Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Jtt-12-01-005 1.6
Published online on 21 August 2012 J Telemed Telecare, doi: 10.1258/jtt.2012.120105
Q Evaluation of a telemedical care programme
Frank Marzinzik, Michael Wahl, Christoph M Doletschek,Constanze Jugel, Charlotte Rewitzer and Fabian Klostermann
Department of Neurology, Charite´ - University Medicine Berlin, Germany
SummaryWe reviewed a telemedicine-based care model for drug optimization in Parkinson’s disease. In this model patients sendvideo recordings made in the home to the treating team via the Internet. These serve as the basis for making therapeuticdecisions, in particular drug adjustments. Data from 78 patients were analysed with respect to outcome, methodacceptance and management of the procedure. During the 30-day telemedicine programme, the patients recorded anaverage of 3.2 videos per day. The patients’ motor score on the Unified Parkinson’s Disease Rating Scale (UPDRS) was31 points at enrolment and three months after ICP termination it was significantly lower at 24 points (P , 0.01), i.e. therewas less impairment. The patients rated their condition better at the end than at the beginning of the programme: ona 6-point scale, the mean rating at the beginning was 3.2 and the mean rating at the end was 2.8 (P , 0.001). A blindedinvestigator rated the patients’ videos on the same scale: at the beginning the mean score was 3.0 and at the end itwas 2.8 (P , 0.05). The information from the questionnaire showed overall acceptance and practicability of the method. Both patients’ and neurologists’ use of the method was high. The method seems to be feasible for therapy optimizationin Parkinson’s disease, and of particular interest for patients with complex conditions who do not necessarily have toundergo hospital treatment.
In the integrated care programme for Parkinson’s disease(ICP), outpatient neurologists work together with hospital
Parkinson’s disease (PD) is characterized by the chronic
experts in the evaluation and treatment of PD patients on
progression of various, individually composed motor and
the basis of standardized videos. The recordings are made
non-motor deficits.1 Problems in PD often arise from the
with a camera installed in the patient’s home to capture
drug therapy for the movement disorder. During the early
distinct motor states at several times per day. This provides a
stages, the regular intake of dopaminergic medication
representative picture of individual motor profiles. The
provides good control of motor symptoms and severe
video recordings are automatically sent to the treating team
therapeutic complications are uncommon. However,
via the Internet and serve as the basis for making
5 –10 years after the start of treatment, drug responsiveness
therapeutic decisions, in particular drug adjustments.
usually wears off and about 30% of PD patients develop
Patients are admitted to the ICP by their treating
diurnal fluctuations with increasing hypokinetic and/or
neurologists if they experience fluctuations despite regular
dyskinetic phases. This leads to increased hospital
drug updates and against the background of a previously
stable motor condition. Patients visit the regional clinic for
It is likely that fewer PD patients would require inpatient
ICP where an expert in movement disorders confirms the
treatment if modern communication devices could be used
diagnosis of PD and rates it using the Unified Parkinson’s
in making the necessary therapeutic changes.2,3 In this
Disease Rating Scale (UPDRS), Hoehn & Yahr and
context, a telemedicine-based integrated care programme
neuropsychological scores (for details see Table 1). Patients
for patients with Parkinson’s disease is of interest. The
are taught how to start video sequences and to respond to
programme is reimbursed by a number of public health
the instructions, delivered via a voice system during each
After being admitted to the ICP, a commercial system
provider (MVB – Medizinische Videobeobachtung GmbH)
Correspondence: Fabian Klostermann, Department of Neurology, Charite´ -
installs the necessary equipment in the patient’s home. This
University Medicine Berlin, Campus Benjamin Franklin, 12200 Berlin, Germany(Fax: þ49 30 8445 4264; Email: )
comprises a camera on a tripod, adjusted to capture pictures
Journal of Telemedicine and Telecare 2012: 1 – 6
Copyright 2012 by the Royal Society of Medicine Press
F Marzinzik et al. Telemedicine in Parkinson’s disease
Table 1 Patient data. There were 34 women and 44 men
server via a UMTS connection. From there, copies are sent tothe treating team, comprising the patient’s neurologist and
hospital experts with an advisory role. They are equipped
with software for viewing the videos, which allows the
documentation of patient data and medication changes.
