Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Dexamethasone alters sleep and fatigue in pediatric patients with acute lymphoblastic leukemia
Dexamethasone Alters Sleep and Fatigue in PediatricPatients With Acute Lymphoblastic Leukemia
BACKGROUND. Dexamethasone improves the cure rate of childhood acute lym-
phoblastic leukemia (ALL) but causes physical and behavioral adverse events.
The objective of the current study was to determine the effect of dexamethasone
exposure on sleep and fatigue in pediatric patients with ALL.
METHODS. One hundred pediatric patients with low-risk or standard-risk ALL
were enrolled on 1 of 3 protocols (St. Jude Total XV, Children’s Oncology Group
[COG] 9904, or COG 9905) at 3 institutions. The mean age of the cohort was
9.24 Æ 3.23 years (range, 5.03-18.14 years). The majority of patients were white
(79%) males (62%) with standard-risk ALL (63%). The cohort was divided into 4
subgroups: St. Jude low-risk, St. Jude standard-risk, COG low-risk, and COG
standard-risk. Patients wore a wrist actigraph to monitor sleep activity during 2
consecutive 5-day periods: During the first period, they did not receive dexa-
methasone; and, during the second period, they did. Patients and their parents
1 Division of Nursing Research, St. Jude Chil-
completed fatigue instruments on Days 2 and 5 of each period, and parents com-
dren’s Research Hospital, Memphis, Tennessee.
2 Texas Children’s Cancer Center and Hematology
RESULTS. Actual sleep minutes, sleep duration, total daily nap minutes, and fa-
Service, Texas Children’s Hospital, Houston, Texas.
tigue increased significantly during the dexamethasone treatment for 3 to 4 of
3 Department of Biostatistics, St. Jude Children’s
the subgroups. Total daily nap minutes increased significantly for both standard-
Research Hospital, Memphis, Tennessee.
risk groups during the dexamethasone treatment. Parents reported significant
4 Hematology/Oncology Program, Hospital for
increases in their child’s nighttime awakenings, restless sleep, and nap time dur-
Sick Children, Toronto, Ontario, Canada.
5 Department of Psychology, Tel Aviv University,
CONCLUSIONS. Dexamethasone treatment during continuation therapy for child-
hood ALL significantly and adversely altered sleep and fatigue, confirming that
6 Department of Hematology/Oncology, Our Lady
sleep and fatigue are behavioral responses to dexamethasone. Cancer 2007;
of the Lake Regional Medical Center, Baton
110:2321–30. Ó 2007 American Cancer Society.
7 Department of Pediatrics, Louisiana State Uni-
KEYWORDS: pediatric sleep, fatigue, acute lymphoblastic leukemia, dexametha-
8 Department of Oncology, St. Jude Children’sResearch Hospital, Memphis, Tennessee.
Supported in part by Cancer Center Core GrantCA 21765, RO1NR007610 from the NationalInstitute of Nursing Research and by the Ameri-
D examethasone is central to contemporary treatment of acute
lymphoblastic leukemia (ALL) because of the drug’s marked
antileukemic effects compared with other glucocorticoids, such as
can Lebanese Syrian Associated Charities.
prednisone.1–12 Although it is highly effective in the treatment of
We sincerely appreciate the insights of our study
ALL, dexamethasone also is associated with adverse behavioral
consultants Drs. Ann Berger and Bruce Camitta
events, including mania, psychosis, and altered sleep and fatigue.11–15
and the editorial wisdom of Dr. Angela McArthur.
Because dexamethasone evokes variable patient responses,16 it is pos-sible that behavioral responses are related to interindividual variabili-
Address for reprints: Pamela S. Hinds, PhD, RN,Division of Nursing Research, MS 738, St. Jude
ty in systemic exposure to dexamethasone. Before we can determine
Children’s Research Hospital, 332 N. Lauderdale,
tailored dosing schedules, we must establish the correlation between
Memphis, TN 38105-2794; Fax: (901) 495-2866;
dexamethasone and adverse behavioral effects, particularly sleep and
Received January 16, 2007; revision received
The frequency of adverse events related to sleep and fatigue
July 16, 2007; accepted July 17, 2007.
caused by dexamethasone in pediatric ALL therapy is unknown.
DOI 10.1002/cncr.23039Published online 9 October 2007 in Wiley InterScience (www.interscience.wiley.com).
