Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
3601_e20_p438-453
3601_e20_p438-453 2/19/02 8:59 AM Page 438
Seizures and Syncope in the Cancer Patient
Neurologic complications in cancer patients com-
may be present in a patient, so an accurate evalua-
monly involve altered levels of consciousness. This
tion will require a comprehensive work-up of each
chapter discusses seizures and syncope, two prob-
lems in cancer patients that can have multiple causes. Whereas normally it is easy to distinguish between
Primary and Metastatic Brain Tumors
these two conditions, occasionally when there are noobservers of the event, it can be difficult for the clin-
Primary and metastatic brain tumors can present with
ician to be certain whether a seizure or syncope has
focal or generalized seizures. Among infiltrating
occurred. It is hoped that the sections that follow will
gliomas, low-grade gliomas, particularly those involv-
help clarify the etiologies, presentations, and treat-
ing the temporal lobe, are the most likely to cause
ments for seizures and syncope in cancer patients, in-
seizures, usually with onset in childhood or in the teen-
cluding those caused by drugs given for cancer
age years (Bartolomei et al., 1997; Britton et al., 1994;
Rogers et al., 1993). Patients with seizures caused bybrain tumors present with generalized tonic-clonicseizures or simple or complex partial seizures, with or
SEIZURES
without secondary generalization. Unfortunately, attimes the seizures are difficult to treat. Additionally, an
Seizures are the first clinical manifestation in ap-
increased frequency of seizures in a patient with a
proximately 30% of patients with primary or meta-
known low-grade brain tumor may indicate tumor
static brain tumors (Cascino, 1993; Stein and Cham-
transformation to a more malignant histology.
berlain, 1991). In patients who have systemic cancer
In general, patients with primary brain tumors who
without brain metastases, the incidence of ictal phe-
present with seizures but do not have magnetic res-
nomena is not well documented. In fact, there
onance imaging (MRI) or computerized tomography
have been no prospective or retrospective studies of
(CT) confirmation of tumor at their initial evaluation
seizures in this group, and some seizures in these pa-
have a better prognosis. This fact may reflect an ear-
tients are not recognized as such (e.g., complex par-
lier diagnosis of tumor and/or lower grade of malig-
tial seizures). On occasion, non-ictal, abnormal
nancy. Improvement in MRI scanning techniques al-
movements may be confused with seizures.
lows these patients to be diagnosed with tumor at anearlier time.
Surgery, when feasible, is a desired therapeutic ap-
Etiology
proach for both tumor removal and seizure control
The etiology of seizures in cancer patients is pre-
(Britton et al., 1994). Modern techniques, such
sented in Table 20–1. More than one etiologic factor
as brain mapping and intraoperative electroen-
3601_e20_p438-453 2/19/02 8:59 AM Page 439
Seizures and Syncope in the Cancer PatientTable 20–1. Etiology of Seizures in Cancer Patients
Primary tumors (gliomas), metastatic tumors
Primary tumors (meningiomas), metastatic tumors
Primary tumors (meningeal gliomatosis), metastatic tumors (meningeal carcinomatosis,
Platinum, methotrexate, cytarabine, busulfan, L-asparaginase, 5-fluorouracil, ifosfamide, paclitaxel
IL-2, interferon, lymphokine-activated killer cells, granulocyte-macrophage colony-stimulating factor
Radiologic contrast media used for CT scanning
Volume depletion, overhydration, syndrome of inappropriate antidiuretic hormone secretion
Malnutrition, pancreatic tumors, total parenteral nutrition withdrawal
Nutritional, secondary to chemotherapy (cisplatin)
Drug-related (chemotherapy—cisplatin, amphotericin B), hypoparathyroidism
Pulmonary fibrosis (chemotherapy related), pulmonary embolism, lung cancer
Stroke (thrombotic, embolic), vasculitis (paraneoplastic, treatment induced)
Post-traumatic, due to thrombocytopenia, after spinal taps
Spontaneous, due to thrombocytopenia or coagulopathy
Herpes simplex, herpes zoster, cytomegalovirus
Common pathogens, Listeria, Mycobacterium
cephalography, allow accurate identification of the
Systemic cancers most likely to metastasize to the
seizure focus (Lim et al., 1991; Cascino, 1990; Smith
brain are melanoma, lung carcinoma, renal cell car-
et al., 1991). When surgical resection is not feasible,
cinoma, breast carcinoma, cancers of the gastroin-
radiation therapy (RT) can help control the seizures
testinal tract, and choriocarcinoma (Trillet and
Biron, 1989; Flowers and Levin, 1993; Rosner et al.,
3601_e20_p438-453 2/19/02 8:59 AM Page 440
SYMPTOMS SECONDARY TO CANCER AND ITS TREATMENT
1986). As time of survival increases with the use of
chemotherapy, other types of cancer are thus given
Seizures occur in fewer than 1% of patients treated
more time to develop and can also metastasize to the
with systemic chemotherapy and can occur as a man-
brain. Seizures can also occur secondary to
ifestation of the neurotoxicity of chemotherapeutic
parenchymal brain metastases and with dural and lep-
agents. In general, chemotherapy-associated neuro-
tomeningeal metastases (Wasserstrom et al., 1982;
toxicity is related to specific drugs or drug combina-
tions, dose intensity, and route of administration(Weiss et al., 1974). Because the early studies pre-
Seizures Related to Paraneoplastic
dated both the CT and MRI era, it is possible that
small cerebral tumor metastases were present in thepatient population reported. The chemotherapeutic
Although rare, paraneoplastic encephalomyeloneuri-
agents most commonly reported to cause central ner-
tis can manifest with complex partial or generalized
vous system (CNS) toxicity are cisplatin, methotrex-
seizures, and these occur most frequently with anti-
ate, L-asparaginase, and busulfan. Neurotoxicity is
Hu–associated paraneoplastic encephalomyeloneuri-
also caused by high doses of busulfan, which is ad-
tis in patients with small cell lung carcinoma. Occa-
ministered to recipients of bone marrow transplants
sionally seizures occur in patients with paraneoplastic
(Antonini et al., 1998; Kramer et al., 1997; Snider et
encephalomyeloneuritis associated with prostate or
renal cell carcinoma (Dalmau et al., 1992; Drislane,
The frequency of neurologic toxic effects increases
1994; Franck et al., 1987; de Toffol et al., 1997).
with intra-arterial or intrathecal administration, and
Paraneoplastic temporal lobe epilepsy has even been
blood–brain barrier modification and also when che-
reported in a patient with testicular cancer (Ahern et
motherapy (especially methotrexate) is administered
in conjunction with RT (Weiss et al., 1974; Feun etal., 1991; Stewart et al., 1992; Newelt and Dahlborg,
Seizures Related to Radiation Therapy
1987). Seizures have also been induced by fat em-boli during the intra-arterial administration of cis-
The frequency of preexisting seizures may increase
acutely during RT because of increased cerebraledema. With the use of corticosteroids to controledema and careful monitoring of antiepileptic drug
Methotrexate. Moderate and high doses of intra-
levels, this is a rather infrequent occurrence. Seizures
venous methotrexate can cause leukoencephalopathy
may also occur as a result of radiation-induced brain
with seizures and other neurologic symptoms (Gen-
necrosis or vasculopathy, which are delayed effects
vresse et al., 1999). Methotrexate increases the con-
of RT (Ciaudo-Lacroix and Lapresle, 1985; Rider,
centration of homocysteine, which is oxidatively
1963; Spencer, 1998). Positron emission tomography
metabolized to the excitatory amino acid neurotrans-
and single-photon emission computed tomography
mitters homocisteic acid and cysteine sulfinic acid.