There are also dialogue functions for the exchange of
messages between the hospital team and the neurologist,
and between the neurologist and the patient, e.g. to discuss
or explain medication changes. More details on the
Note: the start LD dose indicates PD drugs, calculated as levodopa equivalence dose, at the
methodology have been published elsewhere.4
beginning of ICP; the end LD dose indicates PD drugs, calculated as levodopa equivalencedose, at the end of ICP
For the 30 days after equipment installation, the
neurologist mainly works with the video sequences which
of the patient walking, a suitable light, loudspeakers for
the patients are asked to record at three scheduled times per
voice instructions to guide the patient through the
day, normally in the morning, early afternoon and evening
recording, a PC, a printer and a transponder with reader, see
(the patients are free to provide additional recordings at any
other time). The neurologist has to confirm that the videos
The patients start each 2-min video sequence by moving
have been reviewed, so that the frequency of inspections
the transponder over the reader. The videos are uniformly
can be traced in the system. In addition, any changes of
structured according to voice announcements about the
medication are stored. The minimum communication from
performance of different motor activities in front of the
the treating neurologist to the patient is a daily printout of
camera (including finger tapping, diadochokinesis, leg
his/her medication plan, be it modified or not.
agility, rising from chair, postural stability, walking). The
At the end of each recording, patients are asked
recordings are stored on the local PC as compressed files
to evaluate their motor state with a mark from 1 to 6
(x-Vid-Codec for MPEG videos) and then transferred to a
(1 ¼ excellent/best to 6 ¼ unacceptable/worst). After thisself-evaluation, the patients report their general conditionand complaints, e.g. non-motor aspects of the disease. Thetreating neurologist makes therapeutic decisions on thebasis of the motor condition, as documented in the videosand the self-evaluation. Continuous drug adjustments takethe individual history of treated symptoms and mentionedcomplaints into account.
Theoretically, the ICP has advantages, such as therapy
involving a team of outpatient and hospital experts,assessment of motor fluctuations based on multiple videosequences or close patient feedback. However, the practicaluse of ICP remains to be settled. We have thereforeexamined the feasibility and efficacy of the new procedure.
A retrospective analysis was performed for 78 consecutivepatients (mean age 67 years SD 8; 44 male, 34 female) whowere routinely included into ICP at the Charite´ from 2008to 2010. The participants were long-term PD patients (9.7years disease duration, SD 0.6), insured by some of themajor health insurance companies. All patients gaveinformed consent to the analysis and anonymouspublication of their data. The study did not require ethicspermission.
In addition to the routine ICP activities, the following
additions were made. Three months after ICP termination, asecond visit to the Charite´ was used to reassess the clinicaland neuropsychological scores and to let the patientsevaluate their own videos (see below). A questionnaire
Figure 1 The PC, transponder unit, camera, printer andloudspeakers
concerning the acceptance and manageability of ICP was
F Marzinzik et al. Telemedicine in Parkinson’s disease
also sent to all patients. This questionnaire contained 14
Table 2 Video recording frequencies by the patients in ICP
Further analyses were conducted on how frequently the
neurologists and their patients made use of the
telemedicine system. With respect to the patients, the
number of individual videos and the daily/nightly hours at
which they were recorded were assessed. Concerning the
treating neurologists, it was determined how many timesduring the 30 days of ICP they reviewed video sequencesand performed medication changes per patient, as
to changes of dopaminergic medication (calculated as
The self-evaluation of the motor state was systematically
assessed at the beginning and at the end of ICP, based onvideos recorded (1) between day 2 and 4, and (2) between
day 27 and 29 of the programme. The first three complete
videos, recorded during morning, afternoon and evening,were selected. For statistical comparisons (see below), the
All of the 78 consecutively enrolled patients terminated ICP
mean rating values belonging to the three videos per
regularly. During the 30 days of the procedure the PD
interval were taken to avoid multiple comparisons per
medication was mostly increased, i.e. the participants
subject and to study daily average states. The three videos
started with dopaminergic drugs, equivalent to 792 mg (SD
should be recorded in one day, ideally at day 2 and,
485) levodopa per day, and terminated ICP with 898 mg (SD
respectively, 27. If, for example in case of poor compliance,
508) (P , 0.01; Wilcoxon signed-rank test). The neurologists
patients did not record the three standard videos during the
reviewed the videos 13.1 times (SD 4.7) and made 5
first day per interval, but during one of the following days,
medication changes (SD 2.9) over the 30 days of ICP.
