Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Microsoft word - vesanoid_pm_20aug2007.doc
PRODUCT MONOGRAPH VESANOID®
®Registered Trade-Mark of Hoffmann-La Roche Limited
Copyright 1994-2007 Hoffmann-La Roche Limited
PRODUCT MONOGRAPH NAME OF DRUG VESANOID® DIFFERENTIATION INDUCING AGENT ALL-TRANS RETINOIC ACID SHOULD BE ADMINISTERED TO PATIENTS WITH ACUTE PROMYELOCYTIC LEUKEMIA (APL) ONLY UNDER THE SUPERVISION OF A PHYSICIAN EXPERIENCED IN THE TREATMENT OF HEMATOLOGICAL ONCOLOGICAL DISEASE (SEE WARNINGS). ACTIONS AND CLINICAL PHARMACOLOGY
All-trans retinoic acid is a natural metabolite of retinol and belongs to the class of compounds known as retinoids, which are structurally related to vitamin A and comprise natural and synthetic analogs. In vitro studies with all-trans retinoic acid have demonstrated induction of differentiation and inhibition of cell proliferation in transformed hemopoietic cell lines, including human myeloid leukemia cell lines.
Acute promyelocytic leukemia (APL) is associated with a non-random chromosomal abnormality characterized by balanced and reciprocal translocations between the long arms of chromosomes 15 and 17 [t(15;17)(q22;q21)]. The gene encoding the retinoic acid receptor-alpha (RAR-α) is located on chromosome 17. A previously unidentified gene, PML, that may act as a transcription factor, is located on chromosome 15. The 15;17 translocation fuses the genes for PML and RAR-α, resulting in the synthesis of two reciprocal fusion transcripts, PML/RAR-α (found in all patients) and RAR-α/PML (found in about 2/3 of patients). PML/RAR-α may inhibit the differentiation of myeloid cells, resulting in carcinogenesis, an effect which may be overcome by the use of high doses of all-trans retinoic acid. Orally administered all-trans retinoic acid induces a high rate of complete remissions in patients with APL.
PHARMACOKINETICS
All-trans retinoic acid is an endogenous metabolite of vitamin A and is normally present in plasma at concentrations of 2 to 4 ng/mL. All-trans retinoic acid is transported directly via the portal system rather than through the lymphatics and thus absorption does not require specific transport mechanisms. All-trans retinoic acid is highly lipophilic with more than 95% of total drug concentration bound to plasma proteins. All-trans retinoic acid is primarily metabolized by liver enzymes and is converted to the 13-cis isomer. Oxidation by P450 isoenzymes leads to the corresponding 4-hydroxy and 4-oxo-compounds. After glucuronidation, these metabolites are excreted in the urine and bile.
Vesanoid®
Page 3
Following a single dose of radiolabelled all-trans retinoic acid, about 30% of the total radioactivity was recovered in the feces and about 60% in the urine. Nearly the entire dose was excreted within 3 to 6 days.
Single Dose: The pharmacokinetics of all-trans retinoic acid were investigated in healthy volunteers following a single oral dose of 40 mg of all-trans retinoic acid and in patients with acute promyelocytic leukemia (APL) treated with 45 mg/m2. Maximum plasma concentrations of all-trans retinoic acid were reached within one to two hours in the APL patients and within 3 to 4 hours in the healthy volunteers. Large intersubject variability was observed. Plasma concentrations declined mono-exponentially with a mean elimination half-life of 0.71 hours. Endogenous levels (2 to 4 ng/mL) were reached 7 to 12 hours after dosing. Multiple Doses: Multiple oral doses of all-trans retinoic acid were associated with a significant (about 2 fold) decrease in both the peak plasma levels and the AUC levels, after 2-6 weeks of treatment. These changes were associated with a 10 fold increase in urinary excretion of 4-oxo all-trans retinoic acid glucuronide.
The administration of ketoconazole, an inhibitor of the P450 enzyme system, after multiple doses of all-trans retinoic acid, resulted in a greater mean plasma all-trans retinoic acid AUC than after the administration of all-trans retinoic acid alone.
Pharmacokinetics in Pediatric Patients: A phase I trial of all-trans retinoic acid administered orally twice-daily for treatment courses of 28 days was performed in pediatrics. Cohorts of at least 3 patients were entered at successive all-trans retinoic acid dose levels (from 45 to 80 mg/m2/day, with a twice a day dosing regimen) until dose-limiting toxicity was consistently observed. Twenty-one patients with a median age of 14 years and various types of tumours including 2 patients with APL were entered into the trial.
