Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Nbheart.org
Journal of Human Hypertension (2009) 23, 188–195
& 2009 Macmillan Publishers Limited All rights reserved 0950-9240/09 $32.00
Rationale and design of the KYOTOHEART study: effects of valsartan onmorbidity and mortality in uncontrolledhypertensive patients with high risk ofcardiovascular events
T Sawada1, T Takahashi1, H Yamada1, B Dahlo¨f2 and H Matsubara1, for the KYOTO HEART
Study Group1Department of Cardiovascular Medicine, Kyoto Prefectural University School of Medicine, Kyoto, Japan and2Department of Medicine, Sahlgrenska University Hospital/O¨stra, Go¨teborg, Sweden
It remains to be determined whether the evidence in
treatment with valsartan or conventional non-angioten-
Western countries for blockade of the renin–angiotensin
sin receptor blocker therapies, and the follow-up
System in cardiovascular diseases could be directly
period will be at least 3 years. The primary end point is
applied to East Asian races including the Japanese
a composite of defined cardio- or cerebro-vascular
population as a long-term strategy. The KYOTO HEART
events. Secondary end points include all causes of
Study (KHS) is designed to investigate the add-on effect
mortality, worsening of cardiac function, new onset or
of valsartan versus conventional anti-hypertensive
worsening of arrhythmias or diabetes mellitus. The KHS
treatment on cardiovascular morbidity and mortality in
will provide new evidence for the management of blood
Japanese hypertensive patients with uncontrolled blood
pressure in hypertensive patients with high risk.
pressure and with high cardiovascular risk. Over 3000
Journal of Human Hypertension (2009) 23, 188–195;
high-risk Japanese patients with uncontrolled hyperten-
doi:10.1038/jhh.2008.116; published online 18 September
sion were randomised to receive either additional
Keywords: metabolic syndrome; high risk; angiotensin receptor blockers; cardiovascular mortality and morbidity;valsartan
arrhythmias and sudden cardiac death. The eventrates of cardiovascular disease in Japan differ from
Hypertension is the most prevalent cardiovascular
those in Europe and the United States. Mortality
disease in the world and a major public health
from CAD in Japan is one-third of that in the United
issue.1 Cardiovascular disease is the leading cause of
States, and mortality from cerebrovascular disease
mortality worldwide2 and is expected to increase
in Japan is B1.5 times higher than that in the United
with the general ageing of the world’s population.
States.3 Hypertension is the most common cause of
The goal of anti-hypertensive therapy is to reduce
CAD and heart failure in Japan, and cerebrovascular
the incidence of blood pressure-related morbid
disease is even more prevalent in the Japanese
events and cardiovascular mortality.
population than in Western societies.4 The percen-
The heart is an important target organ of hyper-
tage of cerebral bleeding is two or three times greater
tension. Continuous high blood pressure is asso-
than in Caucasian people in Europe and in the
United States, and cerebral infarction is mostly
increases the burden of coronary artery disease
caused by lacunar type ischaemic stroke owing to
(CAD). These forms of damage may result in
hypertensive small vessel disease.5 The incidence of
athero-thrombotic infarction or cardio-embolic in-farction is currently increasing in Japan, and the
Correspondence: Dr T Sawada, Department of Cardiovascular
dominant pathogenetic factor for stroke is changing
Medicine, Kyoto Prefectural University School of Medicine,
from small arterial disease to large arterial disease in
Kajiicho 465, Kamigyoku, Kyoto 602-8566, Japan.
Japanese hypertensive patients. These differences
may be partly explained by differences in the
Received 4 June 2008; revised 1 August 2008; accepted 18 August2008; published online 18 September 2008
lifestyle of Japanese and Western populations,
which are reflected in body mass index (mean BMI:
pressure control, on major cardiovascular events
23–25 and 28–30 kg/m2, respectively).6,7 Most of
and in particular the incidences of stroke, heart
mortality–morbidity trials have been carried out in
failure and coronary artery events. In contrast, the
Western country, in which none or only a minority
Candesartan Antihypertensive Survival Evaluation
of East Asian patients were included. Owing to the
in Japan (CASE-J) anti-hypertensive study reported
paucity of large-scale trials in East Asian people,
that candesartan-based and amlodipine-based regi-
it remains to be determined whether the results from
mens produced no statistical differences between
similar clinical trials in Western societies are
therapies on stroke or cardiovascular events in high-
internationally applicable to East Asian races or
risk Japanese hypertensive patients.17 The KYOTO
the Japanese population, or whether genetic back-
HEART Study (KHS) will be important to solve this
ground can cause different pharmacokinetic and
pharmacodynamic responses to the same drug.
A new guideline on metabolic syndrome has
The renin–angiotensin system (RAS) has a major
been introduced very recently in Japan. When the
physiological function in the homoeostasis of
patients have hypertension, the definition of meta-
blood pressure, electrolytes and fluid balance, and
bolic syndrome is made from abdominal obesity
circulatory blood volume.8 However, chronic activa-
plus either dyslipidemia or glucose intolerance, or
tion of RAS contributes to the development of
both. Nevertheless, it remains to be determined
hypertension or cardiovascular target organ damage,
how ARBs affect cardiovascular morbid events and
ultimately leading to the manifestation of cardio-
mortality in hypertensive patients with metabolic
vascular disease.9 Numerous trials have investigated
syndrome. The KHS was also designed to examine
the benefits of angiotensin-converting enzyme
whether valsartan added to conventional anti-
(ACE) inhibitors; the Heart Outcomes Prevention
hypertensive treatment influences the cardiovascu-
Evaluation Study reported that ACE inhibitors
lar events in the hypertensive patients with the
significantly reduced the rates of death, myocardial
metabolic syndrome as well as how it improves the
infarction and stroke in high-risk patients.10 The
morbidity and mortality in other high-risk Japanese
beneficial effect observed was probably in some part
patients with uncontrolled hypertension.
independent of ramipril-mediated blood pressurelowering actions, and the direct participation ofRAS in cardiovascular events was strongly sug-
gested. Another important study investigating the
benefit of RAS-blockade in hypertension, in this
The KHS is a multi-centre (31 hospitals), Prospec-
case with an angiotensin receptor blocker (ARB),
tive, Randomised, Open-labeled, Blinded Endpoints
was the Losartan Intervention For Endpoint reduc-
(PROBE),18 two-arm parallel treatment group com-
tion in hypertension study, where losartan-based
parison with a response-dependent dose titration
anti-hypertensive therapy prevented more cardio-
vascular morbidity and death, and in particularstroke, than an atenolol-based regimen despitesimilar blood pressure control.11 The anti-inflam-
matory properties of ARBs have been reported in
The objective of KHS is to assess the add-on effect of
hypertensive patients,12,13 which may contribute to
valsartan, an ARB, on top of conventional anti-
the beneficial action of ARBs beside the anti-
hypertensive treatment in uncontrolled hyperten-
hypertensive effects. Very recently, it was shown
sive patients with cardiovascular disease or at least
that the ARB telmisartan is equivalent to ramipril in
one additional risk factor indicating high-risk with
preventing vascular events in patients with cardio-
respect to cardiovascular morbidity and mortality,
vascular diseases or high-risk diabetes.14 It is beyond
compared with titration by non-ARB therapy.