the earliest available morning, afternoon and evening
The patients recorded 3.2 SD 0.8 videos per day (amounting
recordings were selected per interval.
to an average of 97.1 videos per patient), close to the
For comparison with the self evaluation, the selected 468
required three recordings per day. This recording frequency
videos (6 videos per patient for 78 patients) were further
was almost unchanged over the thirty days of ICP
rated by a blinded expert from the Movement Disorders
(mean video frequency per day in the 1st/2nd/3rd ten-day
Section of the Neurological Department of the Charite´ who
period: 3.3/3.1/3.2). The daily video recording frequencies
was instructed to use the global scoring system of the
are summarized in Table 2. The timing of the video
patients. This investigator was not involved in any of the
treatments and exclusively evaluated the muted sequences
All but one patient returned the questionnaires. The data
of the motor section of each recording to avoid any
indicated overall acceptance and manageability of ICP. For
reference to the patients’ self-evaluation. To rule out bias
example, 92% noted that they were (rather) content with
due to personal attitudes towards ICP, the videos were
the treatment, 77% stated that they would repeat the
presented in randomized order so that it was impossible to
treatment programme and 81% felt that they could convey
know when during ICP recordings were made. Further, on
their symptoms better than in a hospital visit. Ninety-one
the occasion of the visit three months after ICP, all patients
percent stated that they could handle the home camera
viewed and evaluated their own videos (the muted
system on their own. The questions and responses are
sequences, selected and ordered as for the blinded
investigator). In a debriefing after this procedure, the
The patients’ UPDRS motor score at the enrolment visit
patients generally denied noticing when during ICP single
was 31.2 points (SD 8.9) and three months after ICP
termination it was 24.0 points (SD 9.5); lower scores
The results from the questionnaire were analysed
indicate less impairment. The difference was significant
descriptively. Statistical comparisons between the UPDRS
(P , 0.01; Wilcoxon signed-rank test).
pre vs. post ICP and between the ratings at the beginning vs.
During ICP, the patients rated their condition better at the
end of ICP were run with the Wilcoxon signed-rank test.
end than at the beginning of the programme (global scale
Spearman’s rank correlation was calculated between the
from 1 ¼ best to 6 ¼ worst): the mean ratings were 3.2
changes of scores (self vs. external) and effects were referred
(SD 0.8) vs. 2.8 (SD 0.8), P , 0.001. When viewing their own
Table 3 Diurnal distribution of the video recordings. The values indicate the average number of recordings per subject over the 30 days of the ICP,calculated for all 78 patients in the specified intervals per day
F Marzinzik et al. Telemedicine in Parkinson’s disease
Table 4 Frequencies of responses (%) as provided in questionnaires by 77 patients
1 Could you start the camera on your own?
2 Did you need assistance for any of the procedures?
3 Were your complaints captured better than in a hospital stay for PD?
4 Were your complaints captured better than in an ordinary outpatient visit?
6 Would you recommend the therapy to other PD patients?
9 Did the therapy disturb daily routines?
13 Could you explain your symptoms to your doctor?
14 Are you content with the therapeutic steps taken during the procedure?
videos three months after ICP, the patients also evaluated
The significance of the rated improvements was due to
themselves better in the videos from the end than from the
relatively large changes in patients who had benefited from
beginning of ICP (rating at beginning vs. end: 3.4 SD 0.8 vs.
