Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Untitled
ALCOHOLISM: CLINICAL AND EXPERIMENTAL RESEARCH
Hippocampus Volume Loss Due to Chronic Heavy Drinking
Thomas P. Beresford, David B. Arciniegas, Julie Alfers, Lori Clapp, Brandon Martin,
Yiping Du Dengfeng Liu, Dinggang Shen, and Christos Davatzikos
Objective: No clear consensus exists regarding the effect of sustained, heavy drinking on hippo-
campal volume. Our prior work hypothesized significantly lowered total hippocampus volumes inheavy chronically drinking alcohol-dependent (AD) subjects compared with light-drinking nonde-pendent control subjects matched for age and gender.
Method: Using a series of applicable exclusion criteria culled from previous published studies, we
measured hippocampal volumes from MRI scan data acquired on a 3T scanner and subjected thosedata to automated volume analysis blind to the drinking history.
Results: Comparison with AD test (n 5 8) and non-AD control (n 5 8) subjects found significant
lessening in total ( p 5 0.020) and left ( p 5 0.010) hippocampal volumes with a near-significant differ-ence on the right ( p 5 0.051). Linear regression demonstrated that neither total brain volume norintracranial volume affected the hippocampus measures.
Conclusions: These data support the view that heavy drinking exerts a unique and selectively
injurious effect on the hippocampus. Further study in larger samples must verify this in a search forpossible mechanisms of injury.
Key Words: Hippocampus, Alcohol Drinking, Volume Loss, MRI Scan.
THE EFFECT OF sustained, heavy drinking on convenience samples of heavy drinking and control sub-
hippocampal volume is a subject of continued contro-
jects (Beresford et al., 1999) led us to hypothesize that the
versy. Although some reports in the literature point to a
mean total hippocampus volume (THV) in the AD sub-
volumetric reduction in alcohol-dependent (AD) patients
jects would be significantly smaller than the mean THV in
(Bleich et al., 2003a; Sullivan et al., 1995), others are less con-
the non-AD control subjects. Our specific aim was to rep-
clusive (Agartz et al., 1999). Some have argued that lack of
licate the findings of the prior study but in prospectively
precise sample definition has generated this confusion, citing
gathered sample groups utilizing more stringent exclusion
inclusion of subjects with histories of withdrawal seizures
(Sullivan et al., 1996), for example. Others have disputed suchclaims (Bleich et al., 2003b).
With development project funding, we began a prospect-
ive study of the hippocampal volume in chronically
This project received prior approvals from our university institu-
tional review board (IRB) as well as from the Research and
drinking AD subjects. To assess volume comparisons at
Development Committee of our Department of Veterans Affairs
baseline, we analyzed new data from heavy-drinking AD
(DVA) facility where the study was conducted. All subjects were
test and light-drinking control cases. Early data from
voluntary and signed preapproved consent-for-study documents,consistent with IRB policy.
Medicine, Denver, Colorado (TPB); the Department of Psychiatry,
Both test (AD) and control subjects were adult male veterans who
University of Colorado School of Medicine, Denver, Colorado (TPB,
were eligible for care in the DVA system and were recruited in
DBA, JA, LC, BM, YD); the Department of Neurology, University of
response to posted flyers advertising the study. Our research design
Colorado School of Medicine, Denver, Colorado (DBA); the Depart-
matched AD test and non-AD control subjects for age, gender, and
ment of Radiology, University of Colorado School of Medicine, Denver,
ethnicity. Alcohol-dependent heavy drinkers qualified for study if
Colorado (YD); and the Department of Radiology, University of Penn-
sylvania, Philadelphia, Pennsylvania (DL, DS, CD).
Received for publication May 12, 2006; accepted July 28, 2006.
(1) Chronic heavy drinking: drank 5 or more standard drinks daily
This work was supported by Grant R21-AA14010 from the National
for at least 3 days weekly, and 3 weeks monthly for at least
Institute on Alcohol Abuse and Alcoholism.