the scope of this introduction to review all thestudies showing beneficial effects on cardiovascularoutcomes from blocking the RAS, in particular with
ARBs, in various stages of the cardiovascular
The eligible population consists of Japanese hyper-
continuum.15 It is important though to point out
tensive patients (men and women, X20 years old)
that all these studies with a few exceptions have
whose blood pressures have been uncontrolled for
included at maximum a few percentage of Asian
at least 4 weeks. Uncontrolled hypertension was
patients in general and very few Japanese patients in
defined as a mean sitting systolic blood pressure
X140 mm Hg, and/or a mean sitting diastolic blood
The Jikei Heart Study was designed to examine
pressure X90 mm Hg in the outpatient clinic.
whether the addition of valsartan to conventional
Skilled physicians took standard blood pressure
cardiovascular treatment is effective in Japanese
measurements with patients at rest (5–10 min) in the
hypertensive patients with cardiovascular diseases
sitting position with a validated mercury sphygmo-
manometer in accordance with the guidelines
The JIKEI Heart study demonstrated a preventive
proposed by the Japanese Society of Hypertension.19
action of valsartan, added to excellent blood
The mean of X3 consecutive blood pressure
Journal of Human Hypertension
measurements was calculated and recorded. The
(11) patients who were unwilling or unable to
timing of blood pressure measurement was not
constant in relation to patients’ intake of medica-tion. When patients were already treated for hyper-tension, anti-hypertensive drugs other than ARB
were administered for the first 4 weeks and then if
The protocol was approved by the Ethics Committee
still uncontrolled (X140/90), they were considered
at each participating centre. At the first clinic visit,
as candidates for the study. Uncontrolled hyperten-
the trial objectives, study design, and the risks and
sive patients treated with ACE inhibitors before
benefits of study participation were explained care-
randomisation could also participate in this study.
fully to each patient, and subsequently written and
Uncontrolled hypertensive patients who had been
signed informed consent was obtained.
treated with ARB, but were not treated with ARBwithin 4 weeks before randomisation, could parti-cipate in this study.
When these uncontrolled hypertensive patients
The titration schedule of the study is shown in
had at least one of CAD signs (angina pectoris
Figure 1. After confirming the eligibility for patient’s
or a history of myocardial infarction 46 months
enrolment into this study, patients were randomised
before the screening), cerebrovascular diseases
in accordance with the minimisation method,21
(a history of stroke or transient ischaemic attack
which consisted of eight factors (age, gender,
46 months before the screening), or peripheral
dyslipidemia, diabetes mellitus, smoking, obesity,
arterial occlusive disease (previous limb bypass
history of CAD and/or cerebrovascular disease and
surgery or angioplasty, limb ulcer/gangrene or
history of congestive heart failure), either to the
intermittent claudication with ankle/brachial blood
valsartan add-on group or to the conventional add-
pressure index o0.8), and/or one or more of the
on treatment group. For the valsartan add-on group,
cardiovascular risk factors mentioned below, they
valsartan 80 mg once daily was administered in the
were randomised into the trial. The cardiovascular
morning to the patient as an initial dose and flexibly
risk factors included type II diabetes mellitus
adjusted to a dose of 40–80 mg per day as needed to
(defined as fasting plasma glucose X126 mg per
control blood pressure. The dose of valsartan was
100 ml, causal blood glucose X200 mg per 100 ml,
doubled after 4 weeks if the initial dose did not
glycosylated hemoglobin (HbA1c) X6.5%, and/or
achieve the target blood pressure of less than
plasma glucose 2 h after 75 g glucose load X200 mg
140 mm Hg for systolic blood pressure and 90 mm Hg
per 100 ml or current treatment with anti-diabetic
agents), current smoking, lipid metabolism abnorm-
patients with diabetes or renal disease, target blood
ality (defined as low-density lipoprotein cholesterol
pressure was set to less than 130 mm Hg for systolic
X140 mg per 100 ml, and/or triglyceride X150 mg
blood pressure and 80 mm Hg for diastolic blood
per 100 ml or current treatment with anti-dyslipide-
pressure.) After 8 weeks an additional administra-
mia agents), obesity (defined as body mass index
tion of other anti-hypertensive drugs with flexible
dosing regimen other than ARB and ACE inhibitors
defined by the electrocardiogram (ECG), centrally
was allowed if necessary. In contrast, for the con-
ventional treatment group, the conventional treat-ment with anti-hypertensive drugs other than ARBand ACE inhibitors were provided for the patients to
reach the common goal of blood pressure control.
The exclusion criteria were set as follows: (1)
Periodical follow-up was implemented every 6
malignant or secondary hypertension; (2) pregnant
months after setting the sustainable dose.
women or women of childbearing potential; (3)
Randomisation was automatically executed by the
history of worsening heart failure, unstable angina,
host computer and all the data recorded at each
myocardial infarction, percutaneous coronary inter-
centre was managed centrally at the independent
vention (PCI) or coronary artery bypass grafting
data centre in Kobe, Japan. Randomisation and
(CABG) within the preceding 6 months; (4) arrhyth-
data management were managed by the wide area
mia needing to be treated or accompanied with
symptoms including second or third degree atrio-ventricular block; (5) renal impairment (serumcreatinine level 43.0 mg per 100 ml); (6) hepatic
impairment (hepatic failure, cirrhosis, etc.); (7)
Background data such as sex, age, height, body
history of cerebral infarction, cerebral haemorrhage
weight, signs and symptoms, and risk factors were
or transient ischaemic attack within the past 6
recorded during the enrolment period. The follow-
months; (8) allergy of potential clinical concern;
ing general clinical laboratory tests were carried out
(9) electrolyte abnormality (remarkable change in
at baseline and every 6 months. (1) Urinalysis
sodium or potassium); (10) history of malignant
(proteinuria and urinary occult blood); (2) blood
tumour including leukaemia and lymphoma; and
chemistry tests (serum creatinine, Na, K, triglyceride,
Journal of Human Hypertension
Figure 1 Titration schedule for the KYOTO HEART Study.