Pharmacokinetics were determined in eighteen patients on day one and in seven patients in day 1 and day 28. Time to peak plasma concentrations was between 1 and 4 hours after dosing. Peak plasma concentrations of all-trans retinoic acid of 0.59, 0.62 and 1.64 μM (180, 190 and 490 ng/mL) were observed following doses of 22.5, 30 and 40 mg/m2. AUC values for these doses were 1.29, 1.13 and 3.35 μM (387, 339 and 1005 ng.h/mL), respectively. Peak plasma concentrations and AUC values did not appear to increase in proportion to dose. A greater than three-fold increase in AUC was observed following a 30% increase in dose (30 to 40 mg/m2). The average terminal half-life was 0.7 hours. The AUC on day 1 was significantly greater than the AUC on day 28 (mean decrease 78% ± 30 SD). Quantifiable concentrations of 4-oxo metabolites of all-trans retinoic acid were not observed.
Pharmacokinetics in renal and hepatic impairment The pharmacokinetics of all-trans retinoic acid in patients with compromised kidney or liver function have not been studied. INDICATIONS AND CLINICAL USE
‘Vesanoid’ (all-trans retinoic acid) may be used for the induction of remission in acute promyelocytic leukemia (APL; FAB classification AML-M3). Previously untreated patients, as well as patients who relapsed after, or were refractory to, standard chemotherapy (daunomycin and cytosine arabinoside or equivalent therapies) may be treated with all-trans retinoic acid. Upon achievement of complete remission, full-dose consolidation chemotherapy should be employed. Among patients maintained on all-trans retinoic acid, a loss of responsiveness to all-trans retinoic acid, has been reported, with a median time to relapse of 4-6 months.
Vesanoid®
Page 4 CONTRAINDICATIONS
‘Vesanoid’ (all-trans retinoic acid) is highly teratogenic; therefore it is contraindicated during pregnancy and in nursing mothers. ‘Vesanoid’ must not be used by women of child-bearing potential unless effective contraception is practiced for at least one month before beginning therapy, during therapy and at least one month following discontinuation of therapy.
‘Vesanoid’ is contraindicated in patients with a known hypersensitivity to all-trans retinoic acid or related compounds.
The use of all-trans retinoic acid in combination with vitamin A is contraindicated (see PRECAUTIONS, Drug Interactions).
WARNINGS
All-trans retinoic acid should be administered to patients with APL only under the strict supervision of a physician who is experienced in the treatment of hematological / oncological diseases.
PREGNANCY: Pregnancy: All-trans retinoic acid is highly teratogenic. Its use is contraindicated in pregnant women and women who might become pregnant during or within one month of the cessation of treatment. There is an extremely high risk that a deformed infant will result if pregnancy occurs while taking all-trans retinoic acid, irrespective of the dose or duration of the treatment. Potentially all exposed fetuses can be affected. Therapy with all-trans retinoic acid should only be started in female patients if each of the following conditions is met:
The patient is suffering from life threatening malignancies. She is informed by her physicians of the hazards of becoming pregnant during and within one month after treatment with all-trans retinoic acid.
She is willing to comply with the mandatory contraception measures.
Every woman of child-bearing potential who is to undergo treatment with all-trans retinoic acid uses effective contraception for four weeks before, during and for one month after discontinuation of treatment with all-trans retinoic acid.
Therapy should not begin until the second or third day of the next normal menstrual period.
A negative pregnancy test result must be obtained within the two weeks before commencement of treatment. It is advisable to perform additional pregnancy tests at monthly intervals during therapy.
Should pregnancy occur, in spite of these precautions, during treatment with all-trans retinoic acid or within one month after its discontinuation, there is a high risk of severe malformation of the fetus particularly when all-trans retinoic acid was given during the first trimester of pregnancy.
All these measures should be considered in relationship to the severity of the disease and the urgency of the treatment. NURSING MOTHERS:
Nursing should be discontinued if therapy with all-trans retinoic acid is initiated.
Vesanoid®
Page 5 “RETINOIC ACID SYNDROME”
In many patients (20-25%) with acute promyelocytic leukemia (APL) treated with ‘Vesanoid’ (all-trans retinoic acid), a syndrome may occur characterized by some or all of the following symptoms: fever, dyspnea, acute respiratory distress, pulmonary infiltrates, hypotension, pleural and pericardial effusions, edema, weight gain, hepatic, renal and multi-organ failure (Retinoic Acid Syndrome). RAS is frequently associated with hyperleukocytosis and may be fatal. If symptoms of the “Retinoic Acid Syndrome” become apparent, treatment with a short course of high doses of corticosteroids (i.e. dexamethasone) should be initiated immediately particularly in patients where the syndrome is suspected but hyperleukocytosis is not observed.
During clinical trials hyperleukocytosis has been frequently observed (75%), sometimes associated with the RAS.
For those patients experiencing hyperleukocytosis when they receive all-trans retinoic acid (ATRA) alone, the RAS can be prevented by addition of full-dose anthracycline-based chemotherapy to the all-trans retinoic acid regimen based on the white blood cell (WBC) count. The current therapeutic treatment recommendations are the following:
Immediate treatment of patients presenting with a WBC count of > 5 x 109/L at diagnosis or at any time with a combination of all-trans retinoic acid and chemotherapy.