scans of the brain can help to distinguish brain tu-
Homocysteine also damages the vascular endothelium
mors from radiation-induced necrosis, although ac-
(Quinn et al., 1997). Seizures have been reported
tive epileptogenic foci caused by radiation necrosis
with intrathecal and intraventricular administration of
can demonstrate hyperperfusion and hypermetabo-
methotrexate and cytosine arabinoside as well (Lee
et al., 1997; Resar et al., 1993). Neuroimaging stud-
Seizures have been reported as immediate side
ies, particularly MRI scans of the brain, show diffuse
effects (occurring within the first 2 weeks) in pa-
white matter lesions, some of which may enhance, or
tients treated with radiosurgery. This may be due to
may demonstrate a more focal pattern (Lovblad et al.,
a direct effect of irradiation on cellular permeabil-
1998). Aminophylline has been reported to be an ef-
ity and leakage of irritative chemical products; no
fective treatment for methotrexate-induced subacute
connection has been made with prior external beam
neurotoxicity (Bernini et al., 1995).
radiation, use of corticosteroids, target volume, iso-dose, or pretreatment edema (Werner-Wasik et al.,
Cisplatin. Seizures following intravenous cisplatin
are mainly due to hypomagnesemia and hypocalcemia
3601_e20_p438-453 2/19/02 8:59 AM Page 441
Seizures and Syncope in the Cancer Patient
and thus are easily prevented by magnesium and, if
of interferon, interleukin-2 (IL-2), lymphokine-acti-
necessary, calcium supplementation during the che-
vated killer cells, and some colony-stimulating fac-
motherapy infusion (Bachmeyer et al., 1996; Fuse-
tors (Dierckx et al., 1985; Karp et al., 1996; Meyers
et al., 1991). Transient lesions in the occipital poles,cerebellum, and centrum semiovale have been de-
5-Fluorouracil. Severe neurotoxicity with seizures,
scribed in patients treated with IL-2 who developed
encephalopathy, syncope, ataxia, motor neuropathy,
focal neurologic problems, including seizures (Karp
and demyelinating lesions evident on MRI scan has
been reported in patients treated with 5-fluorouracil(5-FU). These patients had an underlying dihydropy-
Intratumoral Therapies. Intratumoral therapies
rimidine dehydrogenase deficiency, an enzyme that is
seek to decrease systemic toxicity of a chemother-
responsible for the rate-limiting step of 5-FU catabo-
apeutic agent through a high level of regional drug
lism. This deficiency increased binding of 5-FU to
delivery. However, the risk of causing seizures is
thymidylate synthetase and incorporation into RNA
higher in those patients with a prior history of
tumor-related seizures. Increased frequency of
Pre-existing renal disease, which alters the clear-
seizures was noted in patients treated with intratu-
ance of chemotherapeutic agents, has been impli-
moral BCNU Wafers (Gliadel) (Brem et al., 1995);
cated in neurotoxicity, with seizures caused by treat-
seizures typically occurred in the first 5 days after
ment with chlorambucil and cytosine arabinoside.
surgery, although they were also observed at 20 to
Decreasing the dose of the chemotherapeutic agent
is recommended for such patients (Salloum et al.,1997; Smith et al., 1997). Ifosphamide (ifosfamide). Ifosphamide, commonlyused to treat sarcomas, medulloblastoma, and other
Narcotics. Cancer patients often require narcotics
pediatric and adult tumors, can cause severe neuro-
for control of pain. Narcotics occasionally cause
toxicity manifested by coma and seizures (Bhardwaj
neurotoxicity and seizures. Specific drugs associated
and Badesha, 1995; Gieron et al., 1988).
with the occurrence of seizures are meperidine (De-merol Hydrochloride), propoxyphene (Darvon),
Paclitaxel (Taxol). Paclitaxel is highly active against
and, rarely, morphine sulfate. In the case of meperi-
ovarian, breast, and other cancers (lung, uterine). It
dine, the metabolite normeperidine has been im-
is a mitotic spindle inhibitor, and it exerts its major
plicated. Renal dysfunction may contribute to, but
neurotoxic effect on peripheral nerves. Recent re-
is not the determining factor for, the accumulation
ports link paclitaxel-induced encephalopathy with
and neuroexcitatory effect of normeperidine (Goet-
seizures, particularly in those patients treated with
ting and Thirman, 1985; Kaiko et al., 1983; Szeto et
high doses (Nieto et al., 1999; Perry and Warner,
al., 1977). Seizures have been reported in patients
1996). Reversible encephalopathy and seizures have
who have been treated with an intravenous mor-
also been reported with vincristine. A brain biopsy
phine solution containing sodium bisulfate as a
specimen in one reported case revealed neurotubu-
preservative (Meisel and Welford, 1992). An in-
lar dissociation (Hurwitz et al., 1988).
trathecal or intraventricular morphine bolus canalso cause seizures (Kronenborg et al., 1998).
Cyclosporin. Immunosuppressant drugs such as cy-
Propoxyphene has been reported to cause status
closporin are given to bone marrow transplant re-
cipients to prevent rejection. These agents have beenreported to induce seizures in patients pretreated with
Antiemetics. Some neuroleptics used as antiemetics
busulfan or platinum compounds (Ghany et al.,
in conjunction with chemotherapy (phenothiazines,
butyrophenones) have been reported to induceseizures. This phenomenon appears to be dose re-
Biologic Response Modifiers. Encephalopathy and
lated. The newer antiemetics, such as ondansetron,
seizures have been reported after the administration
3601_e20_p438-453 2/19/02 8:59 AM Page 442
SYMPTOMS SECONDARY TO CANCER AND ITS TREATMENT
Antibiotics. Many cancer patients with neutropenia
(Avrahami et al., 1987), particularly in those patients
and depressed immune systems due to malignancy
who have primary or metastatic brain tumors. Con-
and chemotherapy receive broad-spectrum antibiot-
trast-induced seizures are caused by an increased
ics or multiple antibiotics. Some of these have been
susceptibility to seizures and increased permeability
associated with encephalopathy and seizures. Most of-
of the blood–brain barrier in these patients, and they
ten implicated are the quinolones and betalactams.
are possibly a direct toxic effect of the agents used
The neurotoxicity of the quinolones is dose related.
(Avrahami et al., 1989; Fischer, 1980).
Experimental studies have shown that this is becausegamma-aminobutyric acid–like substituents in the
structure of quinolones act as antagonists at the gamma-aminobutyric acid receptors (Akahane et
Metabolic abnormalities are the most common cause
al., 1989). Renal failure and the presence or history
of altered levels of consciousness in cancer patients.
of brain metastases are contributing factors (Walton
Hyponatremia, hypoglycemia, hypomagnesemia,
hypocalcemia, and hypoxia lower the seizure thresh-
Of the betalactams, imipenem/cilastatin (Pri-
old. Seizures caused by metabolic abnormalities tend
maxin) is the most neurotoxic. Betalactam neurotox-
to be generalized. The accompanying cerebral dys-
icity seems to be due to an increased concentration
function is diffuse, even in the rare case of a focal or
of the drug in brain tissue when it is given in high
complex partial seizure (Cascino, 1993; Stein and
doses or given to patients with impaired renal func-
tion or caused by alterations in the blood–brain bar-rier due to infection or malignancy (Bodey et al.,
Hyponatremia. Hyponatremia in cancer patients
1987). An impaired mechanism for clearance of the
can be caused by volume depletion or volume over-
drug from brain tissue may be involved, but this has
load, by drugs, or by a malignancy, such as occurs
not yet been documented (Schliamser et al., 1991).