low-density lipoprotein cholesterol, high-density
infarction (ECG-change and biomarkers for myo-
lipoprotein cholesterol, fasting blood sugar, HbA1C,
cardial infarction), new occurrence or exacerbation
uric acid, blood urea nitrogen, and white blood cell
of heart failure (clinical symptoms including dys-
count; (3) ECG central reading in a core laboratory in
pnoea, shortness of breath and peripheral oedema,
Kyoto Prefectural University Hospital; (4) echocar-
diogram (examined every year, left ventricular
echocardiography according to the guidelines of
diastolic dimension, left ventricular systolic dimen-
the American Heart Association and American
sion, ejection fraction, functional shortening, inter-
College of Cardiology (AHA/ACC), new occurrence
ventricular septum, posterior wall, isovolumic
or exacerbation of angina pectoris (ECG changes
relaxation time, the ratio of early ventricular filling
(E) to atrial contraction (A) velocity, deceleration
guidelines), dissecting aneurysm of the aorta (diag-
time, and left ventricular weight;22 and (5) chest X-
nosed by imaging technique), lower limb arterial
ray (cardiothoracic ratio). In addition, the brain
obstruction (ankle brachial pressure index and
natriuretic peptide (BNP) and aldosterone levels
imaging technique), emergency thrombosis, transi-
were measured in patients related to the progression
tion to dialysis or doubling of serum creatinine
of cardiovascular diseases every year. The oral
levels. The first of these to occur in a specific patient
glucose tolerance test (OGTT) was implemented in
was classified as an event and to be counted as the
patients showing the impaired fasting glucose
primary end point. The following were set as the
stage (110p fasting glucose level o126 mg per
secondary end points: all causes of mortality,
100 ml), and the patients who had impaired glucose
worsening of cardiac function (clinical symptoms
tolerance (IGT: 140p glucose level 2 h after OGTT
together with left ventricular dysfunction by echo-
o200) was checked by OGTT test every year.
cardiography), new occurrence or exacerbation of
Additional Holter ECG measurements were imple-
arrhythmias (diagnosed by Holter ECG), new occur-
mented every year in patients who were already
rence or exacerbation of diabetes mellitus or
diagnosed by Holter ECG to have paroxysmal atrial
impaired glucose tolerance (according to the guide-
lines of American Diabetes Association), or uncon-trolled blood pressure. Any component of compositeprimary end point for which a patient could be
counted once in each category was treated as a
The primary end point was a composite of cardio-
secondary end point. Data from any cause was also
and cerebro-vascular events. Components of the
designated a second end point. The end points
end point include the following: stroke (diagnosed
reported will be reviewed and settled by the
by imaging technique), new or recurrent transient
independent Endpoint Committee. The study was
ischaemic attack (neurological deficit persisting for
registered at http://clinicaltrials.gov/ with the iden-
less than 24 h), new or recurrent acute myocardial
Journal of Human Hypertension
sound echocardiogram, and the efficacy of valsartan
On the basis of results of large end point studies
with/without diabetes and with/without metabolic
patients, the number of patients to be enroled wascalculated as 3000 (1500 in each group) to validatethe hypothesis under the assumption that the
valsartan add-on group achieves a 20% risk reduc-
Recruitment began in January 2004 and follow-up is
tion compared with the conventional treatment
calculated to go on until 2010 or to a time point
group and gives 80% statistical power for detecting
when the pre-determined number of patients with a
clinically significant between-group differences
primary end point has been reached, unless there is
with a two tailed 5% statistical significant level.
a decision for discontinuation of this trial ratified by
Very limited epidemiological data about cardio-
the Steering Committee by recommendation from
vascular risk profiles in Japan are available.
the Data and Safety Monitoring Board.
Information about the prognosis of patients treatedby specialist doctors at specialised hospitals is
particularly scarce. Although the cardiovascularevent rate in the Japanese population is low, the
Earlier large-scaled clinical trials were mainly
hospitals participating in this study undertake the
targeted for white and black races, and only a few
tertiary care of cardiovascular disease; therefore,
studies reported the morbidity and mortality of anti-
they treat more severely ill patients than those seen
hypertensive treatment for East Asian races. Japan is
in other hospitals. On the basis of the prevalence of
one among the countries where people live the
cardiovascular disease in the Japanese cohort,4
longest in the world, and the average life span is 79
it was estimated that the 3-year event rate for
years in men and 85.8 years in women in 2007, and
cardiac mortality and morbidity for patients with
these values are increasing. The incidence of stroke
was relatively higher than that of CAD in Japanese
approximately 12%. The findings of a retrospective
hypertensive patients. The percentage of cerebral
investigation of few patients under treatment at the
bleeding was two or three times greater than in
participating sites were almost identical to this
Europe and the United States, and cerebral infarc-
estimate. However, as this study was end point-
tion was mostly caused by lacunar-type ischaemic
driven, the duration of the study was determined by
strokes owing to hypertensive small vessel disease.5
the accumulated number of patients with a primary
Differences in genetic inheritance among the
races, life-style, public health insurance and free
Analyses will also be made by an independent
access system to hospitals might contribute to the
Statistical Analysis Organization based on the
excellent longevity in Japan. However, the ratio of
intention-to-treat approach and time to first event
the elderly will reach one-fourth of the population
in accordance with the principle of harmonised
in 2020, and the fatty food intake, obesity and high
tripartite guideline ‘Statistical Principles for Clin-
rate of smoking have been increasing the incidence
ical Trials’ developed by International Conference
of high-risk hypertension. Although a new guideline
on Harmonisation (ICH). All randomised patients
on metabolic syndrome has been introduced very
were included in the analysis. Patient characteris-
recently, few studies have reported whether ARBs
tics, corresponding to data characteristics, were
checked for uniform distribution among the various
mortality in hypertensive patients with metabolic
groups. Cox’s proportional hazard regression analy-
syndrome. When patients have hypertension, the
sis was used for comparing the event rate between
definition of metabolic syndrome is made when the
patients also have abdominal obesity plus eitherdyslipidemia or glucose intolerance, or both. TheKHS is a clinical trial designed from PROBE and
wide area network, and is first designed to evaluate
Clinical trials evaluate treatment effects predefined
whether the addition of valsartan to conventional
as primary and secondary end points in the study
anti-hypertensive treatment to improve blood pres-
design. However, post-hoc subgroup analyses are
sure control influences the cardiovascular outcome
frequently added for the reason of the study out-
in Japanese high-risk hypertensive patients with or
without metabolic syndrome. This study will also
Recently, guidelines for reporting subgroup analysis
have the power to address the additional benefits of
have been reported.23 In the KHS, the subgroup
valsartan, which are not related to blood pressure
analysis committee also indicated the detailed
lowering effects. The KHS is expected to provide
planning in the primary end point report; the sub-
benefits beyond the anti-hypertensive effects of
analyses were deliberately planned for cardiovas-
ARBs for hypertensive patients in East Asia with
cular events compared with the number of risk
metabolic syndrome or high-risk. The KHS will
factors, the achievement rate of blood pressure
furthermore settle the issue whether the discrepancy
control, systolic/diastolic parameters using ultra-
between the outcomes of the JIKEI Heart and CASE-J
Journal of Human Hypertension
studies is related to molecule specific differences
11 Dahlo¨f B, Devereux RB, Kjeldsen SE, Julius S,
between ARBs or related to different study designs.