ICP (‘responders’) as opposed to similarly moderate changes
3.1 SD 0.7, P , 0.05). This was also true of the blinded
in patients with negative outcome ratings or no change
investigator (rating at beginning vs. end: 3.0 SD 0.7 vs. 2.8
(‘non-responders’), both according to the patients and
SD 0.7, P , 0.05). Although on average being highest for the
according to the external investigator. Non-responders were
patients during ICP, the rated change of initial vs. end
approximately as frequent as responders with 38/51/50%
ICP condition did not significantly differ, whether
non-responders (unchanged: 17/18/18%, worsened: 21/33/
performed by the blinded investigator or by the patients, be
32%) and 62 /49 /50% responders due to the patients in/
it during or after the programme. Furthermore, the change
after ICP/the blinded investigator. The distribution of
rated by the patients during ICP was moderately correlated
rated changes of initial versus end ICP conditions is
with the respective changes, as rated by the patients
shown in Figure 4 separately for non-responders and
after ICP (r ¼ 0.5, P , 0.01) and by the blinded investigator
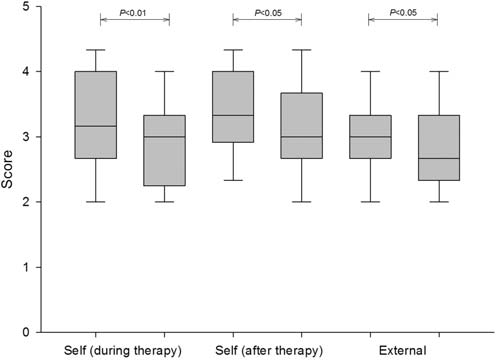
(r ¼ 0.6, P , 0.01; Figure 2). The distribution of the ratings
Differences between responders and non-responders
from the beginning versus the end of the programme is
appeared to prevail with respect to baseline medication and
shown in Figure 3 for the patients during/after ICP and for
medication change throughout ICP. According to the
Figure 3 Self-ratings by the patients during and after ICP, and theratings by the blinded investigator (external) on a scale from1 (best) to 6 (worst). The ratings were made from three recordings
Figure 2 Changes in the self-rated patient scores (abscissa) and the
at an early and a late ICP phase. (Early interval ¼ day 2 –4; late
scores of the blinded investigator (ordinate). The ratings were made
interval ¼ day 27 –29). In the box plots, the boundary of the box
from three recordings at an early and a late ICP phase. (Early
closest to zero indicates the 25th percentile, a line within the
interval ¼ day 2– 4; late interval ¼ day 27– 29). Thus negative values
box marks the median, and the boundary of the box farthest from
indicate worsening and positive values indicate improvement
zero indicates the 75th percentile. The whiskers (error bars) above
throughout the programme. These values were weakly correlated
and below the box indicate the 90th and 10th percentiles
F Marzinzik et al. Telemedicine in Parkinson’s disease
identified with respect to parameters indicating the use ofthe system, i.e. patients belonging to either group recordeda similar number of videos and were reviewed and,respectively, drug-adjusted with similar frequencies by theirneurologists.
Although it was a new treatment modality for the patients,ICP was well accepted and the procedure was mostly notconsidered as especially demanding. The patients’adherence to the recording schedule for the videos and
Figure 4 Changes in the self-ratings by the patients during and after
the neurologists’ usage of the system were generally high.