with paraneoplastic syndrome. Intravascular volumedepletion occurs as a result of poor fluid intake, fluid
Methylphenidate (Ritalin). Patients with brain tu-
loss with emesis, or retention of fluid in the abdom-
mors or systemic cancer often experience fatigue,
inal cavity (ascites), either neoplastic or due to con-
lethargy, depressed mood, and overall neurobehav-
gestive heart failure. Aggressive hydration to enhance
ioral slowing. These symptoms can be caused by the
the renal clearance of some chemotherapeutic drugs
brain tumor itself or by the effects of RT and che-
(platinum, methotrexate) causes dilutional hypona-
motherapy. Methylphenidate has been shown to im-
prove patients’ energy level and function (Meyers et
The syndrome of inappropriate antidiuretic hor-
al., 1998; Weitzner et al., 1995). There is some con-
mone (SIADH) is another common cause of hypona-
cern, however, that the drug may increase the fre-
tremia in patients with cancer. As in paraneoplastic
quency of seizures in patients who have a history of
syndrome, it occurs most commonly in patients with
epilepsy or seizures due to the presence of brain tu-
small cell lung carcinoma and also in those with
mor. This association has been demonstrated by re-
Hodgkin’s lymphoma, non–small cell lung carci-
sults from studies of children with epilepsy and at-
noma, and cancer of the pancreas, colon, prostate,
tention deficit hyperactivity disorder (Gross-Tsur et
or adrenal cortex. Small cell lung carcinoma cells
al., 1997). In contrast, a study of patients with brain
produce arginine-vasopressin–like and atrial natri-
injury and epilepsy suggests that methylphenidate
uretic–like factors, two hormones implicated in para-
may actually decrease the frequency of seizures
neoplastic SIADH (Franck et al., 1987; Vanhees et al.,
(Wroblewski et al., 1992). In sum, the benefit of
2000). For other types of cancer, the production of
methylphenidate therapy for cancer patients with neu-
ectopic hormones is less well documented.
robehavioral slowing outweighs the remote risk of
SIADH also occurs in those patients with lep-
tomeningeal metastases, tumors involving the hypo-thalamus, and basilar meningitis. Drugs that can
Radiologic Contrast Medium. Intravenous contrast
cause the syndrome are carbamazepine, neuroleptics
media used for CT scans of the brain have been re-
(haloperidol [Haldol]), tricyclic antidepressants, and
ported to trigger either focal or generalized seizures
cytotoxics (Vinca alkaloids, cyclophosphamide). Cis-
3601_e20_p438-453 2/19/02 8:59 AM Page 443
Seizures and Syncope in the Cancer Patient
platin can cause SIADH with secondary seizures
syncope, massive pneumonitis, rapid progression of
(Ritch, 1988). Diagnosis is made on the basis of lab-
lung tumors, or metastatic lymphangitic spread. Pa-
oratory findings of hyponatremia, hypo-osmolality of
tients with pulmonary fibrosis secondary to chemo-
the serum, and increased urine osmolality. Renal, he-
therapy (bleomycin, nitrosoureas) or RT are also at
patic, adrenal, and pituitary function are normal.
It is important to correctly diagnose the cause of
hyponatremia to treat it appropriately. Hydration with
normal saline solution corrects the problem of fluiddepletion. Fluid restriction, sodium supplementation,
Cancer patients are very susceptible to infections, and
and sometimes diuretics are indicated to treat fluid
seizures occur in those patients who have systemic
overload. The treatment of SIADH consists of re-
infections or infectious processes in the CNS. Patients
stricting fluids, administering demeclocycline, and
undergoing high-dose chemotherapy with bone mar-
identifying and, if possible, removing the cause. Para-
row transplant are at particular risk. Central nervous
neoplastic SIADH usually resolves if the tumor can be
system infections associated with seizures can
removed or if it responds to radiation or chemo-
be caused by viruses (herpes simplex virus, cy-
therapy. The syndrome may recur, indicating tumor
tomegalovirus, herpes zoster virus); bacteria, includ-
recurrence (McDonald and Dubose, 1993; Richard-
ing common pathogens and opportunistic agents
(Listeria, Mycobacterium); fungi (Aspergillus,Cryptococcus); or parasites (Toxoplasma) (Bosi
Hypoglycemia. Hypoglycemia occurs in cancer pa-
et al., 1998; Pruitt, 1991). Clinically, patients with
tients who receive total parenteral nutrition and re-
seizures caused by infections present with confusion,
sults from either the insulin in the solution or with-
altered level of consciousness (encephalitis), menin-
drawal of total parenteral nutrition. Other causes are
gitic signs, or, in the case of abscess, focal findings.
malnutrition and pancreatic tumors (insulinoma)(Daggett and Nabarro, 1984; Hazard et al., 1985).
Seizures can occur with blood glucose levels below40 mg/dL; they are usually preceded by diaphoresis,
Cancer patients have both embolic and thrombotic
tremor, a sensation of hunger, and nervousness.
strokes. The pathogenesis of cerebrovascular eventsin these patients includes cancer- and treatment-
Hypocalcemia and Hypomagnesemia. Hypocalcemia
related causes (Graus et al., 1985).
and hypomagnesemia are two electrolyte abnormali-ties that have similar effects on the nervous system. Embolic Stroke. Embolic events can occur in the
Hypocalcemia and hypomagnesemia occur in patients
presence of cardiac arrhythmia, which occurs in pa-
who receive intensive chemotherapy, especially cis-
tients treated with paclitaxel, in those with cardiomy-
platin, with overhydration (Bachmeyer et al., 1996;
opathy secondary to doxorubicin, and in cancer-
Fuse-Nagase et al., 1997). Hypocalcemia has also
associated marantic endocarditis (Rosen and Arm-
been reported in patients treated with amphotericin
B. It occurs less commonly with malnutrition or inpatients with secondary hypoparathyroidism follow-
Thrombotic Stroke. Thrombotic strokes are ob-
ing treatment for thyroid cancer. Seizures are a com-
served in patients who have hypercoagulability syn-
mon manifestation of hypocalcemia because of the in-
dromes, paraneoplastic phenomena associated with
creased excitability of the cerebral cortex. Other
pancreatic cancer, breast carcinoma, and other ma-
clinical manifestations of hypocalcemia and hypo-
lignancies (Collins et al., 1975; Patronas and Argy-
magnesemia, including tremor, carpopedal spasm
ropoulou, 1992). Stroke in cancer patients can be
(tetany), and myoclonus, can sometimes be confused
caused by carotid artery stenosis following RT to the
neck for treatment of head and neck tumors or bycompression from neoplastic adenopathy. Radiother-
Hypoxia. Hypoxia is another potential, although less
apy to the brain can induce vasculopathy, another po-
common, cause of seizures in cancer patients. Acute
tential cause of ischemic stroke. Thrombotic and he-
hypoxia occurs with pulmonary embolism, prolonged
morrhagic strokes with secondary seizures have been
3601_e20_p438-453 2/19/02 8:59 AM Page 444
SYMPTOMS SECONDARY TO CANCER AND ITS TREATMENT
reported in children whose leukemias were treated
tient immediately before the seizure, the duration of
with L-asparaginase. L-asparaginase causes deficien-
the event and of the post-ictal period, and whether or
cies of antithrombin, plasminogen, fibrinogen, and
not there are residual mental status changes or focal
factors IX and XI (Priest et al., 1980). Chemother-
neurologic deficits. The clinician should also try to
apy-induced vascular events may be transient, and
obtain information about the administration of all
MRI scans may show areas of ischemia in the water-
medications before the seizure and the presence of
shed distribution (Pihko et al., 1993).