Beevers G, de Faire U et al. Cardiovascular morbidity
The study is ongoing and the first patient was
and mortality in the Losartan Intervention For End-
randomised January 2004. There are currently 3042
point reduction in hypertension study (LIFE): a
randomised trial against atenolol. Lancet 2002; 359:995–1003.
12 Vyssoulis GP, Karpanou EA, Kyvelou SM, Adamopoulos
DN, Antonakoudis GC, Deligeorgis AD et al. Beneficial
effect of angiotensin II type 1 receptor blocker anti-hypertensive treatment on arterial stiffness: the role of
Role of the funding source: The study was funded by
smoking. J Clin Hypertens 2008; 10: 201–207.
Kyoto Prefectural University School of Medicine,
13 Miura Y, Yamamoto N, Tsunekawa S, Taguchi S,
with an unrestricted grant from Novartis Pharma
Eguchi Y, Ozaki N et al. Replacement of valsartan
KK, Japan. The sponsor had no role in study design,
data collection, data analysis, data interpretation or
patients with type 2 diabetes: metabolic and anti-
writing of the report. The executive committee will
atherogenic consequences. Diabetes Care 2005; 28:
have full access to all the data at the end of the
14 The ONTARGET Investigators. Telmisartan, ramipril
study, and has final responsibility for the decision to
or both in patients at high risk for vascular events.
N Engl J Med 2008; 358: 1547–1559.
15 Dzau VJ, Antman EM, Black HR, Hayes DL, Manson JE,
Plutzky J et al. The cardiovascular disease continuum
validated: clinical evidence of improved patient out-comes: part II: clinical trial evidence (acute coronary
1 The Sixth Report of the Joint National Committee on
syndromes through renal disease) and future direc-
prevention, detection, evaluation, and treatment of
tions. Circulation 2006; 114: 2871–2891.
high blood pressure. NIH Publication No 98-4080,
16 Mochizuki S, Dahlo¨f B, Shimizu M, Ikewaki K,
Yoshikawa M, Taniguchi I et al. Valsartan in a Japanese
2 Bonow RO, Smaha LA, Smith Jr SC, Mensah GA,
population with hypertension and other cardiovascu-
Lenfant C. World Heart Day 2002: the international
lar disease (Jikei Heart Study). Lancet 2007; 369:
burden of cardiovascular disease: responding to
the emerging global epidemic. Circulation 2002; 106:
17 Ogihara T, Nakao K, Fukui T, Fukiyama K, Ueshima K,
Oba K et al. Effects of candesartan compared with
3 World Health Organization. Death and DAILY estimates
for 2002 by cause for WHO member states: burden of
cardiovascular risks: candesartan antihypertensive
disease statistics (available at http://www.who.int/
survival evaluation in Japan trial. Hypertension 2008;
entity/healthinfo/statistics/bodgbddeathdalyestimates.xls).
4 Kubo M, Kiyohara Y, Kato I, Tanizaki Y, Arima H,
18 Hansson L, Hedner T, Dahlo¨f B. Prospective randomized
Tanaka K et al. Trends in the incidence, mortality, and
open blind endpoint (PROBE) study. A novel design for
survival rate of cardiovascular diseases in a Japanese
intervention trials. Blood Press 1992; 1: 113–119.
community: the Hisayama study. Stroke 2003; 34:
19 Japanese Society of Hypertension Guidelines Subcom-
mittee for the Management of Hypertension. Guide-
5 Tanizaki Y, Kiyohara Y, Kato I, Iwamoto H, Nakayama
lines for the management of hypertension for general
K, Shinohara N et al. Incidence and risk factors for
practitioners. Hypertens Res 2001; 24: 613–634.
subtypes of cerebral infarction in a general population:
20 Kannel WB, Gordon T, Castelli WP, Margolis JR.
the Hisayama study. Stroke 2000; 31: 2616–2622.
Electrocardiographic left ventricular hypertrophy and
6 Miyazaki T, Hirata M, Moriyama K, Sasaki Y, Aono H,
risk of coronary heart disease: the Framingham Study.
Saito T et al. Metabolic syndrome in Japan diagnosed
with visceral fat measurement by computed tomogra-
21 Pocock SJ, Simon R. Sequential treatment assignment
phy. Proc Japan Acad 2005; 81: 471–479.
with balancing for prognostic factors in the controlled
7 Calle E, Thun M, Petrelli J, Rodriguez C, Health C.
clinical trial. Biometrics 1975; 31: 103–115.
Body-mass index and mortality in a prospective cohort
22 Lang RM, Bierig M, Devereux RB, Flachskampf FA,
of U.S. adults. N Eng J Med 1999; 341: 1097–1105.
Foster E, Pellikka PA et al. Recommendations for
Chamber Quantification: a Report from the American
enzyme inhibitors. Circulation 1998; 97: 1411–1420.
Society of Echocardiography’s Guidelines and Stan-
9 Hollenberg NK. European society of cardiology: angio-
dards Committee and the Chamber Quantification
tensin II antagonists in hypertension and beyond.
