Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Chirurgia 1 dap_c 4'2006 a.qxd
Chirurgia (2011) 106: 127-129Nr. 1, Ianuarie - FebruarieCopyright Celsius
Parathyroid cysts, a rare condition: a case report and review of the literature C. Codreanu1, C.M. Codreanu2
1ENT Department, Galaåi County Hospital, Galaåi2Lariboisiere Hospital, ENT Department, Paris, France
(adenomatous) forms, the last one being responsible of hyper-parathyroidism. We report a case of nonfunctioning sympto-
Chisturile paratiroidiene, o situaåie clinicã rarã: prezentare
matic parathyroid cyst in a 36-year old woman revealed by an
de caz æi discuåii
anterior cervical tumefaction focusing on the pre-operative
Chisturile paratiroidiene reprezintã o adevãratã încercare diagnosis and the management of it regarding the various clinicã æi terapeuticã pentru medicul practician. De cele mai
therapeutic methods described in the literature.
multe ori, dimensiunile acestora sunt mici, de câåiva milimetriîn diametru, deæi uneori pot atinge dimensiuni centimetrice. În
Key words: parathyroid, cyst, case report
funcåie de activitatea secretorie, existã 2 tipuri de chisturi:forme clinice nonfuncåionale (esenåiale) æi forme funcåionale(adenomatoase), ultimile fiind responsabile de hiper-paratiroidism. Autorii prezintã în acest articol un caz clinic de
Introduction
chist paratiroidian nonfuncåional, simptomatic, la o pacientãde 36 de ani, prezentându-se clinic ca o tumefacåie cervicalã
Parathyroid cysts are rare neck tumours. Though they were
anterioarã. Sunt expuse de asemenea metodele de diagnostic
discovered in 1880 by Sandstrom and excised for the first time
preoperator æi conduita terapeuticã actualã.
in 1906 by Goris, only about 250 cases were described in theliterature by now. These cysts usually occur during the fourth
Cuvinte cheie: paratiroidã, chist, prezentare de caz
and fifth decade of life and are defined in relation to theirparathyroid hormone(PTH) secretion capacity: nonfunctioning(essential) and functioning (adenomatous) types. The non-functioning types ( 80% of cases) are more common in females,
Abstract
while the functioning types are more common in males. (1) A
Parathyroid cysts are a rare medical condition, that is why they
single case of malignant transformation has been described. (2)
represent a diagnostic and therapeutic challenge for the
The non-functioning parathyroid cysts’ origin is still
practitioner. The cysts are often small in diameter, measuring a
under debate and there are several hypotheses to explain
few millimeters, but in some cases they are centimetric in size.
There are 2 types of parathyroid cysts, according to their
- forms resulting from the fusion of small cavities within
activity: the nonfunctioning (essential) and the functioning
- vestigial cysts resulting from the 3rd and 4th branchial
- pseudocysts caused by the parathyroid’s necrosis,
containing high levels of PTH but not accompanied
Corneliu Codreanu MDENT Department, Galaåi County Hospital
by an increase of plasma levels of the hormone.
The functioning parathyroid cysts’ origin is generally
accepted as the result of cystic degeneration of a parathyroidadenoma.
In most cases the parathyroid cysts are asymptomatic (3).
Sometimes the cysts are revealed by a tracheal or recurrentnerve compression (4). The symptoms associated with theadenomatous cysts are related to excessive secretion of PTH.
