Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Doi:10.1016/s1473-0502(02)00104-0
Transfusion and Apheresis Science 28 (2003) 93–100
The Norwegian plasma fractionation project––a
12 year clinical and economic success story
O. Flesland a,b,*, J. Seghatchian c, B.G. Solheim b
a Blood Bank, Baerum Hospital, N-1306 Barum, Norway
b Institute of Immunology, Rikshospitalet University Hospital, N-0027 Oslo, Norway
c Blood Component Technology and Thrombosis/Haemostasis Consultancy, 50 Primeroe Hill Road, London NW3 3AA, UK
The establishment of the Norwegian Fractionation Project (Project) was of major importance in preserving national
self-sufficiency when plasma, cryoprecipitate and small batch factor IX-concentrates were replaced by virus inactivatedproducts in the last part of the 1980s. Fractionation was performed abroad by contract with Octapharma after tenderson the European market. All Norwegian blood banks (>50) participated in the Project. Total yearly production was50–60 tons of mainly recovered plasma. From 1993 solvent detergent (SD) treated plasma has replaced other plasma fortransfusion.
The blood banks paid for the fractionation and/or viral inactivation process, while the plasma remained the property
of the blood banks and the final products were returned to the blood banks. The Project sold surplus products to otherNorwegian blood banks and the majority of the coagulation factor concentrates to The Institute of Haemophilia andRikshospitalet University Hospital. Both plasma and blood bank quality was improved by the Project. Clinical ex-perience with the products has been satisfactory and self-sufficiency has been achieved for all major plasma proteins andSD plasma, but a surplus exceeding 3 years consumption of albumin has accumulated due to decreasing clinical use.
The Project has secured high yields of the fractionated products and the net income from the produced products is
NOK 1115 (140 € or US$) per litre plasma. An increasing surplus of albumin and the possibility of significant salesabroad of currently not fractionated IVIgG, could lead to a reorganisation of the Project from that of a co-ordinator toa national plasma handling unit. This unit could buy the plasma from the blood banks and have the plasma frac-tionated by contract after tender, before selling the products back for cost recovery. The small blood banks couldproduce plasma for products for the Norwegian market, while surplus products from the larger blood banks which arecertified for delivery of plasma for fractionation of products to be consumed in the European Community, could be soldon the international market. Ó 2003 Elsevier Science Ltd. All rights reserved.
Abbreviations: HIV: human immunodeficiency virus; HAV: hepatitis A virus; HCV: hepatitis C virus; SD: solvent detergentKeywords: Blood; Plasma; Plasma fractionation; Self-sufficiency; Factor VIII; IVIgG; SD-plasma; Octaplasâ; Uniplasâ
* Corresponding author. Address: Blood Bank, Baerum
Hospital, N-1306 Barum, Norway. Tel.: +47-6780-9703; fax:
Norway is a sparsely populated country with 4.5
million inhabitants. Blood donation is voluntary
and non-remunerated, and all blood banks are
1473-0502/03/$ - see front matter Ó 2003 Elsevier Science Ltd. All rights reserved. doi:10.1016/S1473-0502(02)00104-0
O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
hospital-associated. Self-sufficiency has been a na-
fractionation in 1988, when the fractionation was
tional goal since 1980. Norwegian blood banks
performed at CRTS in Lille, France. All the frac-
produce 50–60 tons of plasma per year, of which
tionation products from the fractionation are re-
approximately 90% has been recovered plasma.
This is not enough to establish a fractionationplant. The plasma is collected in more than 50 dif-ferent blood banks, making each individual blood
bank commercially uninteresting to the interna-tional plasma fractionation industry. At the same
As each blood bank is small, the time for col-
time there is a demand for safe blood products.
lecting one full individual batch of plasma for
In the first part of the 1980s, the policy of self-
fractionation would be long. The Project ensures
sufficiency and use of cryoprecipitates and factor
that fresh frozen plasma (FFP) is shipped from
XI prepared from small plasma pools ensured a
several blood banks at a time, hence reducing
high quality of life for Norwegian haemophiliacs
storage time before fractionation. The Project also
and secured a prevalence of anti-HIV of only 6%
stores the returned fractionated products. Each
for the whole haemophilia population [1]. Because
blood bank orders from this store, when needed,
of the human immunodeficiency virus (HIV) epi-
ensuring that the oldest products are used first.