November 15, 2007 / Volume 110 / Number 10
Earlier studies of the effects of short-term, high-dose
dren’s Cancer Center (TCCC), or the Hospital for Sick
prednisone therapy on behavior, mood, and sleep of
Children. Patients at St. Jude were treated on the
pediatric oncology patients. as reported by their par-
Total XV protocol; patients at TCCC or at the Hospi-
ents, indicated significant negative change in the
tal for Sick Children were treated on Children’s On-
cology Group (COG) 9904 or COG 9905 studies. No
sleep quality, and mood during the on-prednisone
data were collected until after Week 50. The timing
week compared with the off-prednisone week.13,14 In
of the 10-day data collection periods was selected for
2 cases of mania or panic in adolescent girls who
1) similarity in treatment across risk groups within
received dexamethasone as part of their treatment
each ALL clinical trial, 2) less intense treatment
for ALL, the initial symptom was disrupted sleep.15
demands on patients and families, 3) availability of
Sleep in well and chronically ill children and
patients and parents at the treatment settings for
adolescents is a complex, vulnerable process invol-
planned return visits, and 4) ability to maintain the
ving multiple physiologic body systems that are
same sleep environment (the patients’ homes) for
influenced by certain dynamic biologic, social, cul-
the 10-day study period. Only patients in the low- or
tural, and psychologic factors that simultaneously
standard-risk ALL categories participated in this
affect each other.17,18 Sleep in children and adoles-
study, because treatment for high-risk or very-high-
cents evolves in somewhat predictable ways, with
risk ALL differs considerably from the treatment for
decreasing nighttime and daytime sleeping and
Patients needed to be English speaking, willing
Reported outcomes of disrupted or poor-quality
to provide consent according to institutional guide-
sleep are increased daytime sleepiness and inatten-
lines, and had parental consent to participate. There
tive behaviors,23,24 irritability and altered mood,25–27
were no exclusions based on concurrent drugs. Eligi-
reduced ability to learn and use executive function-
ble parents were English speaking, willing to partici-
ing abilities,28–32 lower perceived health-related qual-
pate in this study, and willing to allow their child to
ity of life and well being,33,34 and adversely affected
participate in the study. The study was approved by
immune system indicators.35 Sleep is sensitive to
the institutional review boards at all 3 study sites.
acute and chronic illnesses and related stressors,such as hospitalizations, and to medications, includ-
The objective of Total XV, COG 9904, and COG 9905
including those induced by illness and medications,
protocols is to increase the cure rate in children and
can persist once they are established.37,38 Sleep qual-
adolescents with ALL with the use of risk-directed
ity and fatigue of children and adolescents on and
therapy. The criteria used in risk classification are
off dexamethasone for the treatment of ALL have not
summarized in Table 1. Dexamethasone dosing is
substantially higher in the Total XV protocol than in
The objective of the current study was to deter-
the COG protocols (Table 2). Therefore, for our study,
mine the correlation between systemic exposure to
the St. Jude (Total XV) patients were analyzed sepa-
dexamethasone and sleep quality and fatigue levels
rately from patients who were treated at the other
in pediatric patients during continuation therapy for
childhood ALL. Two hypotheses were tested: 1) Dexa-methasone contributes to changes in sleep efficiency,actual sleep minutes, sleep duration, nocturnal awa-
kenings, total daily sleep minutes, and daily nap
Patients served as their own control. The 10-day
minutes and increased fatigue in children and ado-
study included 2 treatment periods: During the first
lescents; and 2) patient demographic variables (ie,
5 days, patients did not receive dexamethasone (off-
age, sex, and ALL risk category) influence the extent
dex); and during the second consecutive 5 days, they
of change in sleep and fatigue observed during dexa-
did (on-dex). Patients wore an actigraph on their
dominant wrist 24 hours a day for 10 days. Parentsand patients who were age !7 years independentlycompleted fatigue instruments on Days 2 and 5 of
each treatment period, and parents completed a
sleep diary on those same days. This 10-day design
Eligible patients were ages 5 to 18 years and were
exceeded the criterion for number of nighttime
receiving continuation therapy for ALL at St. Jude
Children’s Research Hospital (St. Jude), Texas Chil-
assessments of sleep in children and adolescents.39
Dexamethasone Alters Sleep in ALL/Hinds et al.
Risk Criteria Used in 3 Pediatric Acute Lymphoblastic Leukemia
Dexamethasone Dosages Used in 3 Pediatric Acute Lymphoblastic
No adverse genetic translocationsNo CNS3 status
ALL indicates acute lymphoblastic leukemia; TID, 3 times daily; COG, Children’s Oncology Group;
(no fatigue symptoms) to 70 (high fatigue) andrequires from 6 to 8 minutes to complete.42–44 In this
ALL indicates acute lymphoblastic leukemia; WBC, white blood cells; TEL-AML1, the ets variant 6-
study, the Cronbach a coefficients ranged from .72
acute myeloid leukemia 1 fusion gene; CNS3, central nervous system stage 3 disease.
* Defined by the presence of the breakpoint cluster region-Abelson murine leukemia viral (BCR-ABL)fusion or by !1% leukemic blasts in bone marrow after 6 weeks of remission induction. y High-risk ALL was defined by the presence of CNS3 status, testicular leukemia, or myeloid/lymph-
oid or mixed-lineage leukemia gene (MLL) rearrangement; and very-high-risk ALL was defined by the
The Fatigue Scale-Adolescent, which was designed
presence of BCR-ABL fusion, DNA index <0.81, or >25% leukemic blasts after 4 weeks or >5% leuke-
for adolescents ages 13 to 18 years, is a 14-item, self-
mic blasts after 6 weeks of remission induction.