Writing Group, Developed in Conjunction with the
Angiotensin II antagonists: why is there so much
European Association of Echocardiography, a Branch
excitement? Am J Managed Care 1998; 4(suppl 7):
of the European Society of Cardiology. J Am Soc
10 Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais
23 Wang MSR, Lagakos SW, Ware JH, Hunter DJ, Drazen
G. Effects of an angiotensin-converting-enzyme inhi-
JM. Statistics in medicine-reporting of subgroup
bitor, ramipril, on cardiovascular events in high-risk
analyses in clinical trials. N Engl J Med 2007; 357:
patients. N Engl J Med 2000; 342: 145–153. Journal of Human Hypertension
Medicine, Kyoto Prefectural University of Medi-
Matsubara H supervises the KYOTO HEART Study
cine is the study chairman. B Dahlo¨f, Department
(KHS) as the chief investigator, and several staff
of Medicine, Sahlgrenska University Hospital/
have been appointed by the chief investigator
¨ stra, Go¨teborg, Sweden, is the honorary supervisor
to support the management of the study as repre-
of the logistics, and conducts the reporting of the
sentatives of the KHS group secretariat. The KHS
is administered by the Steering Committee, whichis composed of academic leaders appointed bythe chief investigator. The role of the Steering
Committee is to supervise the overall execution of
Kyoto Prefectural University of Medicine—T Sawa-
da (Main Steering Committee Member), T Shiraya-
In the KHS, the Data and Safety Monitoring Board
ma, Y Mori, M Okigaki, A Matsumuro, H Yamada,
(DSMB), the Endpoint Committee and the Safety
Y Tsutsumi, M Matoba, T Takahashi, H Shiraishi,
Committee are organised independently from the
K Ikeda, T Nakamura and T Yamada; National
study group and each organisation consists of three
Hospital Organization Maizuru Medical Center—S
external experts. The DSMB members are blinded to
Hirano; National Hospital Organization Shiga Hos-
the allocation of drug treatment groups, meet
pital—A Azuma; Kyoto Prefectural Yosanoumi
periodically, have a stopping guideline for terminat-
Hospital—S Kimura; Akashi Municipal Hospital—
ing the trial prematurely and make recommenda-
S Sasaki; Ayabe City Hospital—K Shiga; Omihachi-
tions to the Steering Committee about the ethical
man Community Medical Center—K Maki; Kyoto
aspects of trial continuation by evaluating each case
City Hospital—K Furukawa; Kumihama Hospital—S
of possible adverse events. This study will finish
Okuda; Nantan General Hospital—Y Kajita; Fuku-
when the number of primary endpoints reaches the
chiyama City Hospital—M Nishio; Kyoto First Red
hypothesis after the end of enrolment. The DSMB
Cross Hospital—Y Kohno; Kyoto Second Red Cross
will review the effectiveness and safety of the study
Hospital—M Kitamura; Maizuru Red Cross Hospi-
at regular intervals. This board executes three
tal—K Nishida; Saiseikai Kyoto Hospital—Y Yama-
interim analyses, with the O’Brien–Fleming meth-
od. Yagi K, who is a chief biostatistician at the Louis
Uji Hospital—S Sawada; Gakkentoshi Hospital—R
Pasteur Center for Medical Research, Kyoto, Japan,
Sakai; Kameoka Municipal Hospital—T Kuriyama;
appointed the DSMB members consisting of two
Kyoto Kizugawa Hospital—H Miyanaga; Kyoto
physicians who are independent of the study. The
Interdisciplinary Institute Hospital of Community
Endpoint Committee and the Safety Committee are
Medicine—T Kitani; Social Insurance Kyoto Hospi-
blinded to the allocation of drug treatment groups
tal—H Haruyama; Shakaihoken Kobe Central Hos-
and the results of the study, and are managed
pital—A Nishio; Kouseikai Takeda Hospital—N
separately from investigators and biostatisticians.
Kinoshita; Aijyukai Dohjin Hospital—S Inagaki;
The Safety Committee has the role to oversee the
Matsushita Memorial Hospital—H Sugihara; Aisei-
welfare of patients enroled in the trial from the
kai Yamashina Hospital—M Katamura; Midorigaoka
ethical point of view. In addition, the Substudy
Hospital—T Hachiya; Asahi University Murakami
committee is organised according to the agreement
Memorial Hospital—S Kato; Meiji University of
of the Steering Committee. Investigators are blinded
Oriental Medicine Hospital—K Ohtsuki.
to the allocation of drug treatment groups and theresults of the study until the discontinuation reportfrom the DSMB or the final report of the study data
J Higaki, Department of Integrated Medicine and
Data collection and management, and allocation
Informatics, Ehime University Graduate School of
for drug treatment groups are conducted by the
Medicine, Shitsukawa, Japan; S Kim-Mitsuyama,
automatic electronic data-capturing system using
Department of Pharmacology and Molecular Ther-
the wide area network with a secure server managed
apeutics, Kumamoto University Graduate School of
by the data centre in Kobe, which is independent of
Medical Sciences, Kumamoto, Japan; T Ichiki,
the study implementation group. The statistical
Department of Cardiovascular Medicine, Kyushu
analysis of the data is performed by the biostatisti-
University Graduate School of Medical Sciences,
cians at the Louis Pasteur Center for Medical
Research, Kyoto, Japan, who are blinded to theallocation of drug treatment groups and indepen-
dent of the study implementation group and the
M Kitakaze, Department of Cardiovascular Medi-
funding source. The Data monitoring team periodi-
cine, National Cardiovascular Center, Osaka, Japan;
cally visits randomly selected investigators to check
T Sugiura, Department of Clinical Laboratory
the suitability between the hospital data and the
Medicine, Kochi Medical School, Kochi University,
input data presented by internet network system.