demic, the Norwegian Health Authorities decided
Most of the coagulation factors are sold to the
in 1985 that plasma, cryoprecipitate and factor IX
National Institute of Haemophilia and Rikshos-
should be replaced by virus inactivated plasma
pitalet University Hospital. Factor VIII is made
products prepared from Norwegian plasma by
from all of the plasma. Also, until recently albu-
1988. A pilot project for contract fractionation was
min has been made from all of the plasma. The
initiated by the Red Cross and National Hospital
Project ensures that enough, but not too much, of
Blood Centre in 1986. After an increasing number
other plasma products are produced. Initially this
of blood banks joined the project during 1987–88,
was factor IX and prothrombin complex (factors
the Norwegian Plasma Fractionation Project was
II, VII, IX and X). Later, intravenous immuno-
established and took over co-ordination of con-
globulin (IVIgG) and solvent detergent (SD)
tract fractionation as of January 1989. The con-
treated plasma and cryoprecipitate were intro-
tract fractionation initiative, the postponement of
elective orthopedic surgery in haemophiliacs, anda special grant by the Norwegian Parliament forequipment for freezing and storage of plasma, en-
abled the transition to virally inactivated plasmaproducts with the retention of self-sufficiency [2].
The Project helped to improve the quality of the
The Project collects plasma from all blood
blood banks and the plasma. In order to secure
banks in the country. Based on tenders on the
high yields of factor VIII, product quality became
a point of interest for the blood bank community
Switzerland) has fractionated and/or virus inacti-
from the start, resulting in standardised proce-
vated the plasma since 1988 according to contract.
dures being introduced. FFP which amounted to
On behalf of the blood banks and the Norwegian
95% of the plasma, was generally produced by
counties, the National Institute of Health issued
separation of whole blood within 4 h after collec-
tenders and was the formal contract partner in
tion and promptly snap frozen (core temperature
relation to Octapharma. With respect to the Pro-
<)28 °C within 35 min for 300 ml bags). Norwe-
ject, the Blood Bank Council (appointed by the
gian GMP guidelines were written and inspection
Directorate of Health) was the professional ad-
by pharmacists from the Surgeon GeneralÕs office
viser to the Institute. Production has been carried
were started largely because of this project [3]. ISO
out at OctapharmaÕs plant in Vienna, Austria,
certification and accreditation is now the next step
except for the first eight months of 1989 and test
for several blood banks. Another issue will be
O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
certification of larger blood banks for delivery of
high amounts of anti-Parvovirus B19 IgG. When
plasma for commercial fractionation of products
analysing patients at risk for Parvovirus B19 in-
to be consumed in the European Community.
fection one out of nine patients transfused with
Virus inactivation by SD treatment has been the
only SD-plasma and 8 out of 14 patients trans-
standard procedure for the plasma products. Since
fused with SD-plasma and cellular components,
1998 an additional step of dry-heat treatment or
seroconverted and developed anti-Parvovirus B19
nanofiltration has been added for the coagulation
antibody positive status, however none of them
developed clinical symptoms of disease.
Tests for antibodies directed against HIV and
A study on fractionated albumin [14] demon-
hepatitis C virus (HCV) were introduced in Nor-
strates blocking of transport sites on albumin due
way promptly after they were commercially avail-
to stabilisers added (sodiumcaprylate and acetyl-
able. Due to low HCV prevalence [4], introduction
tryptophan) during pasteurisation of the product,
of NAT test for HCV was delayed until April 2000,
while albumin in SD-plasma is not affected. These
when a small pool test (24 samples) was introduced
transport sites are essential for the binding to al-
for all blood and plasma collections. However,
bumin of such drugs as Naproxen, Warfarin and
according to European guidelines, Octapharma
introduced NAT testing for HCV on all plasmabatches from July 1999. The delay in introductionof small pool NAT-testing in Norway led to the
loss of products from two batches of plasma (onefor fractionation and one for SD-plasma produc-
A successful clinical study with SD-plasma was
tion) due to positive NAT tests for HCV in the final
performed at the Rikshospitalet, University Hos-
production pools. This demonstrated that small
pital, in 1992 [8]. In 1993, Norway was the first
pool testing, even if expensive, is cheaper than
country to introduce SD-plasma as the sole plasma
losing whole batches of plasma and corresponding
for transfusion. The documentation for Methylene
products. From April 2000, small pool HCV NAT
blue treatment of plasma was evaluated as insuf-
testing also became a requirement for the release of
cellular products. We have not yet introduced do-
nor exclusion of people who have spent time in the
plasma (Octaplasâ) differs from the method ap-
UK. This may delay commercialisation further.
