and mortality from falciparum malaria. The sequential com-
binations of artesunate rectocaps followed by doxycycline or
volunteers and patients with uncomplicated falciparum ma-
pyrimethamine/sulfadoxine were equally effective as meflo-
laria. Am J Trop Med Hyg 65: 717–721.
6. Rowland M, Thomas N, 1995. Therapeutic regimens. In Clinical
quine in preventing recrudescence and in this study had a
pharmacokinetics—concepts and applications, 3rd ed. Balti-
100% radical cure rate. The combination regimens seem safe
more: Williams & Wilkins. 83–105.
and highly effective and could be lifesaving in patients with
7. Barradell LB, Fitton A, 1995. Artesunate: A review of its phar-
severe malaria, particularly in rural areas. The present results
macology and therapeutic efficacy in the treatment of malaria.
can be pooled in the future with results from other areas to
8. Hien TT, White NJ. Qinghaosu. Lancet 341: 603–608.
determine the actual efficacy of artesunate suppositories com-
9. Benakis A, Paris M, Loutan L, Plessas CT, Plessas ST, 1996.
pared with current therapeutic options used in different re-
Pharmacokinetic study of a new pharmaceutical form of arte-
sunate (Plasmotrim-200 Rectocaps) administered in healthyvolunteers by rectal route. Jpn J Trop Med Hyg 24: 39–45.
10. Awad MI, Eltayeb IB, Taylor RB (submitted). Pharmacokinetics
Received April 23, 2002. Accepted for publication October 14, 2002.
of artesunate following oral and rectal administration in
Acknowledgments: We deeply thank all the medical staff in Omdur-
man Teaching Hospital and Tropical Disease Hospital, particularly
11. Looareesuwan S, Wilairatana P, Vanijanonta S, Viravan C, An-
Dr. Omer Nemiri, Dr. Fatima A., Dr. Angal Almahdi, and Dr. Amel
drial M, 1995. Efficacy and tolerability of a sequential artesu-
Hajnour, for their assistance and collaboration in carrying out the
nate suppository plus mefloquine in the treatment of severe
clinical trial. We thank Mr Tarig Elfaki, Mr Salah G. Elzaki, Mr.
falciparum malaria. Annu Trop Med Parasitol 89: 469–475.
Mohamed A/gadir, and Mr. Afiefi, for their technical assistance
12. Looareesuwan S, Wilairatana P, Andrial M, 1996. Artesunate
suppository for treatment of severe falciparum malaria inThailand. Jpn J Trop Med Hyg 24: 13–15.
Financial support: This work was supported by the British Chevening
13. Thwe Y, Than M, Phay S, ZawOo A, YuSoe A, 1996. Artesu-
Scholarship, University of Khartoum, Tropical Research Institute,
nate-mefloquine tablets (Plasmotrim Rectocaps, Mefloquine
and Malaria National Administration in Sudan. We thank Mepha
Lactab) in the treatment of severe malaria. Jpn J Trop Med
Pharmaceutical Research, Aesch-Basel, Switzerland, for the donation
14. Eduardo A, Gomez L, 1996. Efficacy of artesunate suppository
The clinical trials were conducted in Khartoum-Sudan. Data inter-
followed by oral mefloquine in the treatment of severe malaria
pretation and writing were undertaken at Robert Gordon University,
in endemic areas where resistance to chloroquine exists in Ec-
United Kingdom, and University of Khartoum, Sudan.
uador. Jpn J Trop Med Hyg 24: 17–24.
15. Bhatt K, Bhatt S, Omonge E, Otekol L, Andrial M, 1996. Efficacy
Authors’ addresses: M. I. Awad and I. B. Eltayeb, Department of
and tolerability of a sequential artesunate suppository-
Pharmacology, Faculty of Pharmacy, University of Khartoum, P.O.
mefloquine treatment of severe review falciparum malaria. Jpn
Box 1996, Khartoum, Sudan. A. M. Y. Alkadru and O. Z. Baraka,
Department of Internal Medicine and Applied Therapeutics, Faculty
16. Halpaap B, Maryse N, Paris M, Benakis A, Peter G, 1998. Plasma
of Medicine, University of Khartoum, P.O. Box 1063, Khartoum,
levels of artesunate and dihydroartemisinin in children with
Sudan. R. H. Behrens, Department of Infectious and Tropical Dis-
plasmodium falciparum malaria in Gabon after administration
eases, London School of Hygiene and Tropical Medicine, Keppel
of 50 milligram artesunate suppositories. Am J Trop Med Hyg
Street, London, UK, Telephone: +44 207 9272661, E-mail:
17. World Health Organization Severe Malaria Task Force, 1997.
Reprint requests: R. H. Behrens, Department of Infectious and
Task force on artesunate suppositories for malaria treatment.