Kochi, Japan; H Rakugi, Department of Geriatric
Journal of Human Hypertension
Medicine, Osaka University Graduate School of
K Yagi, Louis Pasteur Center for Medical Research,Kyoto, Japan; Nobuo Shirahashi, Department ofPreventive Medicine and Environmental Health,
Osaka City University Medical School, Osaka,
K Yagi, Louis Pasteur Center for Medical Research,
Kyoto, Japan; K Kanda, Department of Cardiovascu-lar surgery, Division of Surgery, Graduate School ofMedical Science, Kyoto Prefectural University ofMedicine, Kyoto, Japan; C Sakakura, Department of
Digestive Surgery, Division of Surgery, Graduate
M Miki, Kyoto Prefectural University School of
School of Medical Science, Kyoto Prefectural Uni-
Medicine, Kyoto, Japan; S Toyoda, Kyoto Prefectural
University School of Medicine, Kyoto, Japan. Journal of Human Hypertension
SWINE FLU AND PREGNANCY How to protect yourself and your baby This leaflet gives information about: • the swine flu vaccination that you can have during pregnancy to help protect you and your baby • precautions you can take to reduce your risk of infection • treatments that are available if you do become ill. Flu. Protect yourself and others. SWINE FLU AND P
Revised October 2009, approved January 2010 Flowchart for the Management of Blood Glucose in Type 2 Flowchart for the Management of Blood Glucose in Type 2 Diabetes Mellitus Aim for target HbA1c 6.5-7.5% (or agreed individualised targets) Target set based on macrovascular and microvascular complications. Higher target if at risk of hypoglycaemia. Avoid intensive managem
 Journal of Human Hypertension (2009) 23, 188–195
& 2009 Macmillan Publishers Limited All rights reserved 0950-9240/09 $32.00
Rationale and design of the KYOTOHEART study: effects of valsartan onmorbidity and mortality in uncontrolledhypertensive patients with high risk ofcardiovascular events
T Sawada1, T Takahashi1, H Yamada1, B Dahlo¨f2 and H Matsubara1, for the KYOTO HEART
Study Group1Department of Cardiovascular Medicine, Kyoto Prefectural University School of Medicine, Kyoto, Japan and2Department of Medicine, Sahlgrenska University Hospital/O¨stra, Go¨teborg, Sweden
It remains to be determined whether the evidence in
treatment with valsartan or conventional non-angioten-
Western countries for blockade of the renin–angiotensin
sin receptor blocker therapies, and the follow-up
System in cardiovascular diseases could be directly
period will be at least 3 years. The primary end point is
applied to East Asian races including the Japanese
a composite of defined cardio- or cerebro-vascular
population as a long-term strategy. The KYOTO HEART
events. Secondary end points include all causes of
Study (KHS) is designed to investigate the add-on effect
mortality, worsening of cardiac function, new onset or
of valsartan versus conventional anti-hypertensive
worsening of arrhythmias or diabetes mellitus. The KHS
treatment on cardiovascular morbidity and mortality in
will provide new evidence for the management of blood
Japanese hypertensive patients with uncontrolled blood
pressure in hypertensive patients with high risk.
Journal of Human Hypertension (2009) 23, 188–195
& 2009 Macmillan Publishers Limited All rights reserved 0950-9240/09 $32.00
Rationale and design of the KYOTOHEART study: effects of valsartan onmorbidity and mortality in uncontrolledhypertensive patients with high risk ofcardiovascular events
T Sawada1, T Takahashi1, H Yamada1, B Dahlo¨f2 and H Matsubara1, for the KYOTO HEART
Study Group1Department of Cardiovascular Medicine, Kyoto Prefectural University School of Medicine, Kyoto, Japan and2Department of Medicine, Sahlgrenska University Hospital/O¨stra, Go¨teborg, Sweden
It remains to be determined whether the evidence in
treatment with valsartan or conventional non-angioten-
Western countries for blockade of the renin–angiotensin
sin receptor blocker therapies, and the follow-up
System in cardiovascular diseases could be directly
period will be at least 3 years. The primary end point is
applied to East Asian races including the Japanese
a composite of defined cardio- or cerebro-vascular
population as a long-term strategy. The KYOTO HEART
events. Secondary end points include all causes of
Study (KHS) is designed to investigate the add-on effect
mortality, worsening of cardiac function, new onset or
of valsartan versus conventional anti-hypertensive
worsening of arrhythmias or diabetes mellitus. The KHS
treatment on cardiovascular morbidity and mortality in
will provide new evidence for the management of blood
Japanese hypertensive patients with uncontrolled blood
pressure in hypertensive patients with high risk. which are reflected in body mass index (mean BMI:
pressure control, on major cardiovascular events
23–25 and 28–30 kg/m2, respectively).6,7 Most of
and in particular the incidences of stroke, heart
mortality–morbidity trials have been carried out in
failure and coronary artery events. In contrast, the
Western country, in which none or only a minority
Candesartan Antihypertensive Survival Evaluation
of East Asian patients were included. Owing to the
in Japan (CASE-J) anti-hypertensive study reported
paucity of large-scale trials in East Asian people,
that candesartan-based and amlodipine-based regi-
it remains to be determined whether the results from
mens produced no statistical differences between
similar clinical trials in Western societies are
therapies on stroke or cardiovascular events in high-
internationally applicable to East Asian races or
risk Japanese hypertensive patients.17 The KYOTO
the Japanese population, or whether genetic back-
HEART Study (KHS) will be important to solve this
ground can cause different pharmacokinetic and
pharmacodynamic responses to the same drug.
which are reflected in body mass index (mean BMI:
pressure control, on major cardiovascular events
23–25 and 28–30 kg/m2, respectively).6,7 Most of
and in particular the incidences of stroke, heart
mortality–morbidity trials have been carried out in
failure and coronary artery events. In contrast, the
Western country, in which none or only a minority
Candesartan Antihypertensive Survival Evaluation
of East Asian patients were included. Owing to the
in Japan (CASE-J) anti-hypertensive study reported
paucity of large-scale trials in East Asian people,
that candesartan-based and amlodipine-based regi-
it remains to be determined whether the results from
mens produced no statistical differences between
similar clinical trials in Western societies are
therapies on stroke or cardiovascular events in high-
internationally applicable to East Asian races or
risk Japanese hypertensive patients.17 The KYOTO
the Japanese population, or whether genetic back-
HEART Study (KHS) will be important to solve this
ground can cause different pharmacokinetic and
pharmacodynamic responses to the same drug. measurements was calculated and recorded. The
(11) patients who were unwilling or unable to
timing of blood pressure measurement was not
constant in relation to patients’ intake of medica-tion. When patients were already treated for hyper-tension, anti-hypertensive drugs other than ARB
were administered for the first 4 weeks and then if
The protocol was approved by the Ethics Committee
still uncontrolled (X140/90), they were considered
at each participating centre. At the first clinic visit,
as candidates for the study. Uncontrolled hyperten-
the trial objectives, study design, and the risks and
sive patients treated with ACE inhibitors before
benefits of study participation were explained care-
randomisation could also participate in this study.