plied by Vitex in the US for Plasâ þ SD. Twomajor differences for Octaplasâ are a smaller batchsize (200–380 l versus 600–1500 l) and that a final
ultrafiltration/concentration step performed byVitex is omitted. In addition stabilisation of co-
A research fund of NOK 0.75 million estab-
agulation factors and final citrate concentration
lished by the Project, supports scientific activities
differs for the two products. Pool size increases the
within transfusion medicine. In addition, Octa-
process time, which can affect labile proteins and
pharma has sponsored clinical studies, which have
loss of activity due to absorbtion, while ultrafil-
been carried out as agreed to with hospital re-
tration could influence the good haemostatic bal-
search organisations. These agreements ensure the
ance observed between the coagulation factors
investigatorsÕ rights to publish the study results.
and coagulation inhibitors in Octaplasâ [15]. This
The studies on IVIgG [5–7] and SD-plasma [8–
may explain problems recently observed with
12] have demonstrated good product quality and
Plasâ þ SD and not with Octaplasâ. In addition
interesting clinical results. A study performed by
a2-antiplasmin activity has been reported lacking
us demonstrated that antibodies directed against
in the US produced SD-plasma [16] while it is re-
Parvovirus B19 in SD-plasma, neutralise Parvo-
duced at the most by 76% in Octaplas [15,17–20].
virus B19 in the product [10,13]. Out of 25 plasma
Because a2-antiplasmin is a liver synthesised acute
batches tested, all contained Parvovirus B19 and
phase serine protease inhibitor of plasmin [21], this
O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
could result in fibrinolysis in patients with severe
All haemophilia patients are regularly tested for
liver failure. It should therefore be considered to
viral disease transmission. For enveloped viruses,
administrate serine protease inhibitor (i.e. Apro-
which are inactivated by SD the treatment, only
tinin) when transfusing Octaplasâ to patients with
one seroconversion for HCV has been observed.
severe liver failure (including liver transplants) or
No other patients treated with products from the
with high risk of fibrinolysis. Due to the ultrafil-
same batches seroconverted, nor were any irregu-
tration/concentration process the concentration
larities found with the batches. The conclusion was
of plasma proteins is in general unchanged in the
therefore that the seroconversion was not related
US produced SD-plasma, while a 10% decrease is
to coagulation factor treatment. With respect to
transmission of non-enveloped viruses, which are
After SD-plasma was introduced in Norway,
not affected by SD treatment, four haemophilia
the number of units consumed has increased by
patients were infected with hepatitis A virus
78% to 7.9 units/1000 inhabitants. However, the
(HAV) by highly purified factor VIII in 1998. The
introduction of SD-plasma reduced the unit vol-
batch involved in the HAV transmissions was
ume from 270 to 200 ml, thus the consumed FFP
shown to contain plasma from a donor with vire-
mia in connection with HAV infection. We have
not observed any HAV transmission with cryo-
development and clinical testing of an universal
precipitate or intermediate purity factor VIII
SD-plasma (Uniplasâ) which can be transfused
concentrates [21], but it is documented that the
irrespective of a patients ABO type. In a pro-
content of antibodies against HAV is too low in
spective, randomised study which recently was
the highly purified factor VIII to neutralise the
concluded at Rikshospitalet University Hospital,
HAV [13,22,23]. As a consequence, double viral
Uniplasâ was found to be efficient, well tolerated
inactivation has since been introduced for all pu-
rified coagulation factors and no further viral
A SD treated cryoprecipitate has been produced
by Octapharma for use in Norway in the very few
Since 1993 the SD-plasma, Octpaplasâ, has re-
von Willebrand factor (vWF) deficient patients not
placed FFP and other plasma for transfusion in
responding adequately to the standard factor VIII
Norway. More than 250,000 units have been
product (Octa V.I.â, Octaviâ and Octanateâ).
transfused to all types of patients, including neo-
These are products with a high content of vWF.
nates and 208 liver transplants. Aprotinin has
The SD treated cryoprecipitate also represents a
generally only been used in complicated repeat
cardiac surgery and patients with severe liver fail-ure undergoing liver transplantation. Neithertransmission of viral disease, nor thrombotic/
fibrinolytic complications or TRALI, have beenreported, related to the transfusion of Octaplasâ.