Physical examination usually shows a soft, mobile swelling
often located at the inferior pole of the thyroid. There are casesof multiple cysts described and even cysts developed at othercervical and mediastinal levels (5,6). Cervical ultrasonography(US), followed in some cases by computer tomography (CT) andmagnetic nuclear resonance (MRI) shows a cystic, juxtathyroidswelling with paper-thin walls. The differential diagnosisincludes a thyroid cyst, a parathyroid cyst and a branchial cyst. The diagnostic dilemma can be solved after the fine-needleaspiration of the cyst and examination of the intracystic fluid. In parathyroid cysts it is a watery, colourless, acellular liquid,with high levels of PTH for both nonfunctioning and func-tioning types (3,4,7). PTH in the cystic fluid is almost entirelyin the form of the non-active C-terminal fragment, since PTHis rapidly broken down. In the adenomatous forms, there arethe same high PTH levels in the cystic fluid but in addition the
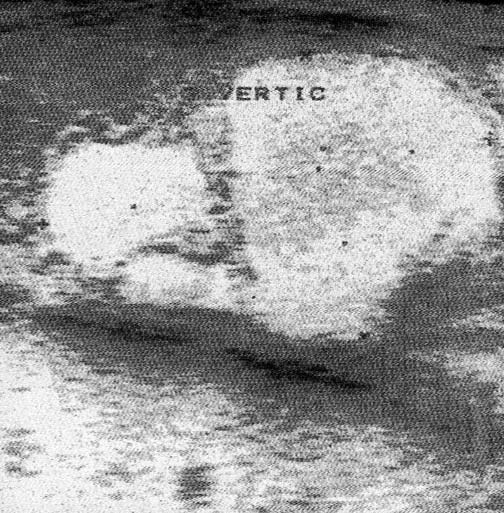
Figure 1. Cervical ultrasonography. Hypoechoic formation with
serum PTH (active) levels are high due to secretion by the
well defined margins in close contact with the posteriorpart of the right thyroid lobeCase report D.M., a 36-year old female with no particular antecedents,presented in our department in 2008 with a 3-year history ofanterior cervical tumefaction, located at the inferior pole ofthe right thyroid lobe. The patient accused a discrete dysphagia and dispnoea upon effort. The tumefaction wasroundish, soft, about 3,5 cm in diameter, not painful duringpalpation. Laryngoscopic findings were normal.Cervical US showed a hypoechoic, oval-shaped formationwith well defined margins and thin walls, in close contact withthe posterior part of the right thyroid lobe (Fig. 1).The thyroid gland hormones` levels were normal as wellas the phosphocalcic metabolism markers. The serum PTHlevel was 28,8 pg/mL (normal values 11-47 pg/mL).Fine needle-aspiration of the cervical tumefactionrevealed 10 ml of clear, acellular liquid. The biochemicalFigure 2. View during surgical removal of the cyst. Parathyroid study of the liquid showed high levels of PTH ( 426 pg/mL). cyst located at the level of the inferior right parathyroid3 weeks after the treatment by fine-needle aspiration, thepatient returns with the same cervical tumefaction that seemsto be greater in size than previously. We decide the surgicalmanagement of the tumefaction under general anesthesia. Thelater with no clinical or ultrasonographic evidence ofcyst located at the level of the inferior right parathyroid waseasily dissected without opening the capsule and then removedalong with the right inferior parathyroid gland (Fig. 2).Discussion The surgical specimen measured 57 x 30 x 24 mm.Histological examination showing a parathyroid cyst with a
Although parathyroid cysts were found in 42 cases from 100
capsule adhering to the parathyroid parenchyma and
autopsies by Black and Watts (8) suggesting a quite frequent
fibroadipose tissue, along with previous laboratory tests con-
pathology this is the only documented case of parathyroid
cluded of a non-functioning parathyroid cyst.
cyst managed in our department in a 10-year period.
Postoperative care was simple, the patient leaving the
In 1979, Calandra and al. (9) found 11 (3,38%) functional
hospital the next day. The patient was examined 3 months
parathyroid cysts among 325 patients hospitalized in the
surgery department for hyperparathyroidism. In another 2.
Uwents P, Debruyne F, Delaere P, Ostyn F. le kyste parathyroi-
article, Clark (10) reviews this particular pathology and finds
dien, une cause de tumefaction de la region du cou. Rev
out in the literature that among 96 parathyroid cysts there were
Laryngol Otol Rhinol. 1994;115:113-115.
Ginsberg J, Young JEM, Walfish PG. Parathyroid cysts, med-ical diagnosis and management. JAMA. 1978;240(14):1506-7.
Our case highlights the management of a non-functional
Alvi A, Myssiorek D, Wassennan P. Parathyroid cyst: current
parathyroid cyst taking into consideration the more recent
diagnostic and management principles. Head Neck. 1996;
reports in the literature, beginning with a cervical ultrasono-
graphy and a fine-needle aspiration of the cystic fluid for the
Haid SP, Method HL, Beal JM. Parathyroid cysts. Report of
cytological assessment. In case of a clear, acellular, colorless
two cases and a review of the literature. Arch Surg.
fluid one must be aware of the possibility of a parathyroid cyst.