measurements was calculated and recorded. The
(11) patients who were unwilling or unable to
timing of blood pressure measurement was not
constant in relation to patients’ intake of medica-tion. When patients were already treated for hyper-tension, anti-hypertensive drugs other than ARB
were administered for the first 4 weeks and then if
The protocol was approved by the Ethics Committee
still uncontrolled (X140/90), they were considered
at each participating centre. At the first clinic visit,
as candidates for the study. Uncontrolled hyperten-
the trial objectives, study design, and the risks and
sive patients treated with ACE inhibitors before
benefits of study participation were explained care-
randomisation could also participate in this study.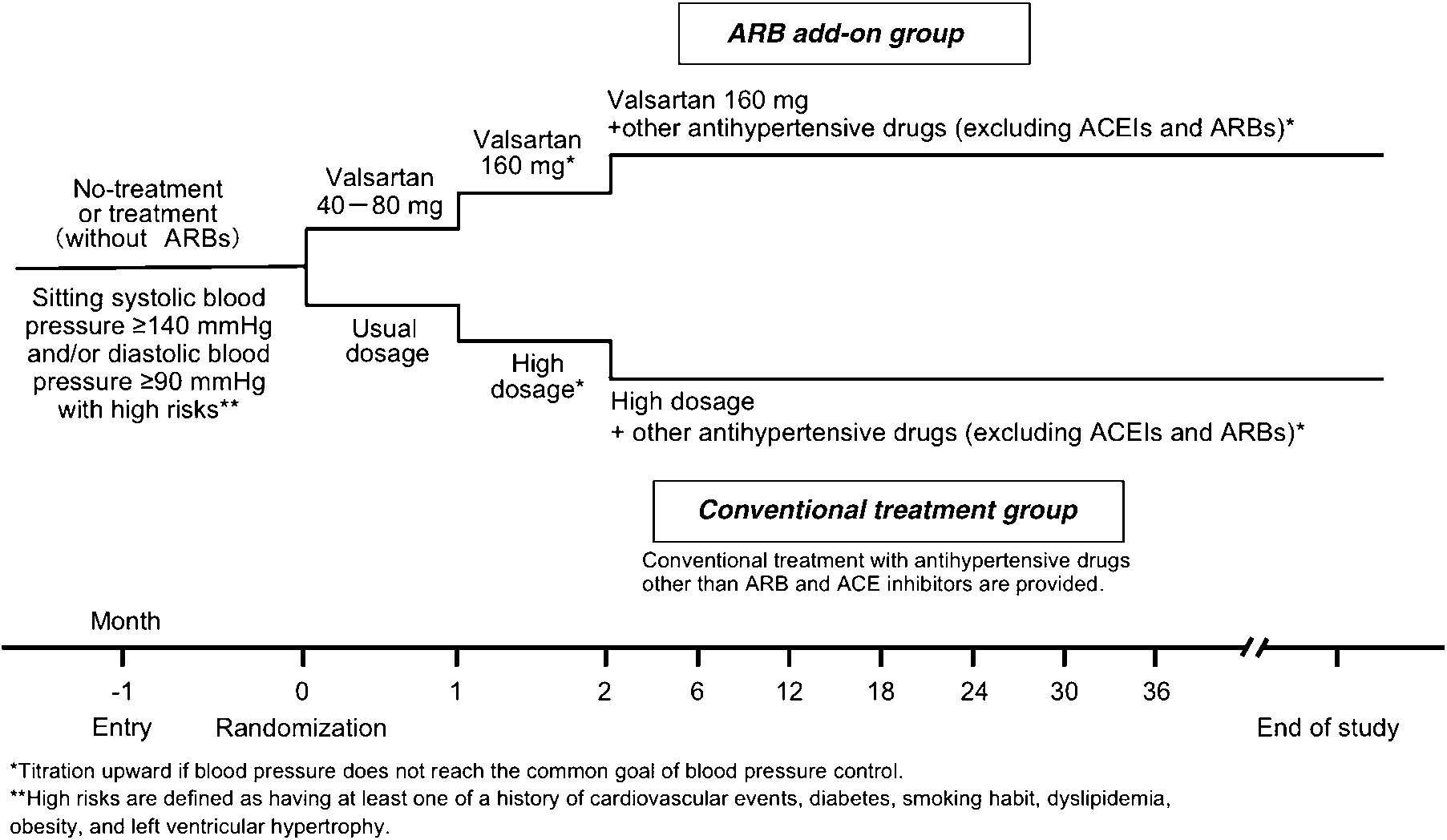
 Figure 1 Titration schedule for the KYOTO HEART Study.
Figure 1 Titration schedule for the KYOTO HEART Study. sound echocardiogram, and the efficacy of valsartan
On the basis of results of large end point studies
with/without diabetes and with/without metabolic
patients, the number of patients to be enroled wascalculated as 3000 (1500 in each group) to validatethe hypothesis under the assumption that the
valsartan add-on group achieves a 20% risk reduc-
Recruitment began in January 2004 and follow-up is
tion compared with the conventional treatment
calculated to go on until 2010 or to a time point
group and gives 80% statistical power for detecting
when the pre-determined number of patients with a
clinically significant between-group differences
primary end point has been reached, unless there is
with a two tailed 5% statistical significant level.
sound echocardiogram, and the efficacy of valsartan
On the basis of results of large end point studies
with/without diabetes and with/without metabolic
patients, the number of patients to be enroled wascalculated as 3000 (1500 in each group) to validatethe hypothesis under the assumption that the
valsartan add-on group achieves a 20% risk reduc-
Recruitment began in January 2004 and follow-up is
tion compared with the conventional treatment
calculated to go on until 2010 or to a time point
group and gives 80% statistical power for detecting
when the pre-determined number of patients with a
clinically significant between-group differences
primary end point has been reached, unless there is
with a two tailed 5% statistical significant level. studies is related to molecule specific differences
11 Dahlo¨f B, Devereux RB, Kjeldsen SE, Julius S,
between ARBs or related to different study designs.