The coagulation factor concentrates are well
The only serious adverse event reported after Oct-
tolerated and the haemophilia patients have ex-
aplasâ transfusion, was due to the misuse of 4 units
pressed satisfaction with the introduction of highly
of Octaplasâ as an acute volume substitution. This
purified factor VIII and IX concentrates which are
resulted in cardiac arrest due to a citrate induced
easier to dissolve and cause less side-effects than
rapid fall in ionised calcium in an elderly patient
low purity concentrates or cryoprecipitate. Only
who, however, was successfully resuscitated.
10% of the patients with a severe deficit of factorVIII have developed an inhibitor to factor VIII (A. Glomstein, personal communication). Due to a
high content of vWF, the factor VIII concentrateshave also given satisfactory treatment results in
The Project has secured Norwegian self-suffi-
ciency. It allowed a smooth transition from cryo-
O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
Fig. 1. Plasma and albumin consumption in Norway from 1985–2001.
precipitate and low purity factor XI to high purity
possibility of commercialisation. This is illustrated
products. In addition, self-sufficiency has been es-
by the consumption of albumin and IVIgG in
tablished for prothrombin complex (factors II,
Norwegian hospitals. After a peak in 1989, when
VII, IX and X), albumin and IVIgG. The amount
we used 332.9 kg albumin/million inhabitants, the
of factor VIII produced has declined due to the
consumption has constantly declined (Fig. 1). The
increased purity of factor VIII, double virus inac-
Cochrane report in 1998 [24] led to a further re-
tivation and the reduced plasma volume (and
duction in albumin use, which in 2001 was only
content of factor VIII) caused by the production
121.5 kg/million inhabitants. By that time we
of A and AB SD-plasma. However, after 1995 a
had a surplus of more than three years production
gradual change has taken place in the factor VIII
of albumin so, to avoid outdating, Octapharma
treatment of children with the substitution of
started to store the albumin paste. The use of
plasma derived factor VIII with recombinant fac-
IVIgG has been low in Norway and IVIgG was
tor VIII. This change also prevented a potential
only produced from 30% of our plasma in 2001.
product shortage by covering the increased factor
Because albumin and, in particular IVIgG, are in
VIII needs when treatment in children in the same
short supply on the international market, Octa-
period was changed from ‘‘on demand’’ adminis-
pharma suggested possible sale of surplus albumin
tration to prophylactic treatment. This policy
and IVIgG outside Norway as early as 1994. This
change was a major reason for the consumption
option was included in the contract from 1998, but
increase from 2 to 3.5 million IU factor VIII/mil-
the Project did not respond to this idea until 2001.
lion inhabitants from 1995 to 2001. However, due
The delayed response was partly due to the blood
to the loss of more than 2 million IU Factor VIII
banks resistance to introduce ALT-testing, which
due to positive HCV NAT tests, 2 million IU
was required for commercialisation. Another
factor VIII from Swedish plasma were imported to
problem was the lack of certification of the blood
ensure the plasma derived factor VIII supply in
banks for delivery of plasma for commercial frac-
2001. Plasma derived factor VIII is currently pri-
tionation of products to be consumed in the Euro-
marily used in adult patients with haemophilia-A
8. Internationalisation and commercialisation
During production, around 0.3% of the plasma
Since the goal of the project was to ensure self-
has been discarded due to excessive haemolysis
sufficiency, too little focus has been put on the
or labelling irregularities. Except for three small
O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
batches of factor VIII, which had to be discarded
The Project is based on the fact that the blood
during pilot production in 1988, there have been
bank that produces the plasma pays for the frac-
no product losses due to production errors.
tionation of this plasma and then owns the prod-
In 1992 three batches of SD-plasma (2580 units)
ucts from fractionation. Input–output from the
were lost when a trailer sank due to a ferry
Project is given in Table 1. Over all, the cost of
wreckage. The loss caused a delay of several
fractionation has been less than the profit from
months in the introduction of SD-plasma in Nor-
the factor VIII sold by the blood banks to the
way, but due to insurance it did not represent an
National Institute of Haemophilia (which has the
economic loss to the Project. Since this incident,
responsibility for home treatment) or Rikshospi-
however, no more than one batch (a monthÕs
talet University Hospital (where treatment of
production) is returned in the same transport.