report instrument that measures adolescents’ cancer-related fatigue on a 5-point Likert-type scale from 14
(no fatigue symptoms) to 70 (high fatigue) and
requires from 3 to 4 minutes to complete.42,43,45 In
The Micromini (Ambulatory Monitoring Inc., Ardsley,
this study, the Cronbach a coefficients ranged from
NY) is a wristwatch-style device that contains a biax-
ial piezoelectric sensor and a microprocessor withprogrammable epoch length. The system’s accompa-
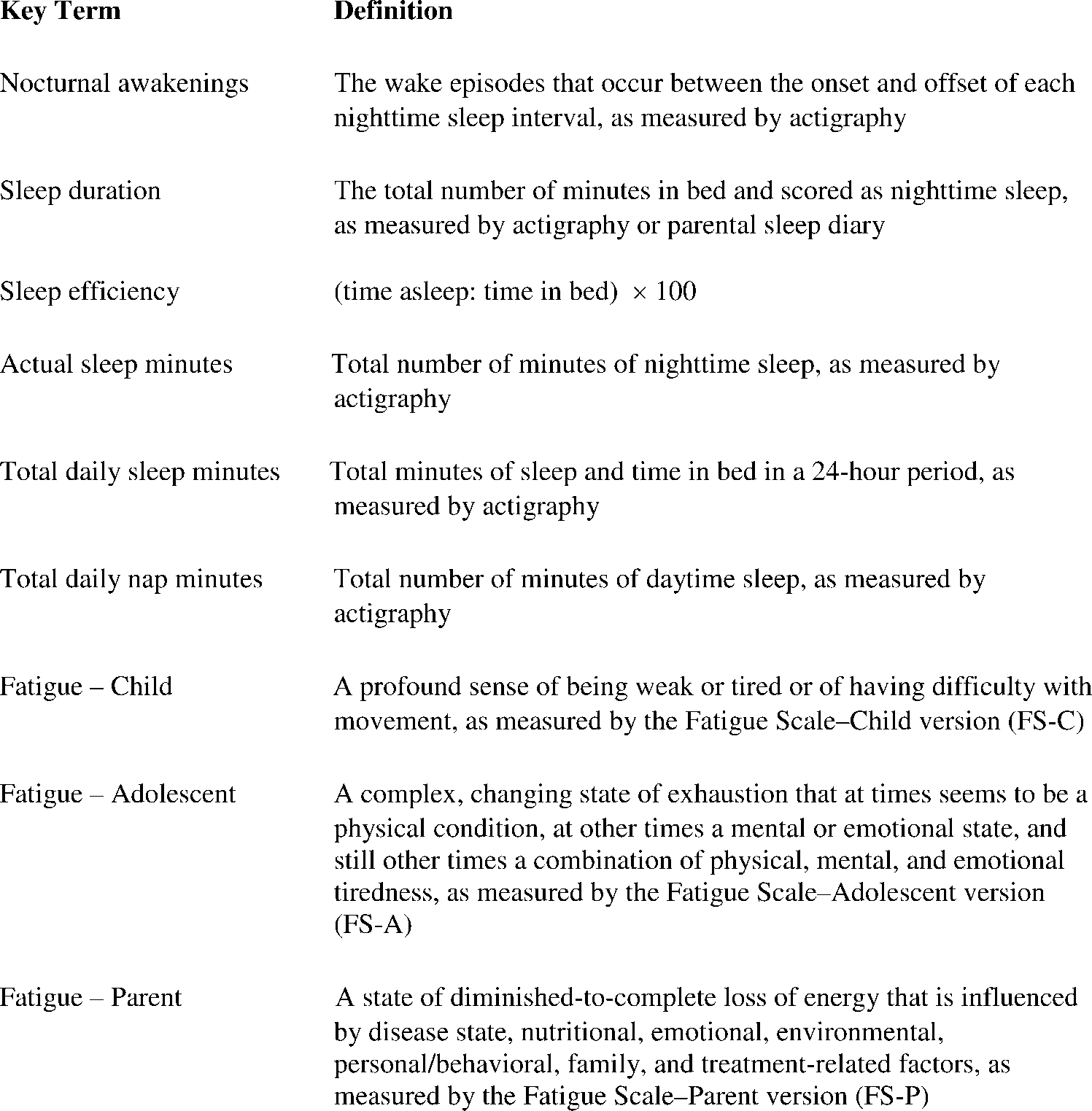
nying software was used to compute the sleep char-
The Fatigue Scale-Parent consists of 17 items that
acteristics (defined in Fig. 1). Sadeh’s algorithm
measure the parents’ perception of their child’s fa-
(previously validated against polysomnography in
tigue on a 5-point Likert-type scale from 17 (no fa-
children40) is the basis of the sleep-wake scoring
tigue) to 85 (high fatigue) and can be completed in 7
to 10 minutes.44 In this study, the Cronbach a coeffi-cients ranged from .91 to .92.