ICP, and the ratings by the blinded investigator (external) on a scale
During ICP, patients evaluated their motor state better at
from 1 (best) to 6 (worst). The changes are shown separately for
the end than at the beginning of the programme. This
patients who at the end of the programme were evaluated better
improvement was in line with the assessment of the
than at its beginning (i.e. ‘responders’, positive values) versus thosewho were unchanged or worse (i.e. ‘non-responders’, negative
external investigator, and also with the follow-up ratings of
values). Note that non-responders were almost as frequent as
the patients who evaluated their own videos three months
responders. Box plot attributes as for Figure 3
Advantages of telemedicine-based health care models
patients after ICP/the blinded investigator, the difference of
have been demonstrated in a number of medical contexts,
the initial and end levodopa equivalence dose was only
but similar data in the field of PD are scarce. In
significant in the responder group (dose increases: 122 SD
neurovascular medicine, remote telemedical expert support
262 mg/145 SD 231 mg, both P , 0.01), but not in
has been shown to improve the outcome of stroke patients
non-responders (dose increases: 80 SD 301 mg/56 SD
in non-specialized community hospitals at similar cost.5
322 mg, P . 0.1). Further, the initial levodopa equivalence
With respect to PD, travelling to remote expert units was
dose was lower in the responders (673 SD 487 mg) than in
reduced through the use of videoconferencing systems with
the non-responders (930 SD 467 mg; P , 0.05) according to
which disease-related dysfunctions were reliably
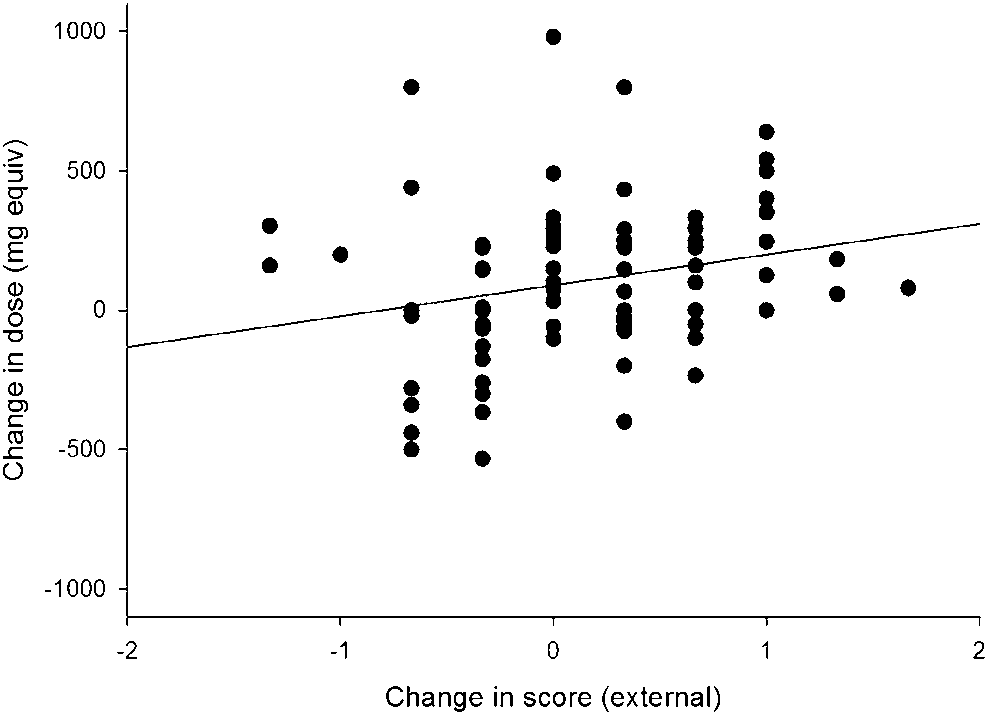
the blinded investigator. The change of the levodopa
assessed.2,3,6 –8 Furthermore, in a recent study with ten PD
equivalence dose throughout ICP was very weakly
patients under telemedical care, quality of life and motor
correlated with the rating change of the external
outcome measures were enhanced compared to a control
investigator (r ¼ 0.25, P , 0.04, Figure 5). No significant
differences between the groups (whether due to the patients
The value of telemedicine as an element of routine care in
in and after ICP or to the blinded investigator) were
PD has not been investigated previously. Most motorsymptoms of PD are visually discernible, so that videorecordings can provide relevant and retrievable informationfor treatment decisions. Once fluctuations have occurred, aconsistent schedule of recordings can convey the dynamicsof motor instability as an essential requirement of rationaldrug adaptations. Other than in regular outpatient settingsin which patients are normally seen at intervals of a fewmonths, evaluations in ICP are so frequent that functionalchanges per day can be quantified, and control of thepatients’ participation is easier than by use of alternativetechniques such as symptom diaries.10
In the present case, the neurologists surveyed the videos
for each patient on average 13 times per month. Thus, givennormal intervals of 2 –3 days between single review dates,6 –9 videos were available for any interim analysis of apatient, who mostly complied with the ICP default of threerecordings per day. In this regard, ICP combines a number
Figure 5 Changes in the evaluation scores from beginning to end of
of advantages of hospital treatment, such as frequent
the programme of the blinded investigator (abscissa) and the
medical assessments and close patient feedback, with
corresponding changes in the levodopa (LD) equivalence dose
features of outpatient care, e.g. continuity of personal
(ordinate) from the beginning compared to the end of theprogramme. These values were weakly correlated
treatment in a normal environment. Furthermore,
F Marzinzik et al. Telemedicine in Parkinson’s disease
treatment decisions can also refer to patient information,
extended, but less frequent monitoring, thus broadening
recorded at times during which regular expert monitoring is
the repertoire of ICP-treatable conditions and, possibly,
unavailable under normal hospital or ambulant conditions.