Tropical Diseases, London School of Hygiene and Tropical Medicine,
TDR/UNDP/World Bank/Special Programme for Research
Keppel Street, London, UK, Telephone: +44 207 9272661, E-mail:
and Training in Tropical Diseases. Geneva: World Health Or-
18. World Health Organization Severe Malaria Task Force, 1999. Workplan of the severe malaria Task Force. TDR/UNDP/World Bank/Special Programme for Research and Training inTropical Diseases. Geneva: World Health Organization.
19. Bunnag D, Viravan C, Looareesuwan S, Karbwang J, Harinasuta
1. World Health Organization, 1996. Investing in health research for
T, 1991. Clinical trial of artesunate and artemether in multi-
development. Report of the Ad Hoc Committee on Health Re-
drug resistant falciparum malaria in Thailand: a Preliminary
search Relating to Future Intervention Options. Report No:
report. Southeast Asian J Trop Med Public Health 22: 380–385.
TDR/Gen/96.1. Geneva: World Health Organization.
20. White NJ, Olliaro PL, 1996. Strategies for the prevention of an-
2. Gilles HM, 1991. Introduction. In A practical handbook in the
timalarial drug resistance: rationale for combination chemo-
management of severe and complicated malaria, 2nd ed.
therapy of malaria. Parasitol Today 12: 399–401.
Geneva: World Health Organization. 1–4.
21. World Health Organization, 2000. Severe falciparum malaria.
3. White NJ, Nosten F, Looareesuwan S, White NJ, Nosten F, Looa-
Trans R Soc Trop Med Hyg 94: 1–90.
reesuwan S, Watkins WM, Marsh K, Snow RW, Kokwaro G,
22. Price RN, Nosten F, Luxemburger C, ter Kuile FO, Phaipun L,
OumaJ, Hien TT, Moyneux ME, Taylor TE, Newbold CI,
Chongsuphajaisiddhi T, White NJ, 1996. Effects of artemisinin
Ruebush TK, Danis M, Greenwood BM, Anderson RM, Ol-
derivatives on malaria transmissibility. Lancet 347: 11654–
liaro P, 1999. Averting a malaria disaster. Lancet 353: 1965–
23. Warrell DA, Molyneux ME, Beales PF, 1990. Severe and com-
4. White NJ, 1994. Clinical pharmacokinetics and pharmacodynam-
plicated malaria. Trans R Soc Trop Med Hyg 84: 1–65.
ics of artemisinin derivatives. Trans R Soc Trop Med Hyg 88:
24. Von Seidlein L, Milligan P, Pinder M, Bojang K, Anyalebechi C,
Gosling R, Coleman R, Ude JI, Sadiq A, Duraisingh M, War-
5. Teja-Isavadharm P, Watt G, Eamsila C, Jongsakul K, Li Q, Keer-
hurst D, Alloueche A, Targett G, McAdam K, Greenwood B,
atithakul G, Teja-Isavadharm P, Watt G, Eamsila C, Jongsakul
Walraven G, Olliaro P and Doherty T, 2000. Efficacy of arte-
K, Li Q, Keeratithakul D, Sirisopana N, Luesutthiviboon L,
sunate plus pyrimethamine-sulphadoxine for uncomplicated
Brewer TG, Kyle DE, 2001. Comparative pharmacokinetics
malaria in Gambian children: a double-blind randomised, con-
and effect kinetics of orally. administered artesunate in healthy
trolled trial. Lancet 355: 352–357.
depolarizations, decreased K+ conductance and[6] Gastaut H, Tassinari CA, editors. Handbook of Electro-enhancement of excitatory signals such as Gluta-encephalography and Clinical Neurophysiology, part A, vol. 13. Amsterdam: Elsevier Scientific Publishing Company;mate [12]. Serotonin plays a dual (may be synergis-tic effect) role in increasing susceptibility to[7] Shouse MN, Staba R, Farber
A New Assault on Addiction motivated to take it. "If this drug isn't used with a comprehensive treatment program," Medicine: Can a single drug keep alcoholics on the says DuPont Merck president Kurt Landgraf, “the failure rates are very high." And wagon and help junkies through withdrawal? naltrexone poses hazards of its own. The common side effects are minor, ranging from
 Mean ± SD of the clinical, hematologic, and biochemical parameters at admission of the 3 second-drug treatment groups
Hemoglobin (g/dl) (men, 13–17 g/dl; women, 12–15 g/dl)
Serum creatinine (mg/dl) (0.5–1.5 mg/dl)
Note. Values in parentheses are laboratory normal range.