any signs of infection. It is important to elicit the pastmedical history, focusing on prior history of seizures,
Venous Sinus Thromboses. Venous sinus throm-
cardiac disease, pulmonary disease, diabetes, and
boses can occur with the secondary venous infarc-
head trauma. Common symptoms associated with
tions that can be caused by tumor invasion or meta-
seizures are headache, paresthesias, diaphoresis, dif-
static or infectious meningitis. Venous infarctions are
ficulty breathing, gastric discomfort, and occasionally
The physical and neurologic examinations will
Parenchymal and Intratumoral Hemorrhage. New-
help to identify the cause(s) of the seizure. The pres-
onset seizure or an increase in seizure frequency oc-
ence of focal neurologic deficits suggests that the pa-
curs in those patients with hemorrhage into a primary
tient has a focal intracranial lesion (parenchymal or
or metastatic brain tumor. Of the metastatic tumors,
dural/meningeal), either neoplastic, infectious (ab-
melanoma, renal cell carcinoma, and choriocarci-
scess, empyema), hemorrhagic, or vascular. Focal
noma are most commonly associated with hemor-
leukoencephalopathy secondary to RT or chemo-
therapy can also present with focal deficits. Alteredlevel of consciousness, myoclonus, and asterixis sug-
Spontaneous Subarachnoid Hemorrhage. While
subarachnoid hemorrhage may occur in patients who
The first seizure in a cancer patient should prompt
have a malignancy, it may not always be possible to
laboratory tests, including complete blood cell count,
elucidate the pathogenesis of the process. One cause
with differential and platelet counts; chemistry pro-
for subarachnoid hemorrhage or small cortical
file; assay of magnesium level; blood and urine cul-
parenchymal hemorrhage is CNS aspergillosis. It is
tures; and blood levels for drugs such as cyclosporin,
important to appreciate that subarachnoid hemor-
methotrexate, aminophylline, ethanol, and, if appro-
rhages can recur along with seizures as part of their
Contrast-enhanced gadopentetic acid–enhanced
MRI scan or CT scan of the brain can usually iden-
Traumatic Subdural or Subarachnoid Hemor-
tify intracranial lesions, leptomeningeal disease,
rhage. These hemorrhages can occur in cancer pa-
strokes, and hemorrhages. The extent of edema and
tients who are thrombocytopenic or who develop a
low-grade disseminated intravascular coagulation
Lumbar puncture is indicated for the diagnosis
syndrome. In such cases, even minor trauma may
of meningitis, leptomeningeal metastases, and sub-
arachnoid hemorrhage. It must be performed withgreat caution in patients who have an intracerebralmass or thrombocytopenia. Platelet transfusion may
Diagnosis
The diagnosis of seizures in cancer patients is made
Electroencephalography helps to identify the sei-
on the basis of a detailed history, physical and neu-
zure focus and differentiate between disease pro-
rologic examinations, laboratory tests, neuroimaging
cesses. Specific findings on electroencephalograms
results, and electroencephalographic findings. When
occur in herpesvirus encephalitis (periodic lateral-
taking the patient’s history, the clinician must try to
ized epileptiform discharges in the temporal lobes)
obtain an accurate description of the ictal event: tim-
and in some metabolic encephalopathies (triphasic
ing of the event in relation to the diagnosis of tumor
and the treatment for cancer, the presence or absence
The differential diagnosis must be made with other
of aura, elements of focality, the behavior of the pa-
paroxysmal events, such as syncope, myoclonic jerks,
3601_e20_p438-453 2/19/02 8:59 AM Page 445
Seizures and Syncope in the Cancer Patient
tetany, transient encephalopathy, transient ischemic
mal lesions. The use of prophylactic antiepileptic
attacks, and panic attacks, which can all mimic
drugs in patients with brain tumors who do not have
seizures is controversial (Cohen et al., 1988). In suchpatients, antiepileptic drugs may cause adverse ef-fects. Whether or not to use antiepileptic drugs is de-
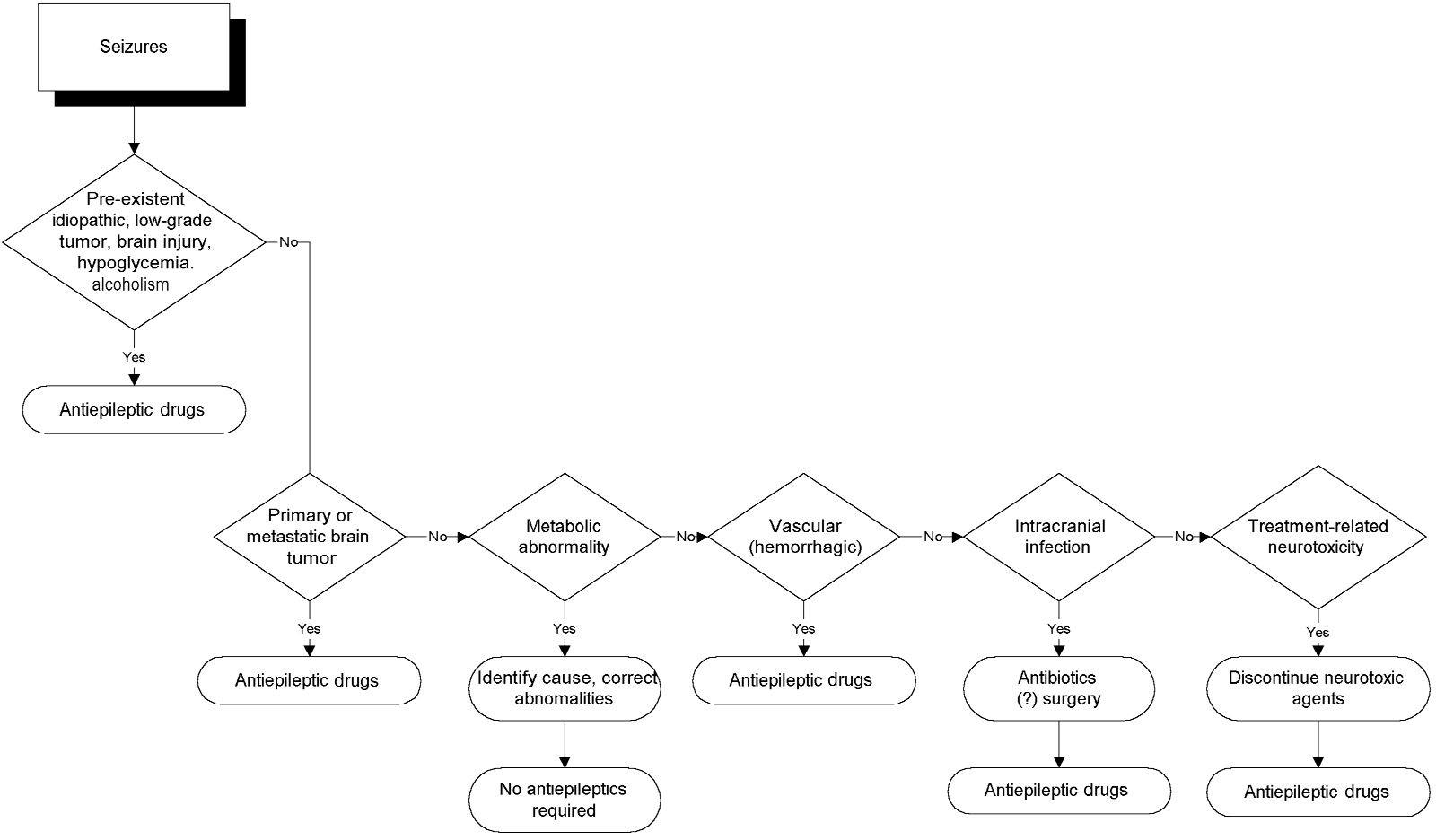
Treatment
termined by the patient’s condition and hepatic and
An algorithm for the management of seizures in can-
renal function and by the concurrent administration
cer patients is presented in Figure 21–1. To decide
of drugs that interfere with antiepileptic drugs’ me-
which therapy to use for ictal events, the neurologist
must answer two important questions: whether the
In patients with altered mental status, antiepilep-
event was a seizure and whether anticonvulsants are
tic drugs must be administered parenterally. The
drugs of choice are benzodiazepines, phenytoin, or
If the patient is in status epilepticus, efforts should
focus on stopping the seizures. Airway patency must
For treatment of generalized seizures, phenytoin is
be established, and intravenous therapy with benzo-
usually the first drug administered. For complex par-
diazepines (lorazepam, diazepam) and antiepileptic
tial seizures, carbamazepine may be the first-line
drugs (phenytoin, phenobarbital) must be initiated.
drug. Phenobarbital is the drug of choice for chil-
If the work-up indicates a toxic or metabolic cause
for the status epilepticus, antiepileptic drugs can bediscontinued once the seizures have stopped and their
cause has been eliminated. Any drugs known to beepileptogenic must be discontinued, the metabolic
Phenytoin is the most widely used antiepileptic drug
abnormalities must be corrected, and appropriate an-
in the United States. A known effective anticonvul-
tibiotic therapy must be instituted for infection, avoid-
sant, it has several advantages: It can be adminis-
tered by multiple routes (oral, intravenous, through
Long-term anticonvulsant treatment is indicated
a gastric tube in its elixir form); it has a long half-
for patients with a pre-existing seizure disorder, pri-
life, which allows once-a-day dosing; and it is inex-
mary or metastatic brain tumors, or other parenchy-
Figure 20–1. An algorithm for the management of seizures in the neuro-oncologic patient.