closing the gaps between classical in- and outpatient care. It
In the present study, patients who profited from the
is regrettable that most public insurers require an a-priori
method appeared to differ from non-responders in terms of
superiority or non-inferiority proof of ICP compared to PD
the augmentation of PD medication during the programme.
hospital therapy (for which efficacy data are not available),
Accordingly, one might ask if a better outcome was due to
although ICP might avoid many ‘habitual’ hospital
the fact of initially underdosed medication which could
admissions, given a complementary use of this and
have been adjusted in ambulant settings just as well.
However, this probably oversimplifies the complex
In conclusion, the data from the present study are
problems of PD drug treatment. Inclusion into ICP required
encouraging for ICP. The method seems to be feasible for
that the patient’s neurologist had noted a disproportionate
therapy optimization in PD, and of particular interest for
deterioration of a previously stable motor condition despite
patients with complex conditions who do not necessarily
regular drug updates. Of course, in this context it may be
have to undergo hospital treatment. Future healthcare
noted that cautious drug handling under outpatient
studies might address which patients will profit most from
conditions is comprehensible, given the numerous
ICP and how efficient it is in comparison to inpatient
neuropsychiatric and vegetative side effects of
dopaminergic medication, particularly relevant in advancedpatients. But even if many physicians performed an
inappropriately ‘sparing’ treatment (rather than aiming at
made equal contributions to the work.
maximum symptom control), ICP would have correctedthis tendency, e.g. by extending the therapeutic team byhospital experts. Here, future studies might systematically
analyse the patients’ neuropsychiatric condition, specificdrug effects, the adjustment of administration schedules
1 Poewe WH, Wenning GK. The natural history of Parkinson’s disease. Ann
and even treatment attitudes of the neurologists to provide
2 Biglan KM, Voss TS, Deuel LM, et al. Telemedicine for the care of nursing
potentially relevant data for healthcare research in the field
home residents with Parkinson’s disease. Mov Disord 2009;24:1073 – 6
3 Hubble JP, Pahwa R, Michalek DK, Thomas C, Koller WC. Interactive
With respect to the self and external evaluations, patients
video conferencing: a means of providing interim care to Parkinson’sdisease patients. Mov Disord 1993;8:380 – 2
rated their improvement about twice as high as the blinded
4 Biemer M, Hampe JF. A mobile medical monitoring system: concept,
investigator. This could reflect a placebo effect. On the other
design and deployment. Proceedings of the International Conference on
hand, the higher improvement could be due to subjectively
5 Audebert HJ, Schenkel J, Heuschmann PU, et al. Effects of the
perceived changes undetectable in the muted video
implementation of a telemedical stroke network: the Telemedic Pilot
sequences for the post-ICP ratings, e.g. relying on off-pain
Project for Integrative Stroke Care (TEMPiS) in Bavaria, Germany. Lancet
relief or benefit from antidepressive treatment.11,12 This
6 Hoffmann T, Russell T, Thompson L, Vincent A, Nelson M. Using the
might also explain why the patients’ overall appraisal of the
Internet to assess activities of daily living and hand function in people
value from ICP, as provided in the questionnaire, appeared
with Parkinson’s disease. NeuroRehabilitation 2008;23:253 – 61
relatively high compared to the postprocedural rating of
7 Samii A, Ryan-Dykes P, Tsukuda RA, Zink C, Franks R, Nichol WP.
Telemedicine for delivery of health care in Parkinson’s disease. J Telemed
motor benefit. Finally, the results from the UPDRS
assessments before versus three months after ICP seem to
8 Adam OR, Ferrara JM, Aguilar Tabora LG, Nashatizadeh MM, Negoita M,
point to a sustained motor improvement after ICP, but these
Jankovic J. Education research: patient telephone calls in a movementdisorders center: lessons in physician-trainee education. Neurology
data were mainly from a neurologist who belonged to the
hospital ICP team and may have been biased.