Sleep Diary-ParentThe sleep diary is a 16-item report that was derivedfrom work by Sadeh et al41 that documents the par-
ents’ daily perceptions of their child’s sleep and nap
A study team member completed concurrent medi-
patterns during the previous 24-hour period and is
cation data forms based on information from parents
and a medical record review of medications the childreceived during the 2 5-day study periods. Forty-
eight different medications were administered during
the first 5-day period, and all but 7 were considered
The Fatigue Scale-Child (FS-C), which was designed
ongoing medications for the patient; 53 different
for children ages 7 to 12 years, is a 14-item, self-
medications were administered during the second 5-
report instrument that scores the intensity of the
day period, and all but 18 were considered ongoing.
patient’s fatigue on a 5-point Likert-type scale from 0
Of the medications that were not considered ongoing
November 15, 2007 / Volume 110 / Number 10
FIGURE 1. Definition of study variables.
during the on-dex week, the majority were related to
anticipated that dexamethasone would have detri-
procedures that were considered a single event.
mental effects on sleep and, thus, based our sample
Transfusion status also was monitored, but no partic-
estimates on a 1-sided hypothesis. We projected that
ipant received a transfusion during the study period.
a change of 10 U on dexamethasone would be im-
Hemoglobin values ranged from 9.1 g/dL to 13.8 g/
portant clinically. To detect this difference with 80%
power at an level a of .05 and assuming a 1-sidedtest, approximately 27 evaluable patients were to be
enrolled from each of 4 risk groups: St. Jude low risk,
The sample-size justification was based initially on
St. Jude standard risk, COG low risk, and COG stand-
the only available sleep and steroid coefficients
ard risk. Given the lower enrollment in the COG low-
(sleep efficiency and prednisone) in children and
risk group (n 5 13 patients), findings from the off-
adolescents with ALL; we then re-estimated sample
dex versus the on-dex analyses for this risk group are
size by using the data collected from the first 46
study participants (26 patients at St. Jude and 20patients at TCCC). We used baseline values for sleep
efficiency during the off-dex week to obtain an esti-
We enrolled 100 patients in the study. The majority
mate of variability to be used in the sample-size cal-
were white boys between ages of 7 years and 12
culation and completed 2 separate calculations: 1 for
years who met the criteria for either the St. Jude or
Total XV and 1 for COG 9904 and COG 9905. Similar
COG standard-risk group. The distribution of patients
to the effects of prednisone on sleep efficiency, we
by age, sex, race, and risk group is presented in Table 3.
Dexamethasone Alters Sleep in ALL/Hinds et al.
mixed-effects models, which incorporated all observa-
Demographic Characteristics of 100 Pediatric Patients With Acute
tions, to assess the impact of time period (off-dex or
on-dex) on fatigue. The criterion for significance forall analyses was a P value at the level of a 5 .05. All
analyses were performed with the SAS software pack-
age (Release 9.1; SAS Institute, Inc., Cary, NC).
Dexamethasone Alters Most Sleep Parameters in
According to the actigraphy measurements, dexa-
methasone treatment was associated significantly
with increases in sleep duration, actual sleep min-
utes, total daily sleep minutes, and total daily nap
minutes and with decreased nocturnal awakenings
(Table 4). During the on-dex period, the average
actual sleep minutes, average sleep duration, and av-
erage nap minutes increased significantly in 2 of the
4 risk groups, and average total daily sleep minutes
increased significantly in 3 of the 4 risk groups (Table
5). Parents’ responses in the sleep diary indicated sig-
nificant increases in their child’s nighttime awaken-ings, restless sleep, and nap time in 1 to 4 of the risk
ALL indicates acute lymphoblastic leukemia; COG, Children’s Oncology Group.
groups during the on-dex period and in tirednessand loss of energy during the on-dex period across
Actigraph data are not available for 12 of the study
participants because of actigraph failure or insuffi-cient recordings, a rate that is less than half of the
rate (28%) reported previously in pediatric studies.19
Patient self-reports of fatigueResults of the PROC MIXED analysis indicated signif-
icant increases in FS-C scores between the 2 5-day
To compare the average scores of study variables
periods within each risk group and across all 4 risk
between the 2 5-day study periods, we used a 1-sam-
groups (P < .0001). Significant increases in fatigue
ple Student t test. Only those patients who had at
also were evident in the COG standard-risk group
least 3 of 5 days of actigraph data during each period
(P 5 .014) and in the total patient group of patients
were included in this analysis. Subsequently, longitu-
ages 13 years to 18 years (P 5 .007) (Table 4). Signifi-
dinal methods (PROC MIXED) that incorporated all
cant increases in fatigue between the measurement
observations were used to analyze the data, and the
days (Days 2 and 5) of each 5-day period also were
conclusions obtained from the 2 approaches were
compared. Testing of the regression coefficient corre-sponding to risk group provided the evidence of dif-
ference in sleep and fatigue between the 2 study
Parents reported significant increases in their child’s
periods. We completed a similar analysis for all de-
fatigue during the on-dex period for every risk group
pendent measures based on actigraph measures and
at both data comparison points (Table 4). The PROC
parent sleep diaries. After primary analyses were
MIXED analyses yielded results similar to those
completed, we calculated observed power for each
For fatigue data, we calculated a summed score
Demographic Variables Influence Dexamethasone-
for each fatigue questionnaire at each time point. We
computed the average fatigue score for each study pe-
riod and tested whether the differences between those
Risk group was associated significantly with change
2 scores were significantly different from zero by
in sleep efficiency (P 5 .012), actual sleep minutes
using the 1-sample Student t test. We also used the
(P 5 .013), and nocturnal awakenings (P 5 .034).