9 months of the previous year, established through Time Line
Reprint requests: Thomas P. Beresford, MD, Denver VA Medical
Follow Back interview (Sobell et al., 1979);
Center (116), 1055 Clermont Street, Denver, CO 80220; Fax: 303-315-
(2) Recent heavy drinking: consumed 5 or more standard drinks
daily on at least 3 days weekly for the past 30 days, established
Copyright r 2006 by the Research Society on Alcoholism.
No claim to original US government works.
(3) AD diagnosis: fulfilled DSM-IV criteria for AD as established
through the Structured Clinical Interview for DSM-IV Axis I
Alcohol Clin Exp Res, Vol 30, No 11, 2006: pp 1866–1870
Disorders (Kessler et al., 2004; Peters et al., 1998; Sbrana et al.,
Pennsylvania who analyzed the MRI scan data blind to the subjects’
study group membership. The steps in image analysis included (1)
Similarly, non-AD light drinking comparison subjects presented
removal of extracranial tissues (skull-stripping); (2) tissue segmenta-
tion into gray matter (GM), white matter (WM), and cerebrospinalfluid (CSF); and (3) elastically warping a labeled atlas to all individ-
(1) o2 standard drinks daily for no more than 3 days weekly, 4
ual subjects, to label and measure automatically the regions of
weeks monthly for 9 months or less during the previous year and
interest in the brains. These steps are described briefly.
(2) Drinking less than 2 standard drinks daily no more than 3 days
(1) Skull stripping: A seed-based region growing procedure was
(3) None fulfilled DSM-IV criteria, either present or lifetime, for
applied first, which separates the brain parenchyma from extra-
cranial material (Goldszal et al., 1998). Manual editing was thenperformed on a slice-by-slice basis, which also removes the cere-
Candidates were excluded from study for SCID-verified psychi-
bellum. Comparison with original, unstripped scans at manual
atric illness: schizophrenia, major depressive disorder, bipolar
editing assures scan data quality for the next step. The interop-
disorder, posttraumatic stress disorder, or poly-substance depend-
erator reliability test revealed nonsignificant differences in the
ence (including concurrent antisocial personality disorder). Systemic
manual editing between the 2 trained operators. For 14 image
physical illness excluded those with any liver disease history, biliru-
sets evaluated, the mean within-subject difference between raters
bin above 1.2 mg/mL, ALT or AST above 200 U/L, Alcohol
was À0.02 Æ 1.37% for white matter and 0.46 Æ 0.88% for gray
Amnestic Syndrome history, HIV seropositivity, history of head
matter. Correlations were greater than 0.99 for both measures.
injury resulting in loss of consciousness, seizure disorder history
Finally, paired t-test comparisons yielded no significant differ-
including those caused by ethanol withdrawal, blood evidence of
folate or vitamin B-12 deficiency, dementia of any type, history of
(2) Tissue segmentation: The SPGR data are segmented into GM,
endocrine dysfunction (including Addison’s disease, Cushing’s
WM, and CSF (Goldszal et al., 1998). An automated segmenta-
disease, or exogenous steroid use within the past 5 years), and any
tion algorithm (Segal et al., 1995) based on k-means clustering
history of genetically based reactions to alcohol use (Asian ancestry
and Markov random fields, which has been validated extensively
with a history of the ethanol flush response). Alcohol-dependent
(Davatzikos and Resnick, 1998; Goldszal et al., 1998), is used at
subjects were excluded if withdrawal symptoms at the time of study
this step. This method also applies correction for magnetic field
(3) Automated measurement of brain structures: A labeled atlas is
transformed spatially into spatial coregistration with each
In this study, heavy-drinking subjects were required to provide a
tissue-segmented individual brain scan via an elastic warping
negative breath ethanol test administered by the study staff on the
algorithm (Davatzikos et al., 2001a, 2001b; Shen and Davatzi-
day of consent, the first day of the study protocol and again on the