Addition of full-dose chemotherapy to ATRA therapy in patients with a WBC of < 5 x 109/L at day 0 of the treatment with ATRA and if WBC counts become:
≥ 6 x 109/L at any time from day 1 to day 6 of treatment and/or ≥ 10 x 109/L at any time from day 7 to day 10 of treatment and/or ≥ 15x 109/L at any time from day 11 to day 28 of treatment
Treatment with dexamethasone (10 mg every 12 hours for up to maximum 3 days or until resolution of the symptoms), if the patient presents early clinical signs of the syndrome.
In cases of moderate and severe RAS, temporary interruption of all-trans retinoic acid therapy should be considered.
Mortality and morbidity is reduced by following these treatment recommendations in patients with this syndrome.
There is a risk of thrombosis (both venous and arterial) which may involve any organ system during the first month of treatment (see Adverse Reactions). Therefore, caution should be exercised when treating patients with the combination of all-trans retinoic acid and antifibrinolytic agents such as tranexamic acid, aminocaproic acid or aprotinin (see PRECAUTIONS, Drug Interactions).
Supportive care appropriate for patients with acute promyelocytic leukemia for example prophylaxis for bleeding and prompt therapy for infection, should be maintained during therapy with tretinoin. The patient’s hematologic profile, coagulation profile, liver function test results, and triglyceride and cholesterol levels should be monitored frequently.
All-trans retinoic acid may cause intracranial hypertension/pseudotumor cerebri. The concomitant use of other agents known to cause intracranial hypertension/pseudotumor cerebri such as tetracyclines might increase the risk of this condition (see PRECAUTIONS, Drug Interactions).
The ability to drive or operate machinery might be impaired in patients treated with all-trans retinoic acid, particularly if they are experiencing dizziness or severe headache.
Micro-dosed progesterone preparations (“minipill”) may be an inadequate method of contraception during treatment with all-trans retinoic acid.
Vesanoid®
Page 6 PRECAUTIONS DRUG INTERACTIONS:
As all-trans retinoid acid is metabolized by the hepatic P450 system, there is the potential for alteration of pharmacokinetics parameters in patients administered concomitant medications that are also inducers or inhibitors of this system. Medications that generally induce hepatic P450 enzymes include rifampicin, glucocorticoids, phenobarbital and pentobarbital. Medications that generally inhibit hepatic P450 enzymes include ketoconazole, cimetidine, erythromycin, verapamil, diltiazem and cyclosporine. There are no data to suggest that co-use with these medications increase or decreases either efficacy or toxicity of all-trans retinoic acid. There are no data on a possible pharmacokinetic interaction between all-trans retinoic acid and daunorubicin and cytosine arabinoside.
Antifibrinolytic agents such as tranexamic acid, aminocaproic acid, and aprotinin: cases of fatal thrombotic complications have been reported rarely in patients concomitantly treated with all-trans retinoic acid and antifibrinolytic agents. Therefore, caution should be exercised when administering all-trans retinoic acid concomitantly with these agents (see WARNINGS).
Agents known to cause intracranial hypertension/pseudotumor cerebri such as tetracyclines: All-trans retinoic acid may cause intracranial hypertension/pseudotumor cerebri. Concomitant administration of all-trans retinoic acid and agents known to cause intracranial hypertension/pseudotumor cerebri as well might increase the risk of this condition (see WARNINGS).
Contraindicated drug associations (see Contraindications) Vitamin A: As with other retinoids, all-trans retinoic acid must not be administered in combination with vitamin A because symptoms of hypervitaminosis A could be aggravated. RENAL AND HEPATIC IMPAIRMENT
The pharmacokinetics of all-trans retinoic acid in patients with compromised kidney or liver function have not been studied. As with other retinoids, the need for dosage adjustments in patients with renal or hepatic impairment is unknown, however, a reduction of dose to 25 mg/m2 is recommended as a precautionary measure.
ADVERSE REACTIONS
Symptoms of the "Retinoic Acid Syndrome" in APL have been frequently reported and may be life- threatening unless treated (see WARNINGS).
The safety profile of ‘Vesanoid’ (all-trans retinoic acid) has been evaluated retrospectively in a small number of patients.
In persons treated with the recommended daily doses of ‘Vesanoid’, the following adverse events were observed frequently (in about ¼ of the patients or more) signs and symptoms of the hypervitaminosis A syndrome (including xeroderma, lip and mouth dryness, cheilitis, rash, edema, nausea, vomiting and bone pain). Headache, fever, shivering, fatigue, back pain, chest pain, dyspnea, coughing, abdominal pain, dermal bleeding, and elevation in serum triglycerides, cholesterol and transaminases may also be observed.
