Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Dear patient: thank you for taking the time to carefully fill out this paperwork
1. When you have headaches, how often is the pain severe?
2. How often do headaches limit your ability to do usual daily activities including household work,
3. When you have a headache, how often do you wish you could lie down?
4. In the past 4 weeks, how often have you felt too tired to do work or daily activities because of
5. In the past 4 weeks, how often have you felt fed up or irritated because of your headaches?
6. In the past 4 weeks, how often did headaches limit your ability to concentrate on work or daily
7. At what age do you remember your first significant headache? _____________________
8. When was the last day you were headache free?
9. When was the last time you had 6 headache-free days in a row? ____________________
10. How often do you have to go to the Emergency Room for headaches? _____________________
11. When your headaches first started, do you remember getting some relief by changing positions
12. What other physicians have you seen for headaches/facial pain?
_____________________________________________________________________________
13. Have you ever been admitted to the hospital for your headaches? ________________________
14. Have you tried chiropractic care or acupuncture for your headaches? Yes or No
15. What studies have you had for your headaches?
a. MRI of head: Y/N Approximate date and place of procedure:____________________
b. CT scan of head: Y/N Approximate date and place of procedure:__________________
c. MRI of neck: Y/N Approximate date and place of procedure:____________________
d. Spinal Tap: Y/N Approximate date and place of procedure:_____________________
17. Do you clench or grind your teeth at night?
19. Do you clench or grind your teeth at night?
20. Have you been diagnosed with TMJ disorder?
21. Does your neck hurt during the headaches?
22. Does your neck hurt when you don’t have a headache? Y or N
Circle any of the medicines below that you tried before to stop headaches once they start: Imitrex tablets
Other medicines used to stop headaches: ______________________________________________________________________
Circle all of the medicines below you have used for prevention of headaches/facial pain: Gabapentin
Other medicines used for headache prevention: ______________________________________________________________________
How many types of headaches do you have?_________ Fill out the information on this page and the following pages for each type of headache you have. Headache #1
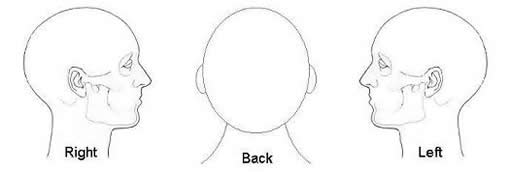
1. Mark the areas where your head hurts for this headache type:
2. Have you had this headache type for less than 3 months? Y or N
3. How would you describe the pain? (examples: throbbing, squeezing, dull,
________________________________________________________________
4. Do you have nausea with this headache?
5. Do you have sensitivity to light with this headache?
6. Do you have sensitivity to sound with this headache?
7. Do you have sensitivity to smell with this headache?
8. Do you have changes in your vision before or during this headache? Y or N
9. Has this headache changed recently? Y or N If so, How has it
changed?________________________________________________________
10. What time of day are these headaches the worst? ________________________
11. What medicines have helped this headache?
________________________________________________________________
12. Circle any of the aggravating factors below:
Aspartame Chocolate Strenuous Monosodium
Headache #2 (If you only have 1 type of headache, you are finished)
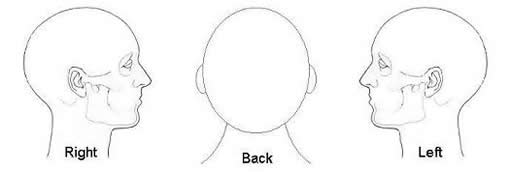
13. Mark the areas where your head hurts for this headache type:
14. Have you had this headache type for less than 3 months? Y or N
15. How would you describe the pain? (examples: throbbing, squeezing, dull,
________________________________________________________________
16. Do you have nausea with this headache?
17. Do you have sensitivity to light with this headache?
18. Do you have sensitivity to sound with this headache?
19. Do you have sensitivity to smell with this headache?
20. Do you have changes in your vision before or during this headache? Y or N
21. Has this headache changed recently? Y or N If so, How has it
changed?________________________________________________________
22. What time of day are these headaches the worst? ________________________
23. What medicines have helped this headache?
________________________________________________________________
24. Circle any of the aggravating factors below:
Aspartame Chocolate Strenuous Monosodium
Part XIV · Ginseng Establishment Insuring Agreement A. General “shade structures” means the posts and shade material used to control garden temperature and light intensity in This Part applies to ginseng seedlings, as defined in this “shade material” means either wooden lath or Except where otherwise provided, the insurance polypropylene cloth used to shade ginseng gardens.
Interpretar é reconhecer-se no outro: o conceito davidsoniano de interpretação radical Este artigo pretende apresentar o conceito de interpretação radical desenvolvido por Donald Davidson. Tal conceito relaciona pensamento, linguagem e mundo, de modo a considerar que só a comunicação pode proporcionar o conceito, sendo o diálogo o contexto real de toda e qualquer objetividad