kos, 2002, 2003), referred to as Hierarchical Attribute Matching
day of the first monitored disulfiram ingestion, as well as previous to
Mechanism for Elastic Registration (HAMMER), thus obtain-
each subsequent witnessed disulfiram administration. This was to
ing the automatic labeling of brain structures in each subject
assure (1) informed consent for study entry, that is, the absence of
brain. By calculating the total volume in each structure with
inebriation and (2) subject safety in disulfiram administration. The
identical label, the volumetric measurement for each brain struc-
MRI scan was performed within 3 days of the last reported alcohol
ture in each subject can be obtained. To achieve this, we first
use, within 4 days of the consent; breath alcohol testing was not
adopted a finely parcellated brain image as a labeled atlas devel-
required on the day of MRI scan. No subjects were scanned while
oped by Kabani and colleagues at the Montreal Neurological
obviously inebriated and none were observed in a disulfiram-ethanol
Institute (Kabani et al., 1998), including the hippocampal
reaction on the scan day. The 3-day limit for inclusion was designed
regions of interest (ROIs). Left and right hippocampi have sep-
to assure MRI study very early in the course of any structural healing
arate labels in this atlas. We then used a HAMMER registration
processes that might have begun with abstinence. All of the subjects
algorithm (Shen and Davatzikos, 2002, 2003) to warp this atlas
were ambulatory volunteers and none were inpatients at the time of
to each individual subject’s image, and thus obtain the auto-
study entry. Control subjects did not receive disulfiram, but reported
matic labeling of the ROIs in each subject and further obtain
negative alcohol use histories at the time of study entry (TLFB) and
their volumetric measurements by computing the volume in each
offered no evidence of intoxication.
labeled ROI. When computing the volume in each labeled ROI,all voxels, whether they are gray matter voxels or white matter
voxels, were counted. Figure 1 shows the automatically labeledhippocampus in representative control and AD subjects. The
All entered subjects completed a baseline 3T-MRI brain scan.
accuracy of the HAMMER registration algorithm has been
Scan data were collected through whole brain-volume acquisition
extensively validated by both real data and simulated data (Shen
using a 3D inversion-recovery spoiled grass (IR-SPGR) pulse
sequence in the coronal plane with an image matrix
256Â192Â124 on a 3T-MRI scanner (General Electric Company,Milwaukee, WI). The image resolution was 0.94Â0.94Â1.7 mm3,
with a lower resolution along the anterior/posterior direction. The
Scan-derived volumetric measurement data acquired in blinded
inversion time of 450 ms was selected to optimize the gray/white
fashion were analyzed for test or control group membership. Differ-
matter contrast. The data acquisition time for the 3D volume was 13
ences in AD test versus non-AD control group means in total
(combined), right, and left hippocampal mean volumes, respec-tively, were compared and assessed for statistical significance using
Student’s t-test of the means for samples with differing variances.
Hippocampal, total brain, and intracranial volumes (ICVs) were
Significance was set at 0.05 in a one-tailed test as indicated by the a
derived using an automated segmentation process on the 3T-MRI
priori prediction of the direction of mean values. We conducted a
images of the brain (Shen and Davatzikos, 2002). These were
secondary analysis using multiple linear regressions to include
assessed by an imaging analysis research group at the University of
potential confounding variables. These included total brain volume
Fig. 1. Labeled hippocampus in representative subjects: control subject (left) and heavy-drinking subject (right).
(TBV) and ICV measures to assess the possible effects of individual
criteria for a substance-related diagnosis: past alcohol abuse (the
variations in brain and calvarium volumes. In this analysis, TBV is
abuse occurred over 30 years before study entry).