Vesanoid®
Page 7
The following adverse events, considered remotely, possibly or probably related to drug treatment have been reported in less than ¼ of all APL patients treated with ‘Vesanoid’ in the clinical trials:
Autonomic Nervous System: tachycardia, hypertension, hypotension, flushing, pallor, red extremeties. Body as a Whole: generalized pain, abdominal distension, post traumatic pain, chest discomfort, hypothermia. Cardiovascular System: cardiac failure, cyanosis, heart enlarged, arrhythmias. Cases of
thrombosis (both venous and arterial) involving various sites (e.g. cerebrovascular accident, myocardial infarctions, renal infarct) have been reported uncommonly.
Central and Peripheral Nervous System: dizziness, confusion, intracranial hypertension, light headed feeling, flank pain, numbness of extremeties, abnormal gait, leg weakness, neurologic reaction, inguinal pain, visual field defects, hyporeflexia, paresthesia. Dermatological: pruritus, increased sweating, alopecia, dry scalp, nasal dryness, nail disorder, photosensitivity reaction, xerophthalmia, erythemia. Gastrointestinal: abdominal pain, diarrhea, constipation, blisters in the mouth, stomach upset, dysphagia, buccal mucosa ulceration, stomatitis, flatulence, ulcer, pancreatitis, diminished appetite. Metabolic and Nutritional Disorders: weight changes, edema of extremities, acidosis, gout, dehydration, fluid overload, moonface, elevation in serum creatinine. Musculoskeletal: musculoskeletal pain. Platelet, Bleeding & Clotting: disseminated intravascular coagulation (DIC), nosebleed and other bleeding disorders, thrombosis. Psychiatric: generalized weakness, anxiety, lethargy, depression, malaise, insomnia, anorexia, agitation, forgetfulness. Resistance Mechanism Disorders: infection, septicemia, moniliasis. Respiratory System: pleural effusion, nasal congestion, pharyngitis, rale, respiratory insufficiency, asthma-like syndrome, pneumonia, respiratory distress, tachypnea, pharynx irritation, pulmonary infiltration, hypoxia, sinusitis, bronchial asthma. Special Senses: blurred vision, visual disturbance, photophobia, conjunctivitis, decreased vision, changes in visual acuity, ear fullness, earache, ear buzzing. Urinary System: dysuria, kidney failure, urinary tract infection, micturition frequency, renal insufficiency, cystitis.
The decision to interrupt or continue therapy should be based on an evaluation of the benefit of the treatment versus the severity of the side effects.
Vesanoid®
Page 8 POST-MARKETING EXPERIENCE: Metabolic and Nutritional Disorders: Occasional cases of hypercalcemia have been reported. Dermatological: Sweet’s syndrome has been reported uncommonly. Erythema nodosum has been reported rarely. Hematologic: Thrombocytosis has been reported rarely. Marked basophilia with or without symptomatic hyperhistaminemia has been reported rarely, mainly in patients with the rare APL variant associated with basophilic differentiation. Musculoskeletal: Myositis has been reported rarely. Others: Vasculitis, predominantly involving the skin has been reported rarely.
There is limited safety information on the use of all-trans retinoic acid in children. There have been some reports of increased toxicity in children treated with tretinoin, particularly increased pseudotumor cerebri.
SYMPTOMS AND TREATMENT OF OVERDOSAGE
In cases of overdose with all-trans retinoic acid reversible signs of hypervitaminosis A (headache, nausea, vomiting, mucocutaneous symptoms) can appear. The recommended dose in acute promyelocytic leukemia is one-quarter of the maximum tolerated dose in solid tumor patients and below the maximum tolerated dose in children. There is no specific treatment in the case of an overdose, however, it is important that the patient be treated in a special hematologcal unit.
DOSAGE AND ADMINISTRATION
A total daily dose of 45 mg/m2 body surface divided in two equal doses is recommended for oral administration to APL patients, including pediatric and geriatric patients.
This is approximately 8 capsules per adult dose. It is recommended that pediatric patients be treated with 45mg/m2 unless severe toxicity becomes apparent. Dose reduction should be particularly considered for children with intractable headache.
Treatment should be continued for 30 to 90 days until complete remission has been achieved.
After completion of remission, a course of consolidation chemotherapy including anthracycline and cytosine arabinoside should be initiated immediately; for example, three courses in 5 to 6 week intervals.
If there has been a remission with ATRA alone, it is not necessary to modify doses of ATRA if ATRA is used with chemotherapy.
The effect of food on the bioavailability of all-trans retinoic acid has not been characterized. Since the bioavailability of retinoids, as a class, is known to increase in the presence of food, it is recommended that all-trans retinoic acid be administered with a meal or shortly thereafter.
Vesanoid®
Page 9 PHARMACEUTICAL INFORMATION DRUG SUBSTANCE: Proper Name: Chemical Name:
3,7-dimethyl-9-(2,6,6-trimethylcyclohex-1-enyl)nona-2,4,6,8-all-trans-
Structural Formula: Molecular Formula: Molecular Weight: Description:
Yellow to light-orange crystalline powder with very low solubility in
water. Slightly soluble in alcohol and in chloroform. It is very sensitive to light and oxygen.