November 15, 2007 / Volume 110 / Number 10
TABLE 4PROC MIXED Analyses Comparing Sleep (as Measured by Wrist Actigraphy and Parental Sleep Diary)and Fatigue Scales During Periods Off and On Dexamethasone
COG indicates Children’s Oncology Group; FS-C, Fatigue Scale-Child; FS-A, Fatigue Scale-Adolescent; FS-P, Fatigue Scale-Parent. * The estimates were adjusted by group (risk category). y Significant difference.
Patients in the St. Jude standard-risk group had sig-
actual sleep minutes experienced by the COG low-
nificantly lower sleep efficiency than patients in the
risk group, both St. Jude risk groups slept less: the
COG low-risk group (regression coefficient, 210.77;
COG versus St. Jude low-risk group (regression coeffi-
P 5 .0035) and the COG standard-risk group (regres-
cient, 286.47; P 5 .011) and the COG versus St. Jude
sion coefficient, 27.06; P 5 .011). Compared with the
standard-risk group (regression coefficient, 2111.75;
TABLE 5Mean Values of Sleep Variables From Patients Who Had ‡3 of 5 Days of Actigraphy Data Available
SD indicates standard deviation; Dex, dexamethasone; COG, Children’s Oncology Group. * Significant difference.
Dexamethasone Alters Sleep in ALL/Hinds et al.
TABLE 6Differences in Fatigue Scores Between the Periods Off Dexamethasone and On Dexamethasone for Patients by Risk Group
Difference of average fatigue between Wk 2 and Wk 1 on D 2St. Jude low risk
Difference of average fatigue between Wk 2 and Wk 1 on D 5St. Jude low risk
Difference of average fatigue between Wk 2 and Wk 1St. Jude low risk
SD, standard deviation; COG, Children’s Oncology Group.
P 5 .002). Finally, the St. Jude low-risk group had
(regression coefficient, 6.70; P < .0001), and the fa-
more nocturnal awakenings per night than the COG
tigue findings were similar for adolescents (regres-
low-risk group (regression coefficient, 5.23; P 5 .011)
sion coefficient, 6.45; P 5 .0074). The extent of change
and the COG standard-risk group (regression coeffi-
in child fatigue was not associated with age (P 5 .55),
sex (P 5 .76), or ALL risk group (P 5 .66); likewise,change in adolescent fatigue was not associated with
age (P 5 .45), sex (P 5 .75), or ALL risk group (P 5 .70).
Age was associated with change in sleep duration
Parents reported significant increases in their child’s
(coefficient, 25.95; P 5 .018). Older patients were in
fatigue during the on-dex period (regression coeffi-
bed less during the on-dex period. Older age also
cient, 10.11; P < .0001), but their reports were not
was associated with less total daily sleep minutes
associated with patient age (P 5 .86), sex (P 5 .65), or
SexBoys experienced significantly more nocturnal awa-
kenings per night (coefficient, 3.19; P 5 .020) than
Actigraphic findings from this study indicate that
girls. However, girls napped more (coefficient, 17.07;
dexamethasone treatment significantly alters sleep
P 5 .027). More nocturnal awakenings were asso-
duration, actual sleep minutes, total daily sleep min-
utes, nocturnal awakenings, and total daily nap min-
utes in pediatric patients with ALL. Patient andparent fatigue reports both indicate that dexametha-
sone is associated with significantly increased fa-
On Day 2 of the off-dex period, parental sleep diary
tigue. These findings confirm that altered sleep and
data significantly exceeded actigraph data for 3
fatigue are behavioral responses to dexamethasone.
groups (St. Jude: low-risk group, t 5 22.51; P 5 .02;
The average sleep efficiency in the 4 risk groups
standard-risk group, t 5 22.33; P 5 .027; COG: low-
for both 5-day study periods was lower than that of
risk group, t 5 23.74; P 5 .003). These differences
pediatric inpatients on a psychiatric unit (91.9%) and
were limited to the first night of sleep diary monitor-
of healthy adolescents who were monitored for 1
ing and may reflect the parents’ inexperience with
week (87% and 89%)46,47 and was lower than the
sleep efficiency (90%) that is considered acceptablefor children and adolescents. Only 1 of the 4 risk
groups had an average sleep efficiency that met the
Children experienced significantly more fatigue dur-
acceptable level during the off-dex period, and none
ing the on-dex period than during the off-dex period
of the risk groups achieved that standard during the
November 15, 2007 / Volume 110 / Number 10
on-dex period. This indicates that these patients had
more total daily nap minutes, suggesting that sleep
poor sleep quality even before they began the dexa-
may be sex-sensitive. In studies of healthy grade
methasone period. The poor sleep quality may be
school children and high school youths, girls slept
secondary to the treatment for ALL in terms of the
significantly longer than boys.53,54 Age was not a
chemotherapeutic agents or the systemic effects of
consistent factor of influence on sleep or fatigue in
the treatment.48 but it is not secondary to hospitali-
our study. Only 2 sleep variables, sleep duration and
zation, because none of the patients had been hospi-
total daily sleep minutes, were associated with age;
talized during the study period or during the
the adolescents had less of both compared with the
previous several months. The actigraphy finding of
low sleep efficiency is supported by parent reports of
Although the combined objective and patient
increased restless sleep of their ill child during the
and parent reports indicate that dexamethasone
on-dex period. These combined objective and sub-
adversely affects multiple patient sleep-quality indi-