the sum of all white matter, gray matter, and ventricular CSF, whileICV is the total volume inside the skull. If no confounding variableswere identified at the 0.1 level of probability, they were removed
from analysis. If no variables remained, the model was reduced to a
simple t-test of the means. As a convergent analysis, we conductedpartial correlation coefficient (PCC) tests between THV and TBV
As shown in Table 1, the total (p 5 0.02) and left
(p 5 0.01) mean volumes were significantly smaller in theAD heavy drinkers than in the light-drinking, non-AD
controls. The right hippocampus mean difference narrowlymissed significance (p
From a total of 54 screened cases (35 test and 19 control), we
accrued a sample of 18 matched subjects who proceeded to MRI
ed independently, mean measures of TBV and ICV each
scan: 9 AD test and 9 non-AD control. The most common reasons
differed significantly between the 2 groups (Student’s t-test,
for failing study qualification included stopping drinking more than
2 tails). The mean TBV was 917.4 Æ 98.1 mL in the alcohol
3 days before study, medical illness exclusion, and presence of Axis I/
group versus 1,040.5 Æ 74.3 mL in the control group
II disorders mentioned above. Two subjects, 1 from each group, were
removed from final data analysis because of potentially significant
5 0.014). The mean ICV was 1,024.4 Æ 104.1 mL among
anatomic abnormalities on the MRI scans that were not regarded as
the drinkers versus 1,162.1 Æ 96.9 mL among the control
related to alcohol use and that indicated clinical referral (evidence of
previous anoxic injury and congenital malformation, respectively). Both subjects were Caucasians; dropping them did not affect eitherage or ethnic distribution. Data were analyzed from the remaining
Because the data sufficiently fit a normal distribution
and did not require any transformation, we proceeded to
multiple linear regression analysis. Drinking status was
Owing to the matching procedure, the mean subject age was
forced into the model during backward stepwise regression
equivalent between groups: AD-test group 47.25 Æ 10.71 years,
to assess our primary scientific question at all times. To
non-AD control group 47.75 Æ 10.78 years. There were 7 Cau-
evaluate whether hippocampus volumes were related to
casians and 1 African American in each group. Within the
brain or calvarium size, TBV and ICV measures were
heavy-drinking group, the subjects’ reported average number of
tested in the regression model as covariates. In the
total drinks in the 30 days before study entry was 392 Æ 259 stand-ard drinks; however, the average alone is somewhat misleading. Of
multivariate model for each side of the hippocampi,
the 8 heavy drinkers, 5 drank daily and 3 drank during binges that
neither covariate contributed significantly (right hippo-
lasted 3 to 4 days weekly. For perspective, all drank an average of
campus, p 5 0.42, p 5 0.65, respectively; left hippocampus,
16 Æ 7 standard drinks on those days when they drank.
By contrast, the control subjects reported far less alcohol exposure
Table 1. Mean Hippocampal Volumes (mean mL Æ SD)
in the prior 30 days. The 8 of them reported a total intake of24 standard drinks for the previous 30 days, an average of 3.0 Æ3.3 standard drinks each for the entire month, or about 0.75 Æ 0.8
standard drinks per person weekly. The range was 0 to 8 drinks
during the month. Of the 8 test subjects, 1 subject met SCID criteria
for current cannabis abuse but not dependence; 1 met criteria for
current stimulant abuse but not dependence; and 1 met criteria for
current cocaine dependence. None of the 8 control subjects met cri-teria for current dependence or abuse of any substance; only 1 met
p 5 0.25, p 5 0.46, respectively). When the total hippo-
this sample includes no female subjects and some reports
campal volume was considered, neither TBV nor ICV
suggest that gender may be a confounding factor in any
significantly contributed to the model (p 5 0.31, p 5 0.53,
comparison with male and female AD drinkers (Pfeffer-
respectively) when drinking status was included. With
baum et al., 2001; Gianoulakis et al., 2003). Other possible
volume covariates showing no effect, we concluded that
variables of interest were not recorded including handed-
Student’s t-test was the appropriate statistic for assessment
ness, socioeconomic status, or body size. Our previous
of between-group hippocampus volumes measures.
research (Lucey et al., 1999), however, casts doubt as to
Using the whole sample (n 5 16), we calculated the par-
whether body size is a contributing variable in a design
tial correlation coefficients (PCC) between THV and TBV,
controlling for age and gender. Finally, this study did not
as well as THV and ICV, controlling for drinking status as
address any possible secondary molecular effects from
either a heavy or a light drinker. We found no association
high ethanol exposure (Bleich et al., 2003a).
between THV and either variable: for total brain volume,
The test subjects in this study were seen in middle age
PCC 5 0.281, p 5 0.31; for intracranial volume, PCC 5
after long, heavy-drinking careers. Although a recent
report found that adolescents with alcohol use disorderswho are free of psychiatric comorbidities experience areduction in the left hippocampus (Nagel et al., 2005), our
data offer no comment on heavy, sustained drinking at an
The data presented here support the hypothesis that
earlier age, for example, binge drinking in young adults
chronic, heavy drinking of ethyl alcohol is associated with
when the course of heavy drinking is comparatively early.