studies is related to molecule specific differences
11 Dahlo¨f B, Devereux RB, Kjeldsen SE, Julius S,
between ARBs or related to different study designs. Medicine, Kyoto Prefectural University of Medi-
Matsubara H supervises the KYOTO HEART Study
cine is the study chairman. B Dahlo¨f, Department
(KHS) as the chief investigator, and several staff
of Medicine, Sahlgrenska University Hospital/
have been appointed by the chief investigator
¨ stra, Go¨teborg, Sweden, is the honorary supervisor
to support the management of the study as repre-
of the logistics, and conducts the reporting of the
sentatives of the KHS group secretariat. The KHS
is administered by the Steering Committee, whichis composed of academic leaders appointed bythe chief investigator. The role of the Steering
Committee is to supervise the overall execution of
Kyoto Prefectural University of Medicine—T Sawa-
da (Main Steering Committee Member), T Shiraya-
In the KHS, the Data and Safety Monitoring Board
ma, Y Mori, M Okigaki, A Matsumuro, H Yamada,
(DSMB), the Endpoint Committee and the Safety
Y Tsutsumi, M Matoba, T Takahashi, H Shiraishi,
Committee are organised independently from the
K Ikeda, T Nakamura and T Yamada; National
study group and each organisation consists of three
Hospital Organization Maizuru Medical Center—S
external experts. The DSMB members are blinded to
Hirano; National Hospital Organization Shiga Hos-
the allocation of drug treatment groups, meet
pital—A Azuma; Kyoto Prefectural Yosanoumi
periodically, have a stopping guideline for terminat-
Hospital—S Kimura; Akashi Municipal Hospital—
ing the trial prematurely and make recommenda-
S Sasaki; Ayabe City Hospital—K Shiga; Omihachi-
tions to the Steering Committee about the ethical
man Community Medical Center—K Maki; Kyoto
aspects of trial continuation by evaluating each case
City Hospital—K Furukawa; Kumihama Hospital—S
of possible adverse events. This study will finish
Okuda; Nantan General Hospital—Y Kajita; Fuku-
when the number of primary endpoints reaches the
chiyama City Hospital—M Nishio; Kyoto First Red
hypothesis after the end of enrolment. The DSMB
Cross Hospital—Y Kohno; Kyoto Second Red Cross
will review the effectiveness and safety of the study
Hospital—M Kitamura; Maizuru Red Cross Hospi-
at regular intervals. This board executes three
tal—K Nishida; Saiseikai Kyoto Hospital—Y Yama-
interim analyses, with the O’Brien–Fleming meth-
od. Yagi K, who is a chief biostatistician at the Louis
Uji Hospital—S Sawada; Gakkentoshi Hospital—R
Pasteur Center for Medical Research, Kyoto, Japan,
Sakai; Kameoka Municipal Hospital—T Kuriyama;
appointed the DSMB members consisting of two
Kyoto Kizugawa Hospital—H Miyanaga; Kyoto
physicians who are independent of the study. The
Interdisciplinary Institute Hospital of Community
Endpoint Committee and the Safety Committee are
Medicine—T Kitani; Social Insurance Kyoto Hospi-
blinded to the allocation of drug treatment groups
tal—H Haruyama; Shakaihoken Kobe Central Hos-
and the results of the study, and are managed
pital—A Nishio; Kouseikai Takeda Hospital—N
separately from investigators and biostatisticians.
Medicine, Kyoto Prefectural University of Medi-
Matsubara H supervises the KYOTO HEART Study
cine is the study chairman. B Dahlo¨f, Department
(KHS) as the chief investigator, and several staff
of Medicine, Sahlgrenska University Hospital/
have been appointed by the chief investigator
¨ stra, Go¨teborg, Sweden, is the honorary supervisor
to support the management of the study as repre-
of the logistics, and conducts the reporting of the
sentatives of the KHS group secretariat. The KHS
is administered by the Steering Committee, whichis composed of academic leaders appointed bythe chief investigator. The role of the Steering
Committee is to supervise the overall execution of
Kyoto Prefectural University of Medicine—T Sawa-
da (Main Steering Committee Member), T Shiraya-
In the KHS, the Data and Safety Monitoring Board
ma, Y Mori, M Okigaki, A Matsumuro, H Yamada,
(DSMB), the Endpoint Committee and the Safety
Y Tsutsumi, M Matoba, T Takahashi, H Shiraishi,
Committee are organised independently from the
K Ikeda, T Nakamura and T Yamada; National
study group and each organisation consists of three
Hospital Organization Maizuru Medical Center—S
external experts. The DSMB members are blinded to
Hirano; National Hospital Organization Shiga Hos-
the allocation of drug treatment groups, meet
pital—A Azuma; Kyoto Prefectural Yosanoumi
periodically, have a stopping guideline for terminat-
Hospital—S Kimura; Akashi Municipal Hospital—
ing the trial prematurely and make recommenda-
S Sasaki; Ayabe City Hospital—K Shiga; Omihachi-
tions to the Steering Committee about the ethical
man Community Medical Center—K Maki; Kyoto
aspects of trial continuation by evaluating each case
City Hospital—K Furukawa; Kumihama Hospital—S
of possible adverse events. This study will finish
Okuda; Nantan General Hospital—Y Kajita; Fuku-
when the number of primary endpoints reaches the
chiyama City Hospital—M Nishio; Kyoto First Red
hypothesis after the end of enrolment. The DSMB
Cross Hospital—Y Kohno; Kyoto Second Red Cross
will review the effectiveness and safety of the study
Hospital—M Kitamura; Maizuru Red Cross Hospi-
at regular intervals. This board executes three
tal—K Nishida; Saiseikai Kyoto Hospital—Y Yama-
interim analyses, with the O’Brien–Fleming meth-
od. Yagi K, who is a chief biostatistician at the Louis
Uji Hospital—S Sawada; Gakkentoshi Hospital—R
Pasteur Center for Medical Research, Kyoto, Japan,
Sakai; Kameoka Municipal Hospital—T Kuriyama;
appointed the DSMB members consisting of two
Kyoto Kizugawa Hospital—H Miyanaga; Kyoto
physicians who are independent of the study. The
Interdisciplinary Institute Hospital of Community
Endpoint Committee and the Safety Committee are
Medicine—T Kitani; Social Insurance Kyoto Hospi-
blinded to the allocation of drug treatment groups
tal—H Haruyama; Shakaihoken Kobe Central Hos-
and the results of the study, and are managed
pital—A Nishio; Kouseikai Takeda Hospital—N
separately from investigators and biostatisticians. Medicine, Osaka University Graduate School of
K Yagi, Louis Pasteur Center for Medical Research,Kyoto, Japan; Nobuo Shirahashi, Department ofPreventive Medicine and Environmental Health,
Osaka City University Medical School, Osaka,
K Yagi, Louis Pasteur Center for Medical Research,
Kyoto, Japan; K Kanda, Department of Cardiovascu-lar surgery, Division of Surgery, Graduate School ofMedical Science, Kyoto Prefectural University ofMedicine, Kyoto, Japan; C Sakakura, Department of
Digestive Surgery, Division of Surgery, Graduate
M Miki, Kyoto Prefectural University School of
School of Medical Science, Kyoto Prefectural Uni-
Medicine, Kyoto, Japan; S Toyoda, Kyoto Prefectural
University School of Medicine, Kyoto, Japan.
Medicine, Osaka University Graduate School of
K Yagi, Louis Pasteur Center for Medical Research,Kyoto, Japan; Nobuo Shirahashi, Department ofPreventive Medicine and Environmental Health,
Osaka City University Medical School, Osaka,
K Yagi, Louis Pasteur Center for Medical Research,
Kyoto, Japan; K Kanda, Department of Cardiovascu-lar surgery, Division of Surgery, Graduate School ofMedical Science, Kyoto Prefectural University ofMedicine, Kyoto, Japan; C Sakakura, Department of
Digestive Surgery, Division of Surgery, Graduate
M Miki, Kyoto Prefectural University School of
School of Medical Science, Kyoto Prefectural Uni-
Medicine, Kyoto, Japan; S Toyoda, Kyoto Prefectural
University School of Medicine, Kyoto, Japan.