9 Dorsey ER, Deuel LM, Voss TS, et al. Increasing access to specialty care: a
Weaknesses of ICP include the limitation of the
pilot, randomized controlled trial of telemedicine for Parkinson’s disease. Mov Disord 2010;25:1652 – 9
programme to 30 days and the emphasis on the treatment
10 Stone AA, Shiffman S, Schwartz JE, Broderick JE, Hufford MR. Patient
of PD motor symptoms. For example, diagnosis and
non-compliance with paper diaries. BMJ 2002;324:1193 – 4
treatment of common neuropsychiatric problems in PD
11 Tolosa E, Compta Y. Dystonia in Parkinson’s disease. J Neurol
could be realised, if the 30 monitoring days were used at
12 Schrag A. Quality of life and depression in Parkinson’s disease. J Neurol Sci
individualised intervals. Such flexibility would allow
MESSA’s new MESSA Saver Rx drug program is designed to help MESSA members save money and stay healthy by providing discounted copayments on more than a hundred maintenance drugs prescribed for chronic conditions. MESSA Saver Rx will also reduce health care costs over the long term for our members and for their MESSA health plans by providing lower copayments for prescription dru
Bayerischer Landtag 16. Wahlperiode Drucksache 16/ 15931 Begründung: Die Pille danach auf der Basis von Levonorgestrel wird inzwi-der Abgeordneten Margarete Bause, Dr. Martin Runge, schen weltweit als Notfallkontrazeptivum in solchen Fällen ange- Ulrike Gote, Claudia Stamm, Theresa Schopper, Renate wandt, in denen eine andere Verhütungsmethode im Ausnahmefall Ackermann, T
 F Marzinzik et al. Telemedicine in Parkinson’s disease
Table 1 Patient data. There were 34 women and 44 men
server via a UMTS connection. From there, copies are sent tothe treating team, comprising the patient’s neurologist and
hospital experts with an advisory role. They are equipped
with software for viewing the videos, which allows the
documentation of patient data and medication changes.
F Marzinzik et al. Telemedicine in Parkinson’s disease
Table 1 Patient data. There were 34 women and 44 men
server via a UMTS connection. From there, copies are sent tothe treating team, comprising the patient’s neurologist and
hospital experts with an advisory role. They are equipped
with software for viewing the videos, which allows the
documentation of patient data and medication changes.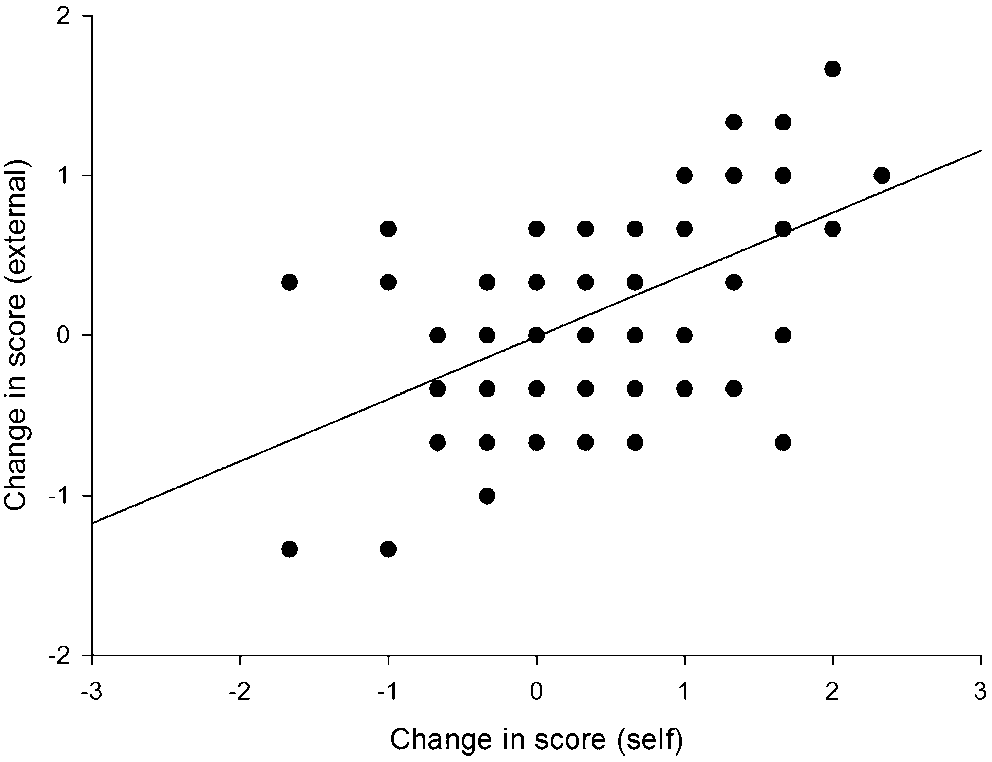
 F Marzinzik et al. Telemedicine in Parkinson’s disease