reduced THV and that observed volume reductions are
Future directions suggested by this line of research
likely independent of total brain and intracranial volumes.
include enlarging the sample beyond middle-aged, male,
Although the data are derived from a relatively small
DVA subjects in an effort to arrive at more generalizable
sample, the subjects represent a group selected to be
conclusions. Future replication study should include a
free of variables previously reported as potentially con-
wider sampling of heavy drinking men and a large sample
founding volumetric MRI data—the exclusion criteria
of heavy-drinking women. If the data continue to suggest
listed above. As a result, we offer these results as clearly
THV lessening, studies at earlier points in the drinking
implicating an injurious role of chronic heavy ethanol use
career—such as in heavy-drinking adolescents—as well as
in specific minority groups would be indicated. The data
For an added perspective, we construed the group mean
observed here relate only a cross-sectional view of THV
differences as a drug effect of ethanol. The calculated
and raise the importance of recording the natural history
effect difference in THV between the AD and control
of hippocampus volume change, if any, over the course of
groups yielded Cohen’s d 5 1.1. For left and right hippo-
abstinence from ethanol. While the present report suggests
campus volumes, d 5 1.3 and 0.9, respectively. Cohen’s
injury to the hippocampus, injuries are often capable of
statistic defines effect sizes as large equaling 0.6 to 0.8 or
healing in a healthy environment. It is our hope, as well, to
greater, medium 0.3 to 0.5, and small 0.0 to 0.2 (Cohen,
explore this in serial, controlled MRI studies of active AD
1988). The large effect size in this case appears best attrib-
uted to the difference in drinking status between these 2groups. As a comparison for discussion purposes, wecalculated this statistic from the reported effect data ofnaltrexone on days abstinent as reported in a recent
multicenter trial (Anton et al., 2006). Those data yielded
Agartz I, Momenan R, et al (1999) Hippocampal volume in patients with
d 5 0.24, only a small effect. In the same study, medical
alcohol dependence. Arch Gen Psych 56:356–363.
management without the study medication resulted in
Anton RF, O’Malley SS, et al (2006) Combined pharmacotherapies and
behavioral interventions for alcohol dependence: the COMBINE
d 5 0.49, a medium effect. By contrast, the effect of
study; a randomized controlled trial. JAMA 295:2003–2017.
ethanol that we observed in reducing THV appears to be
Beresford T, Arciniegas D, et al (1999) Hippocampal to pituitary volume
ratio: a specific measure of reciprocal neuroendocrine alterations in
This study has several limitations that prevent general-
alcohol dependence. J Studi Alcohol 60:586–588.
ization to all heavy, sustained users of alcohol. As
Bleich S, Bandelow B, et al (2003a) Hyperhomocysteinemia as a new risk
factor for brain shrinkage in patients with alcoholism. Neurosci Lett
mentioned, the data presented from a small and highly
select sample gathered to establish that hippocampus vol-
Bleich S, Sperling W, et al (2003b) Lack of association between hippo-
ume loss can be reliably observed. The small sample size
campal volume reduction and first-onset alcohol withdrawal seizure.
may have to do with the smaller mean ICV that we
observed in the drinking subjects; while previous research
Cohen J (1988) Statistical Power Analysis for the Behavioral Sciences.
Lawrence Earlbaum Associates, Hillsdale, NJ.
strongly suggests lessened mean TBV in heavy drinkers, no
Davatzikos C, Genc A, et al (2001a) Voxel-based morphometry using the
reports in our awareness note lessened ICV as a general
RAVENS maps: methods and validation using simulated longitudinal
characteristic in a single gender sample. Concomitantly,
Davatzikos C, Li HH, et al (2001b) Accuracy and sensitivity of detection
Pfefferbaum A, Rosenbloom M, et al (2001) Sex differences in the
of activation foci in the brain via statistical parametric mapping: a
effects of alcohol on brain structure. Am J Psychiatry 158:
study using a PET simulator. Neuroimage 13:176–184.