 1. When you have headaches, how often is the pain severe?
2. How often do headaches limit your ability to do usual daily activities including household work,
3. When you have a headache, how often do you wish you could lie down?
4. In the past 4 weeks, how often have you felt too tired to do work or daily activities because of
5. In the past 4 weeks, how often have you felt fed up or irritated because of your headaches?
6. In the past 4 weeks, how often did headaches limit your ability to concentrate on work or daily
7. At what age do you remember your first significant headache? _____________________
8. When was the last day you were headache free?
9. When was the last time you had 6 headache-free days in a row? ____________________
10. How often do you have to go to the Emergency Room for headaches? _____________________
11. When your headaches first started, do you remember getting some relief by changing positions
12. What other physicians have you seen for headaches/facial pain?
_____________________________________________________________________________
13. Have you ever been admitted to the hospital for your headaches? ________________________
14. Have you tried chiropractic care or acupuncture for your headaches? Yes or No
15. What studies have you had for your headaches?
a. MRI of head: Y/N Approximate date and place of procedure:____________________
b. CT scan of head: Y/N Approximate date and place of procedure:__________________
c. MRI of neck: Y/N Approximate date and place of procedure:____________________
d. Spinal Tap: Y/N Approximate date and place of procedure:_____________________
1. When you have headaches, how often is the pain severe?
2. How often do headaches limit your ability to do usual daily activities including household work,
3. When you have a headache, how often do you wish you could lie down?
4. In the past 4 weeks, how often have you felt too tired to do work or daily activities because of
5. In the past 4 weeks, how often have you felt fed up or irritated because of your headaches?
6. In the past 4 weeks, how often did headaches limit your ability to concentrate on work or daily
7. At what age do you remember your first significant headache? _____________________
8. When was the last day you were headache free?
9. When was the last time you had 6 headache-free days in a row? ____________________
10. How often do you have to go to the Emergency Room for headaches? _____________________
11. When your headaches first started, do you remember getting some relief by changing positions
12. What other physicians have you seen for headaches/facial pain?
_____________________________________________________________________________
13. Have you ever been admitted to the hospital for your headaches? ________________________
14. Have you tried chiropractic care or acupuncture for your headaches? Yes or No
15. What studies have you had for your headaches?
a. MRI of head: Y/N Approximate date and place of procedure:____________________
b. CT scan of head: Y/N Approximate date and place of procedure:__________________
c. MRI of neck: Y/N Approximate date and place of procedure:____________________
d. Spinal Tap: Y/N Approximate date and place of procedure:_____________________

 17. Do you clench or grind your teeth at night?
19. Do you clench or grind your teeth at night?
20. Have you been diagnosed with TMJ disorder?
21. Does your neck hurt during the headaches?
22. Does your neck hurt when you don’t have a headache? Y or N
Circle any of the medicines below that you tried before to stop headaches once they start: Imitrex tablets
Other medicines used to stop headaches: ______________________________________________________________________
Circle all of the medicines below you have used for prevention of headaches/facial pain: Gabapentin
Other medicines used for headache prevention: ______________________________________________________________________
17. Do you clench or grind your teeth at night?
19. Do you clench or grind your teeth at night?
20. Have you been diagnosed with TMJ disorder?
21. Does your neck hurt during the headaches?
22. Does your neck hurt when you don’t have a headache? Y or N
Circle any of the medicines below that you tried before to stop headaches once they start: Imitrex tablets
Other medicines used to stop headaches: ______________________________________________________________________
Circle all of the medicines below you have used for prevention of headaches/facial pain: Gabapentin
Other medicines used for headache prevention: ______________________________________________________________________




 Headache #2 (If you only have 1 type of headache, you are finished)
Headache #2 (If you only have 1 type of headache, you are finished)