Also, the high levels of PTH in the fluid are in correlation
Gurbuz AT, Peetz ME. Giant mediastinal parathyroid cyst: an
with this diagnosis whatever the type of the cyst. Moreover,
unusual case of hypercalcemic crisis. Case report and review of
laboratory tests reveal if the cyst is nonfunctioning (normal
the literature. Surgery. 1996;120(5):795-800.
Pacini F, Antonelli A, Lari R, Casperini L, Baschieri L, Pinchera
PTH, calcium and phosphorous serum levels - as in our case)
A. Unsuspected parathyroid cysts diagnosed by measurement of
or functioning (high serum levels of PTH, calcium and
thyroglobulin and parathyroid hormone concentrations in fluid
aspirates. Ann Intern Med. 1985;102(6):793-4.
Fine-needle aspiration leads frequently to a relapse in 2
Black BM, Watts CF. Cysts of parathyroid origin; report of two
cases out of 4 in one month time in Prinz et al.’s experience
cases and study of incidence and pathogenesis of cysts in
(11) and in 2 cases out of 12 in Shi’s experience (12). Some
parathyroid glands. Surgery. 1949;25(6):941-9.
authors (13) suggest a tetracycline injection in the cyst as an
Calandra DB, Shah KH, Prinz RA, Sullivan H, Hofmann C,
alternative to the surgical treatment, but this method has a
Oslapas R, et al. Parathyroid cysts: a report of eleven cases
high risk of cyst’s wall rupture followed by intense cervical
including two associated with hyperparathyroid crisis. Surgery. 1983;94(6):887-92.
pain (14,15) or even recurrent laryngeal nerve palsy (16).
10. Clark OH. Parathyroid cysts. Am J Surg. 1978;135(3):395-402.
In case of a nonfunctioning cyst, Clark suggests the surgical
11. Prinz RA, Peters JR, Kane JM, Wood J. Needle aspiration of
management of the cyst after the first relapse of the ultra-
nonfunctioning parathyroid cysts. Am Surg. 1990;56(7):420-
sonography-guided fine-needle aspiration,in case of patients
complaining of significant symptoms or in case of other 12. Shi B, Guo H, Tang N. Treatment of parathyroid cysts withlocations (mediastinal, retromandibular). In case of a function-
fine-needle aspiration. Ann Intern Med. 1999;131(10):797-8.
ing cyst the surgical excision of the cyst is always indicated as
13. Sánchez A, Carretto H. Treatment of a nonfunctioning
parathyroid cyst with tetracycline injection. Head Neck.
New techniques such as minimally invasive endoscopic
14. Ryan WG, Dwarakanathan A. Minor complication of thyroid
parathyroidectomy represent an alternative to the classic
cyst sclerosis with tetracycline. Arch Intern Med. 1986;146(1):
surgical approach and are yet to be evaluated.
15. Okamura K, Ikenoue H, Sato K, Yoshimin M, Nakagawa M,
References
Kuroda T, et al. Sclerotherapy for benign parathyroid cysts. Am J Surg. 1992;163(3):344-5.
Mevio E, Gorini E, Sbrocca M, Artesi L, Mullace M, Lecce S.
16. Treece GL, Georgitis WJ, Hofeldt FD. Resolution of recurrent
Parathyroid cysts: description of two cases and review of the
thyroid cysts with tetracycline instillation. Arch Intern Med.
literature. Acta Otorhinolaryngol Ital. 2004;24(3):161-4.
1Department of Nephrology and Dialysis and 2University Department of Medicine, Sestre milosrdnice University Hospital,SUMMARY Drug dialyzability is determined by complex interaction of many factors, including the char-acteristics of the drug and the technical aspects of the dialysis system. Numerous aspects of dialysis pre-scription, including some elaborated in this article, have the potent
For the use only of Physician, Gynaecologist, Oncologist, Leuprolide Acetate for Injection 11.25 mg (Depot) LUPRODEXTM 11.25 mg (3 months Depot) Lyophilized For Intramuscular / Subcutaneous use For Single use only Not for Intravenous Administration DESCRIPTION: LUPRODEXTM (DEPOT) 11.25 mg is a sterile lyophilized containing Leuprolide Acetate formulated as Microspheres.
 accepted as the result of cystic degeneration of a parathyroidadenoma.
accepted as the result of cystic degeneration of a parathyroidadenoma.