3601_e20_p438-453 2/19/02 8:59 AM Page 446
SYMPTOMS SECONDARY TO CANCER AND ITS TREATMENT
Problems associated with phenytoin are related to
therapy with busulfan (Fitzsimmons et al., 1990).
its pharmacokinetics. It is metabolized in the liver,
Phenytoin was also shown to selectively enhance the
and its serum levels are influenced by liver disease
cytotoxicity of microtubule inhibitors, such as Vinca
(metastatic or noncancer related) as well as by its
alkaloids; this activity is presently under investigation
multiple drug interactions (DeMonaco and Lawless,
for potential clinical use (Ganapathi et al., 1993).
1983; Gattis and May, 1996; Ghosh et al., 1992). Dex-amethasone, commonly used in patients with primary
and metastatic brain tumors as well as an adjuvantantiemetic in patients receiving chemotherapy, has
Carbamazepine and its newer derivative oxcar-
been demonstrated to lower phenytoin levels (Gattis
bazepine (Trileptal) is the anticonvulsant of choice
and May, 1996; Lackner, 1991). Platinum-containing
for patients with complex partial seizures, and it is
chemotherapy regimens have been reported to de-
used as a second-line antiepileptic drug for patients
crease phenytoin levels to as low as 25% of the ini-
with generalized seizures who either did not have ad-
tial therapeutic level, with return to baseline after
equate seizure control with phenytoin or developed
discontinuation of chemotherapy. Procarbazine, a
allergic reactions to it. When administered together
chemotherapeutic agent related to disulfiram, can
with phenytoin, carbamazepine decreases the pheny-
increase the level of phenytoin. Anticonvulsants also
toin level. It can only be administered orally or
increase the risk of procarbazine hypersensitivity re-
through a gastrostomy tube and therefore cannot be
actions (Lehmann et al., 1997). The phenytoin dose
used in emergency situations. The main difficulty with
needs to be adjusted and the levels monitored closely
using carbamazepine in cancer patients is its myelo-
in those patients receiving chemotherapy to avoid un-
toxic effect, which causes neutropenia, lymphopenia,
der dosing and toxic effects (Neef and de Voogd-van
and aplastic anemia (Silverman and Chapron, 1995).
der Straaten, 1988; Grossman et al., 1989; Ghosh et
These problems limit its use in patients who are re-
al., 1992). Phenytoin also increases clearance and
ceiving chemotherapy. Furthermore, carbamazepine
may thus decrease the efficacy of chemotherapeutic
levels are decreased by chemotherapeutic drugs such
agents such as busulfan, paclitaxel, topotecan and re-
as platinum (Jain, 1993). Carbamazepine also causes
lated drugs (Grossman et al., 1998; Hassan et al.,
SIADH. Like phenytoin, carbamazepine can cause
1993; Zamboni et al., 1998). Because of decreased
allergic reactions, including Stevens-Johnson syn-
protein binding and increased free plasma drug lev-
els, the dose must be decreased for patients who arebeing treated with warfarin or cimetidine.
Both total and free phenytoin levels should be
monitored in patients who have impaired renal func-
Valproic acid and its derivative divalproex sodium
tion because phenytoin excretion may be impaired.
(Depakote) are used for patients with seizures that
Seizures can occur in cancer patients receiving
are not controlled by phenytoin. The drugs are ad-
phenytoin when subtherapeutic levels of the drug are
ministered orally and are metabolized in the liver.
administered, and they can also occur as a manifes-
When administered together with phenytoin, val-
tation of phenytoin toxicity. Phenytoin can cause al-
proate can either decrease or increase phenytoin lev-
lergic reactions, usually a cutaneous rash. Severe re-
els. Methotrexate has been reported to cause an acute
actions, including Stevens-Johnson syndrome, have
decline in the level of serum valproate (Schroeder
been described in patients being weaned from corti-
and Ostergaard, 1994). Reported toxic effects that
costeroids while receiving RT to the brain (Delattre
limit its use in cancer patients are hepatotoxicity, pro-
longed bleeding time, and dose-dependent thrombo-
In vitro, but not in vivo, studies indicated a possi-
ble radiosensitizing effect of phenytoin on astrocy-toma cells (Lordo et al., 1987). Phenytoin and other
enzyme inducers were reported to have a protectiveeffect in patients receiving busulfan, reducing its neu-
Phenobarbital remains the drug of choice for con-
rotoxicity and myelotoxicity. Phenytoin is now used
trolling seizures in children. It is mainly used as an
for seizure prophylaxis in patients receiving chemo-
adjunct to phenytoin or for adult patients for whom
3601_e20_p438-453 2/19/02 8:59 AM Page 447
Seizures and Syncope in the Cancer Patient
other anticonvulsants have failed. Its main side effect
vulsants and as adjuncts for better seizure control by
is somnolence, although some patients experience
patients who fail anticonvulsant monotherapy. Conclusions
Seizures are a common neurologic problem in pa-
A new class of antiepileptic drug, GABA agonists, has
tients with systemic and CNS malignancies and may
recently been released to the marketplace, and there
have multiple etiologies. Examination should be
is not much experience with their use by cancer pa-
aimed at identifying and treating all of its possible
tients. Neurontin is purported to cause fewer side ef-
causes. The treatment of seizures in cancer patients
fects than conventional antiepileptic drugs, but there
must be individualized, and metabolic factors and
have been no studies to evaluate its interactions, if
drug interactions must be taken into consideration
any, with chemotherapeutic agents. Because it has so
when anticonvulsant therapy is initiated.
few side effects, it is commonly used in combinationwith phenytoin, carbamazepine, or valproate for braintumor patients with refractory complex partial
Syncope is defined as a sudden transient loss of con-sciousness and postural tone with spontaneous re-
covery. The frequency of syncope in cancer patients
Lamotrigine is a new, structurally unique, anticon-
is not well documented. Presyncope, with premoni-
vulsant that acts on voltage-dependent sodium chan-
tory symptoms but without loss of consciousness
nels, resulting in decreased release of excitatory neu-
(“faint feeling”), is probably even more common
rotransmitters. It is indicated for treatment of partial
(Plum and Posner, 1982). Syncope occurs because
seizures but can cause severe dermatologic side ef-
of a transient interruption of cerebral blood flow.
fects and myelotoxicity. It has known interactions with
Common presyncopal symptoms are dizziness, light-
other anticonvulsants, but to date there are no re-
headedness, palpitations, diaphoresis, and, occa-
ports of interactions with chemotherapeutic drugs.
Lamotrigine is a dehydrofolate reductase inhibitorand should not be used by patients treated with
Etiology
methotrexate and other antimetabolites.