Mean ± SD of the clinical, hematologic, and biochemical parameters at admission of the 3 second-drug treatment groups
Hemoglobin (g/dl) (men, 13–17 g/dl; women, 12–15 g/dl)
Serum creatinine (mg/dl) (0.5–1.5 mg/dl)
Note. Values in parentheses are laboratory normal range.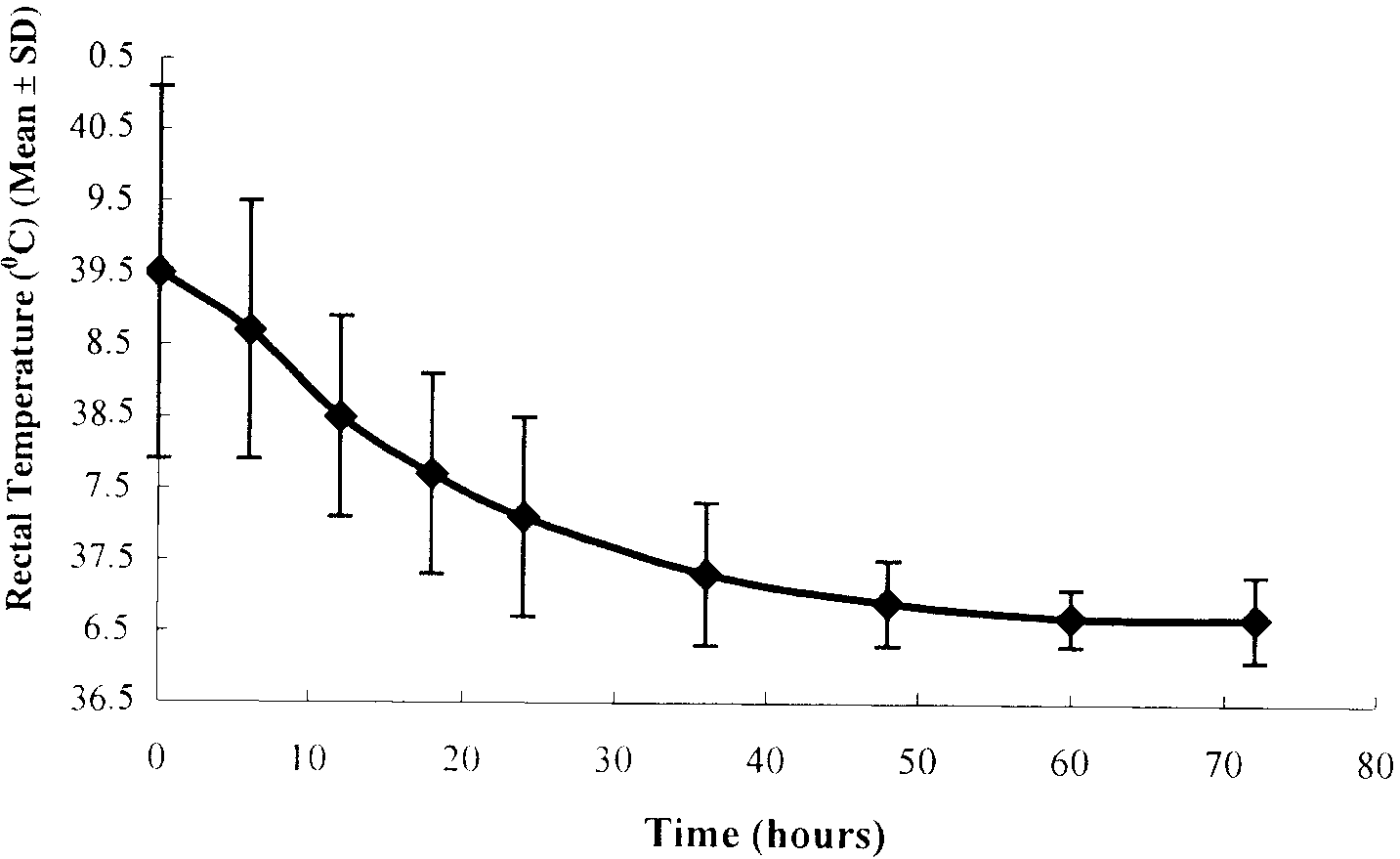 tory, cultural objection to the use of suppositories needed tobe considered. Cultural acceptance is variable and respondsto education. There was little resistance to the use of thesuppositories by patients or their relatives.
tory, cultural objection to the use of suppositories needed tobe considered. Cultural acceptance is variable and respondsto education. There was little resistance to the use of thesuppositories by patients or their relatives.