Composition:
Each capsule contains 10 mg tretinoin. The non-medicinal
ingredients are: soybean oil, gelatin, partially hydrogenated soybean oil, glycerol, yellow beeswax, hydrogenated soybean oil, hydrogenated hydrolyzed starch, sorbitol, iron oxide, mannitol, titanium dioxide
STABILITY AND STORAGE RECOMMENDATIONS:
Bottles: Keep the bottle tightly closed; store at 15-30°C. Protect from light.
AVAILABILITY OF DOSAGE FORMS
‘Vesanoid’ (all-trans retinoic acid) capsules are available in bottles of 100 capsules.
INFORMATION FOR THE PATIENT
You have been prescribed 'Vesanoid' (pronounced VES-AN-OYD) by your doctor. Reading this information can help you learn about 'Vesanoid' and how to make this medicine work best for you. If you have any questions or concerns after reading this information, speak with your doctor or pharmacist.
What is Acute Promyelocytic Leukemia? Acute promyclocytic leukemia, also known as APL, is a form of cancer in the blood where there
is uncontrolled growth of certain types of abnormal white blood cells.
Symptoms of the disease include weakness, tiredness and weight loss. Treatment for APL can include chemical therapy (known as chemotherapy), blood transfusions,
Vesanoid®
Page 10
What is 'Vesanoid'? 'Vesanoid' is a prescription medication. It belongs to the family of drugs called retinoids. Each capsule contains 10 mg of the active ingredient tretinoin. It also contains additional
(non-medicinal or inactive) ingredients. These are: soybean oil, gelatin, partially hydrogenated soybean oil, glycerol, yellow beeswax, hydrogenated soybean oil, hydrogenated hydrolyzed starch, sorbitol, iron oxide, mannitol, titanium dioxide.
What is 'Vesanoid' used for? How does it work? 'Vesanoid' is used to treat acute promyelocytic leukemia. 'Vesanoid' works to stop the growth of
abnormal blood cells which occur in APL.
Who should take 'Vesanoid'? 'Vesanoid' can be used in patients with APL who have never been treated, as well as those
patients who have not responded to their current anti-cancer treatment, or where the leukemia has returned despite previous anti-cancer treatment.
It is prescribed under the strict supervision of a doctor who is experienced in the treatment of
What should you tell your doctor before you start taking 'Vesanoid'? Before beginning treatment with 'Vesanoid', make sure your doctor knows if: you have ever had a bad reaction to all-trans retinoic acid (tretinoin) or any of the inactive
you are allergic to other medicines, food and dyes you have any other illnesses/diseases, such as kidney or liver disease you are pregnant, plan on becoming pregnant, or are breast-feeding a child you are taking any vitamin preparations or health food supplements that contain vitamin A.
Vitamin A in high doses has many of the same side-effects as ‘Vesanoid’. Taking both together may increase your chance of getting side-effects.
you are taking any other medicines, particularly:
those used to treat fibrin disorders such as tranexamic acid (Cyklokapron®†), aminocaproic
acid (Amicar®†) and aprotinin (Trasylol®†)
birth control pills as ‘Vesanoid’ may reduce the effectiveness of some low dose products antibiotics, particularly tetracyclines, as these products when taken with ‘Vesanoid’ may
This information will help your doctor and you decide whether you should use 'Vesanoid' and what extra care may need to be taken while you are on the medication.
How should 'Vesanoid' be taken? Your doctor has prescribed 'Vesanoid' after carefully studying your case. Other people may not benefit from taking this medicine, even though their problems may seem similar to yours. Do not give your 'Vesanoid' to anyone else. • The number of capsules you will take is based on your body surface area which your doctor will
calculate for you. Take the dose which the doctor has prescribed twice daily.
• Treatment can last anywhere from 1 to 3 months depending on your response to the treatment. If
you respond completely to 'Vesanoid' therapy, other treatment will follow.
• Take this medicine only as directed by your doctor. Do not take more of it, do not take it more
often, and do not take it for a longer time than your doctor ordered.
• A negative pregnancy test result must be obtained within the two weeks before starting treatment
with ‘Vesanoid’. It is suggested that additional pregnancy tests be done at monthly intervals during therapy.
Vesanoid®
Page 11
What should you do if you forget a dose of the medication? • If you forget to take a dose of 'Vesanoid' take it as soon as possible, then just carry on with the
regular times you take your medication. If you remember your missed dose close to the time for your next dose, do not double your dose.
• It may be a good idea to ask your doctor, pharmacist or nurse ahead of time what to do about
What else should you remember while you are taking 'Vesanoid'? • 'Vesanoid' can cause birth defects. There is an extremely high risk that your baby will be deformed if you are pregnant while taking ‘Vesanoid’. Therefore it should not be taken during pregnancy. If you are a woman of child-bearing potential you must use effective contraception for at least one month before beginning therapy, during therapy and at least one month following discontinuation of therapy.