The etiology of syncope in cancer patients is pre-sented in Table 20–2. As in the case of seizures, sev-
eral etiologic factors may contribute to syncope in
Topiramate is another new anticonvulsant used as ad-
cancer patients, the most common being orthostatic
junctive therapy for partial seizures. It acts on sodium
hypotension, with cardiac causes assuming a sec-
channels and as a GABA agonist. It produces no sig-
ondary role. Other causes are drugs, vasovagal reac-
nificant drug interactions, and its main side effect is
tions, and cerebrovascular disease (Kapoor, 1991,
psychomotor slowing. Topamax may cause leuko-
Orthostatic hypotension is commonly present in the
Gabitril is another new GABA-ergic anticonvulsant,
terminal stages of cancer in those patients who are
which is indicated as an adjunctive treatment of com-
suffering from malnutrition and dehydration. It also
plex partial seizures. It has no significant drug inter-
occurs in those who become dehydrated from eme-
actions, and it can be safely used with enzyme-
sis caused by chemotherapy. Patients with severe ane-
inducing drugs. Rarely, it may cause anemia and
mia often present with syncope or presyncope caused
thrombocytopenia. These new drugs can be used by
by insufficient oxygenation of the brain rather than
patients with known allergy to the first-line anticon-
from volume depletion. The drop in blood pressure
3601_e20_p438-453 2/19/02 8:59 AM Page 448
SYMPTOMS SECONDARY TO CANCER AND ITS TREATMENT
Table 20-2. Etiology of Syncope in Patients with Malignancy
Platinum compounds, Vinca alkaloids, taxanes, diabetes
Tricyclic antidepressants, vasodilators, diuretics
Chemotherapeutic agents (fluorouracil, Vinca alkaloids, platinum compounds, taxanes),
CNS depressants (barbiturates), biologic response modifiers
Nutritional, pancreatic tumors (insulinoma)
Parapharyngeal tumors, radiation therapy to neck
Myocardial ischemia (mediastinal radiation, atherosclerosis), cardiomyopathy (adriamycin,
Chemotherapy (paclitaxel, interleukin-2), mediastinal radiation, pre-existing cardiac disease
Micturition, coughing, swallowing, strong emotional stimuli
with change in position is accompanied by an in-
Syncope is also part of the spectrum of direct neu-
creased heart rate. Chemotherapeutic agents such as
rotoxic effects of chemotherapeutic drugs such as flu-
cisplatin and Vinca alkaloids cause a peripheral neu-
orouracil (Hook et al., 1992; Shehata et al., 1999).
ropathy with dysautonomia. The heart rate does not
Biologic response modifiers and colony-stimulating
increase significantly with the drop in blood pressure
factors also cause hypotension with syncope or near-
in patients who have this condition.
Another common cause of orthostatic hypotension
in cancer patients is related to drugs such as diuret-
ics and antidepressants. The pathogenetic mechanismof orthostasis in patients taking diuretics is intravas-
Syncope in hypoglycemic patients has a fairly typical
cular volume depletion, whereas antidepressants,
clinical presentation, which suggests its diagnosis. It
neuroleptics, and some antiemetics cause an anti-
is preceded by a sensation of hunger. The patient be-
cholinergic effect. Hypotension with possible presyn-
comes irritable, tremulous, and diaphoretic and may
cope or syncope is a common side effect of biologic
complain of dimming vision. The skin becomes pale.
agents such as interferon, IL-2, and tumor necrosis
Loss of consciousness is brief and is usually not fol-
factor. Orthostatic presyncope and syncope also oc-
lowed by confusion; however, with severe hypo-
cur in patients with severe infections that cause high
glycemia, there may be associated seizure activity. Hy-
poglycemia occurs in patients who have insulinoma,malnutrition, and insulin-dependent diabetes and canbe caused by insulin overdosing from total parenteral
nutrition. The symptoms of patients with insulinoma
Syncope can be a side effect of medications, even in
typically occur in the morning, before breakfast, or
the absence of other etiologic factors. The mechanisms
between meals (Daggett and Nabarro, 1984; Hazard
are orthostatic hypotension either through volume de-
pletion (diuretics, mannitol), vasopressor effects (bi-ologic response modifiers), anticholinergic effects
(antidepressants), cardiac arrhythmia (paclitaxel, in-travenous phenytoin), or peripheral neuropathy (vin-
Syncope is a common manifestation of cardiac dis-
cristine, paclitaxel, platinum compounds).
ease. Cancer patients can experience the same prob-
3601_e20_p438-453 2/19/02 8:59 AM Page 449
Seizures and Syncope in the Cancer Patient
lems that patients without malignancy do. The main
neuralgia–asystole syndrome, carotid sinus syndrome,
pathogenetic mechanisms for syncope of cardiac ori-
and glossopharyngeal-related reflex cardiogenic
gin are pump failure, heart blocks, and arrhythmias.
syncope without neuralgic pain (Cicogna et al., 1993;
Pump failure occurs in myocardial infarction or
Dykman et al., 1981; Wang and Ng, 1995). Na-
cardiomyopathy. In cancer patients, cardiomyopathy
sopharyngeal and parapharyngeal carcinomas cause
can be caused by chemotherapy with anthracyclines,
these syndromes. In these patients, syncope does not
especially daunorubicin, which may be irreversible.
respond to medical management or in some cases to
Other cardiotoxic chemotherapeutic agents are mi-
pacemaker insertion. Syncope may resolve after treat-
toxantrone and estramustin. The risk for cardiac
ment of the tumor or may require intracranial inter-
disease increases if such drugs are administered fol-
vention to resect the glossopharyngeal nerve.
lowing RT to the chest and mediastinum. Viral my-ocarditis in the immunosuppressed patient and
graft-versus-host disease following allogeneic bonemarrow transplant are other causes of heart failure.
Vasovagal syncope is one of the most common types
Heart failure patients usually have symptoms sugges-
of syncope in young adults, and patients usually pres-
tive of myocardial ischemia before syncope: chest
ent with a history of prior syncopal episodes. Vaso-
pain, dyspnea, and signs of heart failure.
vagal syncope occurs in response to stress, pain,
Heart blocks and cardiac arrhythmias in cancer
fear, and heat and is preceded by symptoms such as
patients are usually caused by a pre-existing cardiac
palpitations, queasiness, nausea, diaphoresis, and
condition. Arrhythmias do occasionally result from
abdominal discomfort. Incontinence is uncommon.
paclitaxel or IL-2 therapy. Several case reports of syn-
The underlying pathophysiologic mechanism is
cope describe cardiac arrhythmias, coronary artery
thought to be a reflex withdrawal of sympathetic tone
stenosis, and defective cardiovascular reflexes in pa-
(Bezold-Jarisch reflex), indicated clinically by tachy-
tients who were treated with RT to the mediastinum
cardia, followed by bradycardia, pallor, and hy-
or neck (de Waard et al., 1996; Mary-Rabine et al.,
potension. Syncope that occurs during micturition or
1980; Shapiro et al., 1996). Syncope occasionally oc-
defecation (situational syncope), typically after a
curs after obstruction of pulmonary flow caused by
long period of bed rest, is more common in men
Diagnosis
Syncope can be a manifestation of cerebrovascular
The diagnosis of syncope is made primarily on
disease in the anterior or posterior circulation and
the basis of the patient’s clinical presentation (if the
may or may not be associated with focal neurologic
episode is witnessed) or an accurate and detailed his-
deficits. Possible causes of altered cerebral blood
tory. The history should include data on the patient’s
flow in cancer patients include compression of the
complaints before the loss of consciousness, appear-
carotid artery by tumor, stenosis of the subclavian or
ance of the patient (skin pale or flushed, diaphore-
carotid arteries following RT to the chest or neck, and
sis, breathing pattern), duration of the episode,
thrombotic or embolic events. When syncope occurs
associated seizure activity, incontinence, and the
after elevation or exertion of the left arm, a subcla-
presence or absence of confusion. Information
vian steal must be suspected, and blood pressure
should also be obtained about the patient’s past med-
ical history with regard to cardiac disease, hyperten-sion or hypotension, diabetes and hypoglycemia, typeof cancer, psychiatric history, medications, and cir-
cumstances of the event (micturition or defecation,
Patients with head and neck tumors, thyroid tumors,
crowded or overheated area, pain, stress). The phys-
and cervical lymphadenopathy can develop recurrent
ical and neurologic examinations, if feasible at or
syncope related to carotid sinus hypersensitivity. Syn-
near the time of the event, can reveal the presence of
cope in patients with head and neck tumors can oc-
hypotension, arrhythmia, or focal findings suggestive
cur through several mechanisms: glossopharyngeal
of a vascular or neoplastic brain lesion.