Norwegian haemophiliacs is centralised). Sale of
The major loss of products was due to two
factor IX, prothrombin complex, SD-treated
plasma batches which tested positive for HCV by
cryoprecipitate and IVIgG to the same units pro-
NAT in 1999 and to look back procedures. The
vided an income of NOK 153 million (19 million €
losses due to look back procedures were increased
or US$). In addition, the blood banks consumed
by the authorities demand to discard products
albumin and SD-plasma worth NOK 461 million
containing plasma collected from a donor one year
(57.5 million € or US$) produced from their own
prior to seroconversion, if the blood bank could
plasma. At the end of 2001, the Project had a stock
not provide samples from the previous dona-
of coagulation factors, albumin, IVIgG and SD
tions which demonstrated negative serological and
plasma worth NOK 62.1 million (7.8 million € or
NAT-testing results. This led to a policy of 100%
US$), and paste worth NOK 10.1 million (1.3
collection and storage of retention samples from
million € or US$), based on international spot
The cost of scrapped products has been divided
On a national scale this has been a very sound
by the blood banks according to the total amount
project. Each blood bank has received the prod-
of plasma delivered to date, and represents NOK
ucts they needed, plus their part of the profit. The
36.5 million (4.6 million (€) or US$) or 2.6% of the
profit has been greater than the costs involved. The
blood banks could look at it two ways; they couldsay that the value of each litre of FFP they pro-duced was approximately NOK 1115 (€ or US$140), or they could say that the plasma products
they used were in fact free of charge. This is mostfavourable, taking into account that only first class
Prices have been set yearly. The Project has
apheresis plasma from licensed blood banks costs
priced its products at, or below, the present in-
€ or US$ 80–90 on the international market, and
ternational market price for each product. The
that about 90% of the Norwegian plasma was the
products have not been subjected to government
less valued recovered plasma. With the reduced
consumption of albumin, this is changing. Hospi-tals using little or no fractionated plasma productspay for fractionation, receive payment for coagu-
lation factors and IVIgG, but have little interest inthe albumin they receive. As albumin presently
Over a period of 12 years the project has ob-
cannot be sold outside Norway, it may appear to
tained a high yield of albumin (26.5g/l plasma) and
be better for the blood bank to sell its FFP to the
factor VIII (212 IU/l plasma) in addition of se-
highest bidder. However, so far no Norwegian
curing the Norwegian needs for factor IX, pro-
blood banks are GMP-certified to deliver plasma
trombin complex (factors II, VII, IX and X),
for fractionation of products to be consumed in
SD-cryoprecipitate, IVIgG and SD-plasma.
the European Community. For blood banks using
O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
Table 1The Norwegian Plasma Fractionation Project: plasma income-products outcome 1989–2001
(include transport,storage and admin-istration)
92.5 (total, subtracted scrapped products)
From a total of 663,638 l of plasma, 599,375 l were fractionated and 64,263 l were used for the production of SD-plasma.
a Included albumin paste worth 0.8. b IU Factor VII. c IU Factor VIII. d Included IVIgG paste worth 0.5. e Unit volume 200 ml.
their entire production of albumin, participation in
The price could be calculated to provide cost re-
the Project is still very lucrative.
covery for the blood banks that supplied FFP,while all surplus products would be sold for themarket price. This would ensure continued na-
tional self-sufficiency and give excellent resultseconomically both for each blood bank and on a
As the Project has been a success for the supply
of safe blood products based on a self-sufficiencyconcept and has generated a significant income tothe blood banks over a long period, it should not
be terminated lightly. At the same time the voicesobjecting to the present situation need to be heard,
The strong support of Director Bodolf Hareide,
since the project is based on all blood banks
CEO National Institute of Health, and the pro-
sharing common interests. One way forward may
fessional guidance by the Blood Bank Council
be to change the role of the Project, from that of a
have been essential for the Project. Tor-Einar
co-ordinator, to a national plasma handling unit.