• Breast-feeding of infants should be discontinued if therapy with 'Vesanoid' is started. • Get your blood monitored regularly and keep all of your scheduled doctor's appointments. • Your ability to drive a motor vehicle or operate machinery might be impaired if you are taking
‘Vesanoid’, especially if you experience dizziness or a severe headache.
What are the possible unwanted effects of 'Vesanoid'? Unwanted effects are possible with all medicines. Tell your doctor or pharmacist as soon as possible if you do not feel well while you are taking 'Vesanoid'. The most common possible unwanted effects are: • dry
• dry mouth and lips • swelling of the mouth and lips • rash • swelling • nausea • vomiting • bone pain. Less common possible unwanted effects are: • headache • shivering • tiredness • back
• depression. Should you develop depression or your depression worsens, consult your doctor. Signs of depression include feelings of sadness, irritability, unusual tiredness, trouble concentrating, change in normal sleep patterns and loss of appetite. What possible unwanted effects require immediate medical attention? Call your doctor immediately if you notice any of the following symptoms: fever, difficulty breathing, shortness of breath, lightheadness, dizziness or a faint feeling, unusual Vesanoid®
Page 12
swelling, weight gain, difficulty in urination, yellowing of the skin or eyes.
Some or all of these symptoms may be signs of retinoic acid syndrome which is a medical emergency and should be treated immediately. If you become pregnant while on this medication and within one month following discontinuation
of therapy you must consult with your doctor immediately as 'Vesanoid' can cause birth defects.
If you are concerned about these or any other unexpected effects while on 'Vesanoid' talk with your doctor or pharmacist.
What should you do in case of an overdose or accidental taking of 'Vesanoid'? Contact your doctor and/or poison control centre immediately if you suspect you have taken an
overdose or someone else accidentally ingests your 'Vesanoid'. If you are unable to contact them, go to a hospital emergency department for medical help.
What is the safe way to handle and dispose of 'Vesanoid'? Capsules of 'Vesanoid' should not be opened. Be sure that any discarded medicine is out of the reach of children. If you need help with safe disposal of 'Vesanoid', consult your pharmacist. How should this product be stored? Keep out of the reach of children. Store at room temperature (15-30°C) in the original labelled container Store away from heat and direct light. This leaflet does not provide all known information about 'Vesanoid'. If you have any further questions or concerns about your treatment, please speak with your doctor or pharmacist.
†Cyklokapron is a registered trademark of Pharmacia Aktiebolag, Amicar is a registered trademark of American
Cyanamid Company, Trasylol is a registered trademark of Bayer Aktiengesellschaft
Vesanoid®
Page 13 PHARMACOLOGY TEST TYPE Therapeutic Activity:
Ehrlich sarcoma, mouse Ehrlich ascites, sarcoma, mouse Crocker sarcoma S180, mouse leukemia L1210, rat Walker carcinosarcoma 256, rat uterus epithelioma T8 (Guerin)
to 1.6% of body weight; antagonism of several tumor-induced immunosuppressive changes
Vesanoid®
Page 14 TEST TYPE
factor, interleukin-alpha, interleukin 4, tumor necrosis factor alpha
Mechanism of Action:
retinoic acid produced high binding affinity ligand
RARmyl and mylRAR fusion transcripts found in acute promyelocytic leukemia; chimeric protein has altered transcriptional activation properties
General Pharmacodynamics:
effect on hexobarbital narcosis, placing/grasping reflex
Vesanoid®
Page 15 TEST TYPE
doses up to 1 mg/kg; at 10 mg/kg, biphasic effects on blood pressure, biphasic effects on respiration, slight bradycardia; similar effects produced by vehicle
administration of P185x2 mastocytoma cells
carbomylmethyl-Ficoll; no effect on immunosuppression caused by cyclophosphamide or cyclosporin A
5, 15 mg/kg) daily for 5 days prior to challenge, then daily for 1 week and 3 times weekly thereafter
no enhancement of proliferative response in mixed lymphocyte culture; no stimulation of lymphocyte response to mitogens
15, 50 mg/kg) daily for 6 days prior to challenge
Vesanoid®
Page 16 TEST TYPE
No effect on mitogenic response to phytohemagglutinin or concanavalin A administered 1-25 days after tretinoin
neurological signs of experimental allergic encephalomyelitis
mitogenic effects of phytohemagglutinin or rabbit -antihuman-thymocyte globulin; no effect on conconavalin A or pokeweed mitogen
activity in response to K562, KG-1, MOLT-4, SK-N-SH, and LA-N-5 cells
2-fold increase in VLDL-triglyceride secretion rate
Increase in VLDL and HDL lipoproteins; no effect on serum cholesterol
nephrocalcinosis and reduced calcium loss from bone due to 7.5 mg/kg cholecalciferol; no effect on hypercalcemia
Vesanoid®
Page 17 TEST TYPE
cells in vagina; irregular mating patterns; no or slight effect on serum progesterone levels in vitamin A deficient animals
surgery, 250 μg (approximately 1.25 mg/kg) on day 1 post-surgery, then 100 μg/day (approximately0.5 mg/kg)
quantitatively subnormal spermatogenesis in vitamin A deficient animals
Activation of protein synthesis in 111 of 698 testicular proteins
Drug Interactions:
nonsteroidal anti-inflammatory drugs (NSAIDS)
aminogluethimide, cimetidine, itraconazole, metyrapone, saperconazole
Vesanoid®
Page 18 TOXICOLOGY ACUTE TOXICITY: OBSERVATION LD50 (mg/kg)
Symptoms noted in the mice and rats included sedation, hair loss, respiratory depression, blood-encrusted eyes, swollen eyelids, changes in skin texture, cachexia, diuresis, diarrhea and salivation.