Table 4 Frequencies of responses (%) as provided in questionnaires by 77 patients
1 Could you start the camera on your own?
2 Did you need assistance for any of the procedures?
3 Were your complaints captured better than in a hospital stay for PD?
4 Were your complaints captured better than in an ordinary outpatient visit?
6 Would you recommend the therapy to other PD patients?
9 Did the therapy disturb daily routines?
13 Could you explain your symptoms to your doctor?
14 Are you content with the therapeutic steps taken during the procedure?
videos three months after ICP, the patients also evaluated
The significance of the rated improvements was due to
themselves better in the videos from the end than from the
relatively large changes in patients who had benefited from
beginning of ICP (rating at beginning vs. end: 3.4 SD 0.8 vs.
F Marzinzik et al. Telemedicine in Parkinson’s disease
Table 4 Frequencies of responses (%) as provided in questionnaires by 77 patients
1 Could you start the camera on your own?
2 Did you need assistance for any of the procedures?
3 Were your complaints captured better than in a hospital stay for PD?
4 Were your complaints captured better than in an ordinary outpatient visit?
6 Would you recommend the therapy to other PD patients?
9 Did the therapy disturb daily routines?
13 Could you explain your symptoms to your doctor?
14 Are you content with the therapeutic steps taken during the procedure?
videos three months after ICP, the patients also evaluated
The significance of the rated improvements was due to
themselves better in the videos from the end than from the
relatively large changes in patients who had benefited from
beginning of ICP (rating at beginning vs. end: 3.4 SD 0.8 vs.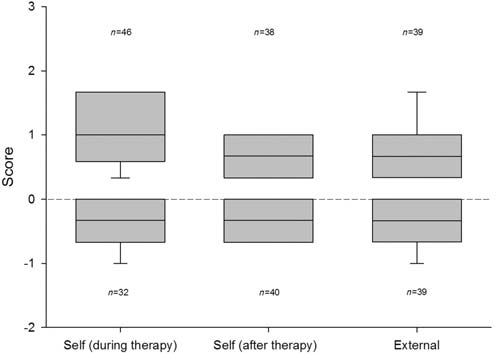
 F Marzinzik et al. Telemedicine in Parkinson’s disease
identified with respect to parameters indicating the use ofthe system, i.e. patients belonging to either group recordeda similar number of videos and were reviewed and,respectively, drug-adjusted with similar frequencies by theirneurologists.
F Marzinzik et al. Telemedicine in Parkinson’s disease
identified with respect to parameters indicating the use ofthe system, i.e. patients belonging to either group recordeda similar number of videos and were reviewed and,respectively, drug-adjusted with similar frequencies by theirneurologists.