Svae, Octapharma, initially established the Pro-
This unit could then buy the plasma from the
jects efficient logistics for collection and transport
blood banks and have the plasma fractionated by
of plasma/return and distribution of final prod-
contract after tender, before selling the products
ucts. Jan Erik Orn has been responsible these tasks
back. The small blood banks could produce plas-
ma for products for the Norwegian market, whilesurplus products from the larger blood banks
certified for delivery of plasma for fractionation ofproducts to be consumed in the European Com-
[1] Evensen SA, Ulstrup J, Skaug K, Fr€
munity could be sold on the international market.
A, Rollag H. HIV infection in Norwegian haemophiliacs:
O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
the prevalence of antibodies against HIV in heamophiliacs
[12] Tollefsrud S, Noddeland H, Svennevig JL, Berntsen G,
treated with lyophilized cryoprecipitate from volunteer
Mollens TE, Solheim BG. Universal fresh frozen plasma
donors. Eur J Haematol 1887;39:44–8.
(Uniplasâ)––a safe product in open heart surgery, submit-
[2] Solheim BG, Heier HE, Evensen SA. Self-sufficiency for
blood and plasma products in Norway. Biol Clin Heamtol
[13] Rollag H, Solheim BG, Svennevig JL. Viral safety of blood
derivatives by immune neutralization. Vox Sang 1998;
[3] Retningslinjer for GMP i blodbanker. Statens helsetilsyns
veiledningsserie 1-1996. Oslo: Statens helsetilsyn; 1996.
[14] Nordbo A, Andersen A, Kongsgaard UE, Bormer OP,
[4] Nordoy I, Schrumpf E, Elgjo K, Flesland O, Andersen
Olsen H. Pharmaceutical-grade albumin: impared drug-
Glende J, Orjasaeter H, et al. Liver disease in anti-hepatitis
binding capacity in vitro, in preparation.
C virus-positive Norwegian blood donors. Scand J Gas-
[15] Haubelt H, Blome M, Kiessling AH, et al. Effects of
solvent/detergent-treated plasma and fresh-forzen plasma
[5] Aukrust P, Muller F, Svenson M, Nordoy I, Bendtzen K,
on haemostasis and fibrinolysis in complex coagulopathy
Fronland SS. Administration of intravenous immonolob-
following open-heart surgery. Vox Sang 2002;82:9–14.
ulin (IVIG) in vivo––down-reguolatory effects on the IL-1
[16] Mast AE, Stadanlick JE, Lockett JM, Dietzen DJ. Solvent/
system. Clin Exp Immunol 1999;115:136–43.
detergent-treated plasma has decreased antitrypsin activ-
[6] Gullestad L, Aass H, Fjeld JG, Wikeby L, Andreassen AK,
ity and absent antiplasmin activity. Blood 1999;94:3922–
Ihlen H, et al. Immunomodulating therapy with intrave-
nous immunoglobulin in patients with chronic heart
[17] Hellstern P, Sachse H, Schwinn H, Oberfrank K. Manu-
failure. Circulation 2001;103:220–5.
facture and in vitro characterization of solvent/detergent-
[7] Aukrust P, Gullestad L, Lappegard KT, Ueland T, Aass
treated human plasma. Vox Sang 1992;63:178–85.
H, Wikeby L, et al. Complement activation in patients with
[18] Beeck H, Hellstern P. In vitro characterization of solvent/
congestive heart failure: effect of high-dose intravenous
detergent-treated human plasma and of quarantine fresh
immunolglobulin treatment. Circulation 2001;104:1494–
frozen plasma. Vox Sang 1998;74(Suppl 1):219–23.
[19] Leebeek FWG, Schipperus MR, van Vliet HHDM. Coag-
[8] Solheim BG, Svennevig JL, Mohr B, Dragsund M,
ulation factors in solvent/dergent treated plasma. Transfu-
patients undergoing open heart surgery. In: M€
[20] Zeiler T, Wittmann G, Zimmermann R, et al. The effect of
virus inactivation on coagulation factors in therapeutic
DIC Pathogenesis and Disseminated Intravascular Fibrin
plasma. Br J Haematol 2000;111:986–7.