3601_e20_p438-453 2/19/02 8:59 AM Page 450
SYMPTOMS SECONDARY TO CANCER AND ITS TREATMENT
Examination should include measurement of blood
Treatment
pressure and heart rate in both supine and standing
Syncope is a brief, usually fully reversible, episode of
positions and in both arms to determine the presence
loss of consciousness that generally does not require
of position hypotension or the subclavian steal syn-
specific treatment. However, when the cause of syn-
drome. Auscultation of the heart can reveal arrhyth-
cope is a life-threatening condition such as a heart
mias and/or cardiac valve abnormalities. Cardiac
block, malignant arrhythmia, or pulmonary embolus,
monitoring, echocardiogram, and laboratory tests
close monitoring and urgent appropriate treatment
also help the clinician make the diagnosis. Labora-
must be instituted. Insertion of a cardiac pacemaker
tory tests should include hemoglobin, hematocrit,
and, in some cases, intracranial section of the glos-
white blood cell count, differential count, and platelet
sopharyngeal nerve are necessary. In simple syncope,
count to rule out anemia and infection; electrolyte,
the elimination of the causative agent(s) usually pre-
glucose, calcium, and magnesium levels; drug levels
vents further occurrences. Supportive therapy, main-
when appropriate (psychotropics and antidepres-
tenance of good nutritional status, hydration or blood
sants, opiates, barbiturates); and blood and urine cul-
transfusions to maintain adequate intravascular vol-
ume, correction of hypoglycemia and electrolyte ab-
When focal neurologic deficits are present, a CT
normalities, and discontinuation of offending drugs
or MRI scan of the brain is indicated. Electroen-
can prevent the occurrence of syncope in cancer pa-
cephalography is helpful in the differential diagnosis
tients (Benitez del Rosario and Salinas Martin, 1997).
with seizures, especially in patients with focal neuro-logic deficits if seizure activity has been witnessedduring syncope (Hoefnagels et al., 1991). Hypo-
REFERENCES
glycemic syncope and the syncope in Adams-Stokessyndrome (third-degree heart block) can be associ-
Ahern GL, O’Connor M, Dalmau J, et al. 1994. Paraneoplastic
temporal lobe epilepsy with testicular neoplasm and atypi-
Upright tilt-table testing is useful for diagnosing
cal amnesia. Neurology 44:1270–1274.
vasovagal syncope. It is performed by measuring
Akahane K, Sekiguchi M, Une T, Osada Y. 1989. Structure–
blood pressure and heart rate (continuous electro-
epileptogenicity relationship of quinolones with special ref-erence to their interaction with gamma-aminobutyric acid
cardiogram) in the supine position and then bring-
receptor sites. Antimicrob Agents Chemother 33:1704–
ing the patient suddenly to an upright position on the
tilt table and maintaining the upright position until
Antonini G, Ceschin V, Morino S, et al. 1998. Early neurologic
presyncope or syncope occurs in association with hy-
complications following allogeneic bone marrow transplant
potension and/or tachycardia. The test can be per-
for leukemia: a prospective study. Neurology 50:1441–1445.
formed with or without infusion of isoproterenol
Avrahami E, Weiss-Peretz J, Cohn DF. 1987. Focal epileptic ac-
(Kapoor, 1992). Lumbar puncture is usually not in-
tivity following intravenous contrast material injection in pa-
dicated except when meningitis or meningeal metas-
tients with metastatic brain disease. J Neurol Neurosurg Psy-
The differential diagnosis must be made taking into
Avrahami E, Weiss-Peretz J, Cohn DF. 1989. Epilepsy in pa-
tients with brain metastases triggered by intravenous con-
account all factors that can cause altered level of con-
trast medium. Clin Radiol 40:422–423.
sciousness, including seizures, encephalopathy, cere-
Bachmeyer C, Decroix Y, Medioni J, et al. 1996. [Hypomag-
bral ischemia, brain concussion, and drug or alco-
nesemic and hypocalcemic coma, convulsions and ocular
hol intoxication. In these cases, loss of consciousness
motility disorders after chemotherapy with platinum com-
is of longer duration, and the history and physical ex-
pounds]. Rev Med Interne (Paris) 17:467–469.
Bartolomei JC, Christopher S, Vives K, Spencer DD, Piepmeier
aminations establish the diagnosis. Psychiatric con-
JM. 1997. Low-grade glioma of chronic epilepsy: a distinct
ditions such as conversion reactions, generalized anx-
clinical and pathological entity. J Neurooncol 34:79–84.
iety disorder with hyperventilation, and panic attacks
Benitez del Rosario MA, Salinas Martin A. 1997. Hydration for
must also be considered. Information about psy-
control of syncope in palliative care. J Pain Symptom Man-
chotropic and antidepressant medications should be
Bernini JC, Fort DW, Griener JC, Kane BJ, Chappell WB, Ka-
obtained from patients who have a psychiatric
men BA. 1995. Aminophylline for methotrexate-induced
neurotoxicity. Lancet 345:544–547.
3601_e20_p438-453 2/19/02 8:59 AM Page 451
Seizures and Syncope in the Cancer Patient
Bhardwaj A, Badesha PS. 1995. Ifosfamide-induced noncon-
hairy cell leukemia treated with interferon. Clin Neurol Neu-
vulsive status epilepticus. Ann Pharmacother 29:1237–
Drislane FW. 1994. Nonconvulsive status epilepticus in patients
Blaney SM, Balis FM, Poplack DG. 1991. Pharmacologic ap-
with cancer. Clin Neurol Neurosurg 96:314–318.
proaches to the treatment of meningeal malignancy. On-
Dykman TR, Montgomery EB Jr, Gerstenberger PD, Zeiger HE,
Clutter WE, Cryer PE. 1981. Glossopharyngeal neuralgia
Bodey GP, Elting L, Jones P, Alvarez ME, Rolston K, Fainstein
with syncope secondary to tumor. Treatment and patho-
V. 1987. Imipenem/cilastatin therapy of infections in can-
Feun LG, Savaraj N, Lee YY, et al. 1991. A pilot clinical and
Bosi A, Zazzi M, Amantini A, et al. 1998. Fatal herpesvirus 6
pharmacokinetic study of intracarotid cisplatin and
encephalitis after unrelated bone marrow transplant. Bone
bleomycin. Sel Cancer Ther 7:29–36.
Fischer HW. 1980. Occurrence of seizures during cranial com-
Brem H, Piantadosi S, Burger PC, et al. 1995. Placebo-
puted tomography. Radiology 137:563–564.
controlled trial of safety and efficacy of intraoperative con-
Fitzsimmons WE, Ghalie R, Kaizer H. 1990. The effect of he-
trolled delivery by biodegradable polymers of chemother-
patic enzyme inducers on busulfan neurotoxicity and myelo-
apy for recurrent gliomas. The Polymer-Brain Tumor Treat-
toxicity. Cancer Chemother Pharmacol 27:226–228.