Vesanoid®
Page 19 LONG-TERM TOXICITY: ROUTE & DURATION Subchronic Toxicity:
Glomerular hyperemia, glomerular edema, tubular cell degeneration
decreased weight gain at all doses; slight decrease in hematocrit; bone fractures at 1.56 mg/kg or higher
doses, 2/10 dead after 11 - 12 days at 215 mg/kg; 8/10 dead after 6 - 14 days at 464 mg/kg; bone changes at both doses
Reduced body weight gain, bone fractures, decrease in red blood cells, hemoglobin hematocrit, albumin; increase in cholesterol, alkaline phosphatase, alpha/beta globulins
albumin, increased serum alkaline phosphatase
At two highest doses, increased liver weight and increased serum alkaline phosphatase
doses, hyperplasia of blood-forming elements, slight increase in liver Kupffer cells, thinning of epidermis
At high dose, increased alkaline phosphatase, decreased albumin; decreased cholesterol
Vesanoid®
Page 20 ROUTE & DURATION
depressed growth, increased serum alkaline phosphatase, bone fractures, testicular degeneration at 14 mg/kg/day; decreased haematocrit/ red blood cells, increased alkaline phosphatase at 4 mg/kg/day; decreased haematocrit in females at 1 mg/kg/day
Dose-related renal changes - tubular dilation, basophilia, mineralization, glomerular adhesions
At 30 mg/kg/day, decreased body weight gain, subacute eczema, acanthotic proliferation of epidermis, spermatogenesis, atrophy of testicular tubular epithelia, hyperplasia of blood-forming elements in marrow; no mortality
Chronic Toxicity: TERATOLOGY AND REPRODUCTION: DOSE ROUTE & DURATION Segment I Study:
No effect on fertility or reproductive capacity;
increased mortality of offspring in 5 mg/kg
Segment II Study:
Dose-related teratogenicity; resorption of all
fetuses at 9 mg/kg or higher; maternal toxicity at doses above 3 mg/kg
Skeletal abnormalities at 3 and 10 mg/kg;
maternal toxicity, fetal resorptions, and no viable offspring at high dose
6 mg/kg/day; slight embryotoxicity, but all offspring died at 6 mg/kg/day; no maternal toxicity
Dose-related incidence of spina bifida aperta
Increased incidence of polydactyly; no clear
Teratogenicity (spina bifida, tail defect, craniofacial defect)
Vesanoid®
Page 21
Embryotoxicity at 50 mg/kg; teratogenicity and
gestation days 9 - 11; 5% teratogenicity at low dose given on gestation days 8 - 10
Dose-related teratogenicity; no effect on
offspring at 2 and 5 mg/kg/day; low birth weight and 50% mortality during lactation period at high dose
a) Peak resorption rate on gestation day 9;
Maxillofacial malformations; higher doses
Significant postnatal mortality after 5 mg/kg on
11 - 13, 14 - 16; 2.5 or 5 mg/kg p.o. on
gestation days 11 - 13; behavioral changes in
or 6 mg/kg p.o. on gestation days 14 - 16
Dose and time-related teratogenicity and
embryolethality; peak effect on gestation day 7
Teratogenicity and significant increase in
resorptions at 6 mg/kg/day; no evidence of skeletal abnormalities nor maternal toxicity
Slight reduction in maternal weight gain,
increased resorptions, reduced fetal weight and survival at 1 and 2 mg/kg/day; teratogenicity at high dose
Doses of 25 and 75 mg/kg/day not tolerated; all
fetuses aborted on day 19 at 15 mg/kg/day; at 5 mg/kg/day, teratogenicity in 1/24 fetuses; 14/24 fetuses did not survive 24-hour
Dose-dependent embryotoxicity; teratogenicity
b) No malformations but 5/19 aborted fetuses
Gestation days 24 - 35 most sensitive for
Vesanoid®
Page 22 Segment III Study:
Slight inhibition of maternal weight gain at high
dose; slight reduction (-12 to 16%) in survival of offspring; no functional or behavioral change in offspring
MUTAGENICITY: ROUTE & DURATION
metabolic activation; 8 mcg/plate with/without UV exposure
CARCINOGENICITY: ROUTE & DURATION
Absence of carcinomas at high dose; no effect on incidence of papillomas induced by 7, 12 dimethyl-benz[a]anthracene + 12-0-tetradecanoyl-phorbol-13-acetate
Increased incidence of diethylnitrosamine-induced liver tumors; tretinoin alone had no effect
Vesanoid®
Page 23 BIBLIOGRAPHY
Adamson PC, et al. Dose dependent pharmacokinetics of all-trans retinoic acid. J Natl Cancer Inst 1992;84:1332-5.