Formation. Amsterdam: Excerpta Medica, Elsevier Science
[21] Matsuda M, Wakabayashi K, Aoki N, Morioka Y. Alpha
2-plasmin inhibitor is among acute phase reactants.
[9] Solheim BG, Eggen BM, Heier HE. Self-sufficiency for
plasma and plasma proteins in Norway. In: Sibrowski W,
[22] Hart H, Jones A, Cubie H, McIntosh RV, Cuthbertson B.
Stangel W, Blauhut B, editors. Transfusionsmedizin 1995/
Distrubution of hepatitis A antibody over a process for the
96, vol. 33. Beitr Infusionsther Transfusionsmed; 1966. p.
preparation of a high-purity factor VIII concentrate. Vox
[10] Solheim BG, Rollag H, Svennevig JL, Arafa O, Fosse E,
[23] Wood DJ, Bird CR, Thorpe R, Barrowcliffe TW. Hepatitis
Bergerud U. Viral safety of solvent/detergent treated
A virus antibody levels in factor VIII concentrates. Lancet
plasma. Transfusion 2000;40:84–90.
[11] Noddeland H, Tølløfsrud S, Svennevig JL, Bentsen G,
[24] Cochrane Injuries Group Albumin Reviewers. Human
Brosstad F, Solheim BG. Universal solvent/detergent(SD)-
albumin administration in critically ill patients: systematic
treated plasma (Uniplasâ) rationale and clinical properties.
review of randomised controlled trials. BMJ 1998;317:235–
June 2009 Newsletter First Responders by Doug Brown How To Detect A Heart Attack Dizziness can be an early symptom of heart attack Cardiac chest pain is often vague, or dull, and may be described as a pressure or band-like sensation, squeezing, heaviness, or other discomfort. Pain is Not Always a Symptom of Heart Attack A heart attack often starts with mild symptoms that may not be
VI FIRST AID - HUMAN A. Initial Assessment - Assess for responsiveness by attempting to arouse the patient 1. Assess the airway - open mouth, examine and clear obvious obstructions 2. Assess for breathing - look, listen and feel 3. Assess for circulation - check pulse at neck (carotid artery), check for severe bleeding, treat for shock 4. Assume disability - cervical spine precautions,
 Transfusion and Apheresis Science 28 (2003) 93–100
The Norwegian plasma fractionation project––a
12 year clinical and economic success story
O. Flesland a,b,*, J. Seghatchian c, B.G. Solheim b
a Blood Bank, Baerum Hospital, N-1306 Barum, Norway
b Institute of Immunology, Rikshospitalet University Hospital, N-0027 Oslo, Norway
c Blood Component Technology and Thrombosis/Haemostasis Consultancy, 50 Primeroe Hill Road, London NW3 3AA, UK
The establishment of the Norwegian Fractionation Project (Project) was of major importance in preserving national
self-sufficiency when plasma, cryoprecipitate and small batch factor IX-concentrates were replaced by virus inactivatedproducts in the last part of the 1980s. Fractionation was performed abroad by contract with Octapharma after tenderson the European market. All Norwegian blood banks (>50) participated in the Project. Total yearly production was50–60 tons of mainly recovered plasma. From 1993 solvent detergent (SD) treated plasma has replaced other plasma fortransfusion.