Davatzikos C, Resnick SM (1998) Sex differences in anatomic measures
Sbrana A, Dell’Osso L, et al (2003) Acceptability, validity and reliability
of interhemispheric connectivity: correlations with cognition in men
of the Structured Clinical Interview for the Spectrum of Substance
but not in women. Cereb Cortex 8:635–640.
Use (SCI-SUBS): a pilot study. Int J Methods Psychiatri Res 12:
Gianoulakis C, Dai X, et al (2003) Effect of chronic alcohol consumption
on the activity of the hypothalamic-pituitary-adrenal axis and pituit-
Segal DL, Kabacoff RI, et al (1995) Update on the reliability of diagnosis
ary beta-endorphin as a function of alcohol intake, age, and gender.
in older psychiatric outpatients using the structured clinical interview
of DSM IIIR. J Clin Geropsychol 1:313–321.
Goldszal AF, Davatzikos C, et al (1998) An image processing protocol
Shen D, Davatzikos C (2002) HAMMER: Hierarchical attribute match-
for the analysis of MR images from an elderly population. J Comput
ing mechanism for elastic registration. IEEE Trans Med Imaging
Kabani N, MacDonald D, et al (1998) A 3D atlas of the human brain.
Shen DG, Davatzikos C (2003) Very high resolution morphometry using
mass-preserving deformations and HAMMER elastic registration.
Kessler RC, Abelson J, et al (2004) Clinical calibration of DSM-IV diag-
noses in the World Mental Health (WMH) version of the World
Sobell LC, Maisto SA, et al (1979) Reliability of alcohol abusers’ self-
Health Organization (WHO) Composite International Diagnostic
reports of drinking behavior. Behav Res Therapy 17:157–160.
Interview (WMHCIDI). Int J Methods Psychiatric Res 13:122–139.
Sullivan EV, Marsh L, et al (1995) Anterior hippocampal volume deficits
Lucey MR, Hill EM, et al (1999) The influences of age and gender on blood
in nonamnesic, aging chronic alcoholics. Alcohol Clin Exp Res
ethanol concentrations in healthy humans. J Stud Alcohol 60:103–110.
Nagel BJ, Schweinsburg AD, et al (2005) Reduced hippocampal volume
Sullivan EV, Marsh L, et al (1996) Relationship between alcohol with-
among adolescents with alcohol use disorders without psychiatric
drawal seizures and temporal lobe white matter volume deficits.
comorbidity. Psychiatry Res 139:181–190.
Peters RH, Greenbaum PE, et al (1998) Prevalence of DSM-IV substance
Ventura J, Liberman RP, et al (1998) Training and quality assurance
abuse and dependence disorders among prison inmates. Am J Drug
with the Structured Clinical Interview for DSM-IV (SCID-I/P).
Trans fats clean out—Pantry Products we found that contain trans fat Substitution suggestions (just a few ideas that can be found in mainstream *See ingredient information below; we’ve stores. Good brands can also be found at Betty Crocker Fruit Roll-Ups Strawberry Sensation Chef Boyardee Microwave Macaroni & Cheese* -Annie’s homegrown macaroni and cheese (options for s
Editorials represent the opinions of the authors and JAMA and not those of the American Medical Association. Vitamin E, Memantine, and Alzheimer DiseaseDenis A. Evans, MD; Martha Clare Morris, ScD; Kumar Bharat Rajan, PhD The report by Dysken et al1 in this issue of JAMA raises inter- to support its use because the comparison of the groupesting issues about drug therapy for Alzheimer dise
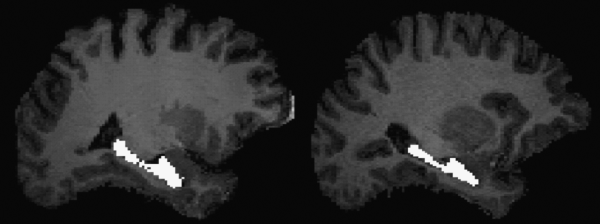 Fig. 1. Labeled hippocampus in representative subjects: control subject (left) and heavy-drinking subject (right).
Fig. 1. Labeled hippocampus in representative subjects: control subject (left) and heavy-drinking subject (right).