jective reports indicate that dexamethasone interferes
cators and fatigue, the findings do not explicate the
with sleep quality. The average actual sleep minutes
precise mechanism of influence. The significant
in our cohort during both study periods was less
increase in fatigue may have contributed to the
than that reported for pediatric patients ages 7 to 14
extended sleep duration and increased total daily
years who were hospitalized on a psychiatric unit.47
nap minutes. Together, these influences are known to
The average sleep duration for patients during both
interfere with sleep/wake cycles and sleep regula-
study periods exceeded that of pediatric outpatients
tion.48 Alternatively for the patients in the St. Jude
with well-controlled asthma (8.2 hours) and that of
standard-risk group, which experienced significantly
age-matched, healthy children (8.3 hours).49 The av-
more nocturnal awakenings than the other risk
erage sleep duration in our cohort on certain nights
groups, the resulting sleep fragmentation may have
approached or exceeded the recommended sleep
contributed to these patient’s increased time in bed
time of 10 to 11 hours for children and 9.2 hours for
as an attempt to recover sleep. Indirectly, the sleep
adolescents.19,20 In addition, our pediatric cohort
woke up, on average, 12 to 16 times each night (simi-
patients’ increased fatigue. Finally, individual differ-
lar to the number of awakenings of 9 children with
ences in metabolism of dexamethasone may help to
ALL who received vincristine during maintenance
explain sleep and fatigue responses to dexametha-
therapy but who slept in their home environment50
sone. These possible explanations need to be exam-
and similar to the awakenings of 29 pediatric oncol-
ogy patients who were hospitalized for scheduled
The current study had several limitations. The
chemotherapy for a solid tumor or acute myeloid
small number of patients in the COG low-risk group
means that findings specific to that risk group need
awaken 1 to 5 or 7 times each night.18,19,52 These
to be considered ‘‘exploratory.’’ In addition, our
findings indicate that pediatric patients receiving
results primarily represent white boys ages 7 to 12
dexamethasone for ALL have fewer actual sleep min-
years with standard-risk ALL. We did not study day-
utes, stay in bed longer, but have poorer sleep quality
time sleepiness, a variable that has been confused
than well children, children with chronic illnesses, or
conceptually with or linked to fatigue,22,23 nor did
hospitalized pediatric patients for illnesses other than
we study the functional outcomes of increased
fatigue or altered sleep, such as cognitive or behav-
ALL risk group was associated significantly with
ioral changes.24,32,54 However, our study strengths
only 3 sleep variables (sleep efficiency, actual sleep
include data collection at 3 pediatric cancer centers,
minutes, and nocturnal awakenings), as measured by
which adds to the generalizability of study findings,
actigraphy. Of the 4 risk groups, the St. Jude stand-
ard-risk group received the highest dose of dexa-
responses for fatigue and sleep outcome indicators,
methasone, had significantly lower sleep efficiency
the combination of patient, parent, and objective
than children in the COG risk groups, and had the
reports to study these variables, the ability to com-
lowest actual sleep minutes and sleep duration of all
pare outcomes from consecutive periods when the
4 groups. Dexamethasone treatment, rather than the
patients did or did not receive dexamethasone, and
ALL risk group, was the more consistent source of
the strength of the statistical findings. The clinical
significant influence on sleep outcomes in our study.
implications of this study include the need to pre-
Sex did not appear to influence fatigue, but it
pare patients and families before the initiation of
did influence 2 sleep variables. Boys experienced
continuation therapy for ALL for a likely increase in
more nocturnal awakenings per night, and girls had
sleep duration, actual sleep minutes, and total daily
Dexamethasone Alters Sleep in ALL/Hinds et al.
sleep minutes and fatigue during dexamethasone
11. Kaspers GJ, Pieters R, Veerman AP. Glucocorticoid sensitivity
and resistance in childhood leukemia. In: Pieters R, Kaspers
In conclusion, dexamethasone treatment alters
GJL, Veerman AJP, editors. Drug Resistance in Leukemia andLymphoma II. Amsterdam, the Netherlands: Harwood Aca-
sleep and fatigue in children and adolescents with
ALL, and the degree of alteration differs by patient
12. Bostrom BC, Sensel MR, Sather HN, et al. Dexamethasone
age, sex, and ALL risk category. Our future studies
versus prednisone and daily oral versus weekly intravenous
will examine the relation between these behavioral
mercaptopurine for patients with standard-risk acute lym-
indicators and the biologic indicators of individual
phoblastic leukemia: a report from the Children’s CancerGroup. Blood. 2003;101:3809–3817.
responsiveness to dexamethasone. These behavioral
13. Drigan R, Spirito A, Gelber RD. Behavioral effects of corti-
and biologic indicators have the potential to identify
costeroids in children with acute lymphoblastic leukemia.
pediatric patients with ALL who will be the most sen-
sitive to dexamethasone treatment, thereby allowing
14. Harris JC, Carel CA, Rosenberg LA, Joshi P, Leventhal BG.
clinicians to design optimal dosing schedules for
Intermittent high dose corticosteroid treatment in child-
hood cancer. J Am Acad Child Psychiatry. 1986;25:120–124.