Transfusion and Apheresis Science 28 (2003) 93–100
The Norwegian plasma fractionation project––a
12 year clinical and economic success story
O. Flesland a,b,*, J. Seghatchian c, B.G. Solheim b
a Blood Bank, Baerum Hospital, N-1306 Barum, Norway
b Institute of Immunology, Rikshospitalet University Hospital, N-0027 Oslo, Norway
c Blood Component Technology and Thrombosis/Haemostasis Consultancy, 50 Primeroe Hill Road, London NW3 3AA, UK
The establishment of the Norwegian Fractionation Project (Project) was of major importance in preserving national
self-sufficiency when plasma, cryoprecipitate and small batch factor IX-concentrates were replaced by virus inactivatedproducts in the last part of the 1980s. Fractionation was performed abroad by contract with Octapharma after tenderson the European market. All Norwegian blood banks (>50) participated in the Project. Total yearly production was50–60 tons of mainly recovered plasma. From 1993 solvent detergent (SD) treated plasma has replaced other plasma fortransfusion.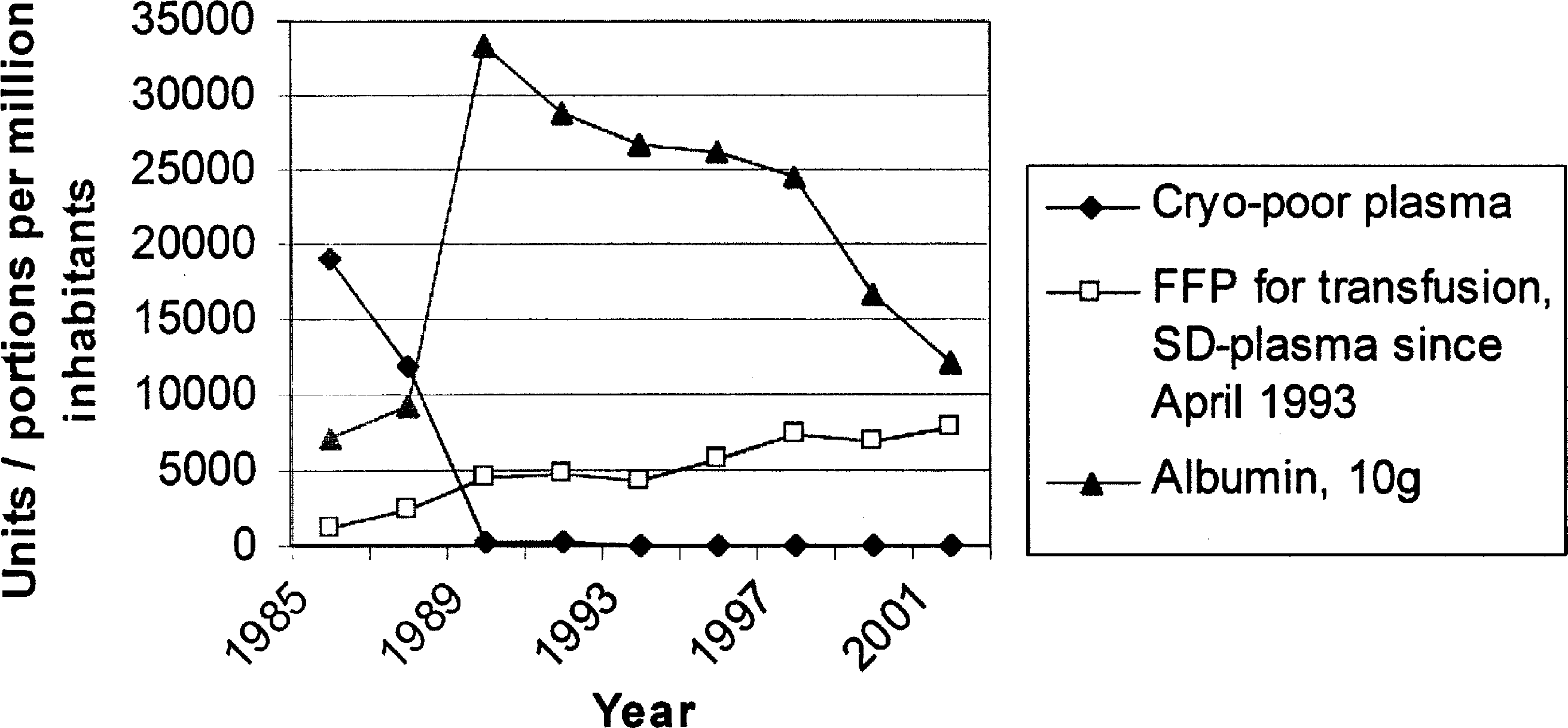 O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
Fig. 1. Plasma and albumin consumption in Norway from 1985–2001.
O. Flesland et al. / Transfusion and Apheresis Science 28 (2003) 93–100
Fig. 1. Plasma and albumin consumption in Norway from 1985–2001.