Breitman TR, Keene BR, Hemmit H. Retinoic acid-induced differentiation of fresh human leukaemia cells and the human myelomonocytic leukemia cell lines HL-60, U-937, and THP-1. Cancer Surv 1983;2:263-91.
Castaigne S, et al. All-trans retinoic acid as a diferentiation therapy for acute promyelocytic leukemia: I. Clinical results. Blood 1990;76:1704-9.
Chytil F. Retinoic acid: biochemistry, pharmacology, toxicology and therapeutic use. Pharmacol Rev 1984;26:93S-100S.
Degos L, et al. Treatment of first relapse in acute promyelocytic leukemia with all-trans retinoc acid. Lancet 1990;336:1440-1.
Degos L, et al. All-trans retinoic acid in acute promyelocytic leukemia, from clinical results to molecular biology. Haematologica 1991;76 (Suppl 4):55.
De Luca HF. Retinoic acid metabolism. Fed Proc Fed Am Soc Exp Biol 1979;38:2519-23.
De The H, et al. The t(15;17) translocation of acute promyelocytic leukemia fuses the retinoic acid receptor α gene to a novel transcribed locus. Nature 1990;347:558-61.
De The H, et al. The PML-RARa fusion mRNA generated by the t(15;17) translocation in acute promyelocytic leukemia encodes a functionally altered RAR. Cell 1991;66:675-84.
Fenaux P, Degos L. Treatment of acute promyelocytic leukemia with all-trans retinoic acid. Leukemia Res 1991;15:655-7.
Gerber LE, Erdman JW,Jr. Changes in lipid metabolism during retinoid administration. J Am Acad Dermatol 1982a;6:664-72.
Howard WB, et al. Comparative distribution, pharmacokinetics and placental permeabilities of all-trans retinoic acid, 13-cis retinoic acid, all-trans-4-oxo-retinoic acid, retinyl acetate and 9-cis retinal in hamsters. Arch Toxicol 1989;63:112-20.
Huang ME, et al. Use of all-trans retinoic acid in the treatment of acute promyelocytic leukemia. Blood 1988;72:567-72.
Lefebvre P, et al. Pharmacokinetics of oral all-trans retinoic acid in patients with acute promyelocytic leukemia. Leukemia 1991;5:1054-8.
Lucek RW, Colburn WA. Clinical pharmacokinetics of the retinoids. Clin Pharmacokinet 1985;10:38-62.
Madani KA. Retinoic acid: A general overview. Nutr Res 1986;6:107-23.
Miller VA, et al. Cytochrome P-450 inhibitors as modulators of all-trans retinoic acid metabolism. Clin Res 1993;41:25A.
Muindi J et al. Clinical pharmacology of oral all-trans retinoic acid in patient with acute promyelocytic leukemia. Cancer Res 1992;52:2138-42.
Smith MA, et al. Phase I and pharmacokinetic evaluation of all-trans retinoic acid in pediatric patients with cancer. J Clin Oncol 1992;10:1666-73.
Warrel RP, et al. Differentiation therapy of acute promyelocytic leukemia with tretinoin (all trans retinoic acid). N Engl J Med 1991;324:1385-93.
IMPROVE YOUR ATHLETIC PERFORMANCE WITH NUTRITIONAL SCIENCE There are 10 minutes left in the game on a humid summer afternoon. The score is 1-1, and your team has been pressing for the clinching goal. You know you have the skills, but you just can’t seem to dig deep enough for that extra surge of energy. Although your heart is in the game, your body can’t seem to keep up. There seem
Shared Care Guideline Hydroxychloroquine (Adults) Indication: Rheumatoid arthritis and inflammatory osteoarthritis, discoid and systemic lupus erythematosus, and dermatological conditions caused or aggravated by sunlight. Licensing Information: Treatment of rheumatoid arthritis, discoid and systemic lupus erythematosus, and dermatological conditions caused or aggravated by
 PRODUCT MONOGRAPH
PRODUCT MONOGRAPH  PRODUCT MONOGRAPH
PRODUCT MONOGRAPH 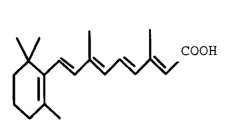 Vesanoid®
Vesanoid®