15. Watanabe TK, Sylvester CE, Manaligod JM. Mania or panic
associated with dexamethasone chemotherapy in adoles-
cents. J Adolesc Health. 1994;15:345–347.
16. Zoorob RJ, Cender D. A different look at corticosteroids.
Agthe AG, Doffel W, Neuendank A, et al. Tailored therapy
Am Fam Physician. 1998;58:443–450.
for relapsed or refractory childhood acute lymphoblastic
17. Jenni OG, O’Connor BB. Children’s sleep: an interplay
leukemia. In: Pieters R, Kaspers GJL, Veerman AJP, editors. Drug Resistance in Leukemia and Lymphoma II. Amster-
between culture and biology. Pediatrics. 2005;115:204–216.
dam, the Netherlands: Harwood Academic Publishers;
18. Mindell JA, Owens JA, Carksadon MA. Developmental fea-
tures of sleep. Child Adolesc Psychiatr Clin N Am. 1999;8:
Veerman AJP, Hahlen K, Kamps WA. High cure rate with a
moderately intensive treatment regimen in non-high-risk
19. Glaze DG. Childhood insomnia: why Chris can’t sleep.
childhood acute lymphoblastic leukemia: results of Proto-
Pediatr Clin North Am. 2004;51:33–50.
col ALL VI from the Dutch Childhood Leukemia Study
20. Grigg-Damberger M. Neurologic disorders masquerading
Group. J Clin Oncol. 1996;14:911–918.
as pediatric sleep problems. Pediatr Clin North Am. 2004;
Balis FM, Lester CM, Chrousos GP, Heideman RL, Poplack
DG. Differences in cerebrospinal fluid penetration of corti-
21. Hoban TF. Sleep and its disorders in children. Semin Neu-
costeroids: possible relationship to the prevention of me-
ningeal leukemia. J Clin Oncol. 1987;5:202–207.
22. Hoban TF, Chervin RD. Assessment of sleepiness in chil-
Tanghe A, Delforge A, Bernier M, et al.
dren. Semin Pediatr Neurol. 2004;8:216–228.
chronic lymphocytic leukemia (CLL) cells in presence of
23. Fallone G, Owens JA, Deane J. Sleepiness in children and
glucocorticoids and modulation of their effect by interleu-
adolescents: clinical implications. Sleep Med Rev. 2002;6:
kin-4. In: Pieters R, Kaspers GJL, Veerman AJP, editors.
Drug Resistance in Leukemia and Lymphoma II. Amster-
24. Fallone G, Acebo C, Arnedt J, Seifer R, Carskadon M.
dam, the Netherlands: Harwood Academic Publishers;
Effects of acute sleep restriction on behavior, sustained
attention, and response inhibition in children. Percept Mot
Silverman LB, Gelber RD, Dalton VK, et al. Improved out-
come for children with acute lymphoblastic leukemia:
25. Hansen DE, Vanderberg B. Neurophysiological features and
results of Dana-Farber Consortium Protocol 91-01. Blood.
differential diagnosis of sleep apnea syndrome in children.
J Clin Child Psychol. 1997;26:304–310.
Gaynon PS, Trigg ME, Heerema NA, et al. Children’s Cancer
26. Lewin DS, England SJ, Rosen RC. Neuropsychological
Group trials in childhood acute lymphocytic leukemia:
sequelae of obstructive sleep apnea in children. Sleep Res.
1983-1995. Leukemia. 2000;14:2223–2233.
Jones B, Freeman AI, Shuster JJ, et al. Lower incidence of
27. Yang CK, Kim JK, Patel SR, et al. Age–related changes in
meningeal leukemia when prednisone is replaced by dexa-
sleep/wake patterns among Korean teenagers. Pediatrics.
methasone in the treatment of acute lymphocytic leuke-
mia. Med Pediatr Oncol. 1991;19:269–275.
28. Hansen M, Janssen I, Schiff A, et al. The impact of school
Mitchell CD, Richards SM, Kinsey SE, et al. Benefit of dexa-
daily schedule on adolescent sleep. Pediatrics. 2005;115:
methasone compared with prednisolone for childhood
acute lymphoblastic leukaemia: results of the UK Medical
29. Owens J, Oppipari L, Nobile C, Spirito A. Sleep and day-
Research Council ALL 97 randomized trial. Br J Haematol.
time behaviors in children with obstructive sleep apnea
and behavioral sleep disorder. Pediatrics. 1998;102:1178–
Pui C-H, Evans WE. Treatment of acute lymphoblastic leu-
kemia. N Engl J Med. 2006;354:166–178.
30. Randazzo AC, Muehlbach MJ, Schweitzer PK, et al. Cogni-
10. Bleyer WA, Poplack DG, Balis FM. Pharmacokinetics of
tive function following acute sleep restriction in children
commonly used leukemic agents in children. In: Kobaya-
ages 10–14. Sleep. 1998;21:861–868.
shi N, Akera T, Mizutani S, editors. Childhood Leukemia:
31. Sadeh A, Gruber R, Raviv A. Sleep, neurobehavioral func-
Present Problems and Future Prospects. New York, NY:
tioning, and behavior problems in school-age children.
November 15, 2007 / Volume 110 / Number 10
32. Sadeh A, Gruber R, Raviv A. The effects of sleep restriction
44. Hockenberry MJ, Hinds PS, Barrera P, et al. Three instru-
and extension on school-age children: what a difference an
ments to assess fatigue in children with cancer: the child,
hour makes. Child Dev. 2003;74:444–455.
parent and staff perspectives. J Pain Symptom Manage.
33. Hart CN, Palermo TM, Rosen CL. Health-related quality of
life among children presenting to a pediatric sleep disor-
45. Hinds PS, Hockenberry M J, Tong X, et al. Validity and
ders clinic. Behav Sleep Med. 2005;3:4–17.
reliability of a new instrument to measure cancer-related
34. Pilcher JJ, Ott ES. The relationship between sleep and
fatigue in adolescents. J Pain Symptom Manage. 2007;July
measures of health and well-being in college students: a
repeated measures approach. Behav Med. 1998;23:170–178.
46. Sadeh A, Hauri PJ, Kripke DF, Lavie P. The role of actigra-
35. Mindell JA, Owens JA. A Clinical Guide to Pediatric Sleep:
phy in the evaluation of sleep disorders. Sleep. 1995;18:
Diagnosis and Management of Sleep Problems. Philadel-
phia, Pa: Lippincott, Williams & Wilkins Publishers; 2003.
47. Sadeh A, McGuire JPD, Sachs H, et al. Sleep and psy-
36. Sadeh A. Stress, trauma and sleep in children. Child Ado-
chological characteristics of children on a psychiatric
lesc Psychiatr Clin N Am. 1996;5:685–700.
inpatient unit. J Am Acad Child Adolesc Psychiatry. 1995;34:
37. Puig-Antich J, Goetz R, Hanlon C, et al. Sleep architecture
and REM sleep measures in prepubertal children with
48. Vena C, Parker K, Cunningham M, et al. Sleep-wake distur-
major depression. A controlled study. Arch Gen Psychiatry.
bances in people with cancer. Part I: an overview of sleep,
sleep regulation, and effects of disease and treatment.
38. Puig-Antich J, Goetz R, Hanlon C, Tabrizi MA, Davies M,
Oncol Nurs Forum. 2004;31:735–746.
Weitzman ED. Sleep architecture and REM sleep measures
49. Sadeh A, Horowitz I, Wolach-Benodis L, Wolach B. Sleep
in prepubertal major depressives. Studies during recovery
and pulmonary function in children with well-controlled,
from the depressive episode in a drug-free state. Arch Gen
stable asthma. Sleep. 1998;21:379–384.
50. Gedaly-Duff V, Lee KA, Nail LM, et al. Pain, sleep dis-
39. Acebo C, Sadeh A, Seifer R, et al. Estimating sleep patterns
turbance, and fatigue in children with leukemia and their
with activity monitoring in children and adolescents: how
parents: a pilot study. Oncol Nurs Forum. 2006;33:641–
many nights are necessary for reliable measures? Sleep.
51. Hinds PS, Hockenberry M, Rai SN, et al. Nocturnal awa-
40. Sadeh A, Sharkey KM, Carskadon MA. Activity-based sleep-
kenings, sleep environment interruptions, and fatigue in
wake identification: an empirical test of methodological
hospitalized children with cancer. Oncol Nurs Forum. 2007;
41. Sadeh A, Acebo C, Seifer R, et al. Activity-based assessment
52. Riter S, Wills L. Sleep wars: research and opinion. Pediatr
of sleep-wake patterns during the 1st year of life. Infant
53. Carskadon MA, Wolfson AR, Acebo C, Tzischinsky O, Seifer
42. Hinds PS, Hockenberry-Eaton MA. Developing a research
R. Adolescent sleep patterns, circadian timing, and sleepi-
program on fatigue in children and adolescents with can-
ness at a transition to early school days. Sleep. 1998;21:
cer. J Pediatr Oncol Nurs. 2001;18(2 suppl 1):3–12.
43. Hockenberry-Eaton M, Hinds P. Fatigue in children and
54. Sadeh A, Raviv A, Gruber R. Sleep patterns and sleep dis-
adolescents with cancer: evolution of a program study.
ruptions in school-age children. Dev Psychol. 2000;36:291–
Semin Oncol Nurs. 2000;16:261–272.
PROGRAMMA CARNEVALMARLIA 2010 - DOMENICA 24 gennaio - Inizio ore 14:30 - 1° Corso Mascherato, con sfilata dei carri allegorici, delle mascherate con la partecipazione della Banda Spettacolo “La Campagnola ” di Marlia., Presenta Adele - Animazione musicale con “Adele Group” - Musica Caraibica con DJ EL PERRO e Guppo di Ballo “ RUMBA QUE SALSA” - Divertimento p
Kevin Case Study 1. Age, Exceptionality Kevin is an 18 year old young man who attends Johnson High School. Kevin’s primary exceptionality is intellectual disabilities, with a secondary exceptionality of an orthopedic impairment. 2. Present Levels of Academic Achievement and Functional Performance / Age- appropriate Transition Assessment Kevin Based on Flori
 November 15, 2007 / Volume 110 / Number 10
FIGURE 1. Definition of study variables.
November 15, 2007 / Volume 110 / Number 10
FIGURE 1. Definition of study variables.