Flowers A, Levin VA. 1993. Management of brain metastases
Britton JW, Cascino GD, Sharbrough FW, Kelly PJ. 1994. Low-
from breast carcinoma. Oncology (Huntingt) 7:21–26.
grade glial neoplasms and intractable partial epilepsy: effi-
Franck G, Sadzot B, Salmon E, et al. 1987. [Paraneoplastic
cacy of surgical treatment. Epilepsia 35:1130–1135.
limbic encephalopathy, inappropriate ADH secretion and
Cascino GD. 1990. Epilepsy and brain tumors: implications for
recurrent subclinical epileptic seizures. Clinical, anatomo-
treatment. Epilepsia 31[suppl 3]:S37–S44.
pathological and metabolic correlations by positron emis-
Cascino TL. 1993. Neurologic complications of systemic can-
sion tomography]. Rev Neurol (Paris) 143:657–669.
cer. Med Clin North Am 77:256–278.
Fuse-Nagase Y, Suwa K, Nagao Y. 1997. Partial seizures asso-
Ciaudo-Lacroix C, Lapresle J. 1985. [Pseudo-tumoral form of
ciated with cisplatin administration: a case report. Clin Elec-
delayed radionecrosis of the brain]. Ann Med Interne
Ganapathi R, Hercberg A, Grabowski D, Ford J. 1993. Selec-
Cicogna R, Bonomi FG, Curnis A, et al. 1993. Parapharyngeal
tive enhancement of vincristine cytotoxicity in multidrug-re-
space lesions syncope-syndrome. A newly proposed reflex-
sistant tumor cells by dilantin. Cancer Res 35:3262–3265.
ogenic cardiovascular syndrome. Eur Heart J 14:1476–
Gattis WA, May DB. 1996. Possible interaction involving pheny-
toin, dexamethasone and antineoplastic agents: a case re-
Cohen N, Strauss G, Lew R, Silver D, Recht L. 1988. Should
port and review. Ann Pharmacother 30:520–526.
prophylactic anticonvulsants be administered to patients
Genvresse I, Dietzmann A, Massenkeil G, Spath-Schwalbe E,
with newly diagnosed brain metastases? A retrospective
Possinger K. 1999. Subacute encephalopathy after combina-
analysis. J Clin Oncol 6:1621–1624.
tion chemotherapy including moderate-dose methotrexate in
Collins RC, Al-Mondhiry H, Chernik NL, Posner JB. 1975. Neu-
a patient with gastric cancer. Anticancer Drugs 10:293–294.
rologic manifestations of intravascular coagulation in pa-
Ghany AM, Tutschka PJ, McGhee RB Jr, et al. 1991. Cy-
tients with cancer. A clinicopathologic analysis of 12 cases.
closporine-associated seizures in bone marrow transplant
recipients given busulfan and cyclophosphamide prepara-
Daggett P, Nabarro J. 1984. Neurological aspects of insulino-
tive therapy. Transplantation 52:310–315.
Ghosh C, Lazarus HM, Hewlett JS, Creger RJ. 1992. Fluctua-
Dalmau J, Graus F, Rosenblum MK, Posner JB. 1992. Anti-
tion of serum phenytoin concentrations during autologous
Hu–associated paraneoplastic encephalomyelitis/sensory
bone marrow transplant for primary central nervous sys-
neuronopathy. A clinical study of 71 patients. Medicine
tem tumors. J Neurooncol 12:25–32.
Gieron MA, Barak LS, Estrada J. 1988. Severe encephalopathy
Delattre JY, Safai B, Posner JB. 1988. Erythema multiforme
associated with ifosfamide administration in two children
and Stevens-Johnson syndrome in patients receiving cranial
with metastatic tumors . J Neurooncol 6:29–30.
irradiation and phenytoin. Neurology 38:194–198.
Goetting MG, Thirman MJ. 1985. Neurotoxicity of meperidine.
DeMonaco HJ, Lawless LM. 1983. Variability of phenytoin pro-
tein binding in epileptic patients. Arch Neurol 40:481–483.
Graus F, Rogers LR, Posner JB. 1985. Cerebrovascular com-
de Toffol B, Uchuya M, Michalak S, Corcia P, Hommet C, Autret
plications in patients with cancer. Cancer 64:16–35.
A. 1997. [Paraneoplastic encephalomyeloneuritis with anti-
Grossman SA, Hochberg F, Fisher J, et al. 1998. Increased 9-
Hu antibodies and cancer of the rectum]. Rev Neurol
aminocamptothecin dose requirements in patients on anti-
convulsants. NABTT CNS Consortium. The New Approaches
de Waard DE, Verhorst PM, Visser CA. 1996. Exercise-induced
to Brain Tumor Therapy. Cancer Chemother Pharmacol
syncope as late consequence of radiotherapy. Int J Cardiol
Grossman SA, Sheidler VR, Gilbert MR. 1989. Decreased
Dierckx RA, Michotte A, Schmedding E, Ebinger G, Degeeter
phenytoin levels in patients receiving chemotherapy. Am J
T, van Camp B. 1985. Unilateral seizures in a patient with
3601_e20_p438-453 2/19/02 8:59 AM Page 452
SYMPTOMS SECONDARY TO CANCER AND ITS TREATMENT
Gross-Tsur V, Manor O, van der MJ, Meere J, Joseph A, Shalev
Lovblad K, Kelkar F, Ozdoba C, Ramelli G, Remonda L, Schroth
RS. 1997. Epilepsy and attention deficit hyperactivity disorder:
G. 1998. Pure methotrexate encephalopathy presenting with
is methylphenidate safe and effective? J Pediatr 130:670–674.
seizures: CT and MRI features. Pediatr Radiol 28:86–91.
Hassan M, Oberg G, Bjorkholm M, Wallin I, Lindgren M. 1993.
Manolis AS, Linzer M, Salem D, Estes NA 3rd. 1990. Syncope:
Influence of prophylactic anticonvulsant therapy on high-
current diagnostic evaluation and management. Ann Intern
dose busulfan kinetics. Cancer Chemother Pharmacol
Mary-Rabine L, Waleffe A, Kulbertus HE. 1980. Severe con-
Hazard J, Simon D, Perlemuter L, et al. 1985. [Insulinoma:
duction disturbances and ventricular arrhythmias compli-
diagnostic elements. 13 cases]. Presse Med (Paris)
cating mediastinal irradiation for Hodgkin’s disease: a case
report. Pacing Clin Electrophysiol 3:612–617.
Hoefnagels WA, Padberg GW, Overweg J, Roos RA, van Dijk
McDonald GA, Dubose TD Jr. 1993. Hyponatremia in the can-
JG, Kamphuisen HA. 1991. Syncope or seizure? The diag-
cer patient. Oncology (Huntingt) 7:55–64.
nostic value of the EEG and hyperventilation test in tran-
Meisel SB, Welford PK. 1992. Seizures associated with high-
sient loss of consciousness. J Neurol Neurosurg Psychiatry
dose intravenous morphine containing sodium bisulfite
preservative. Ann Pharmacother 26:1515–1517.
Hook CC, Kimmel DW, Kvols LK, et al. 1992. Multifocal in-
Menendez LR, Bacon W, Kempf RA, Moore TM. 1990. Fat em-
flammatory leukoencephalopathy with 5-fluorouracil and
bolism syndrome complicating intraarterial chemotherapy
levamisole. Ann Neurol 31:262–267.
with cis-platinum. Clin Orthop 254:294–297.
Hurwitz RL, Mahoney DH Jr, Armstrong DL, Browder TM.
Meyers CA, Obbens EA, Scheibel RS, Moser RP. 1991. Neuro-
1988. Reversible encephalopathy and seizures as a result
toxicity of intraventricularly administered alpha-interferon
of conventional vincristine administration. Med Pediatr On-
for leptomeningeal disease. Cancer 68:88–92.
Meyers CA, Weitzner MA, Valentine AD, Levin VA. 1998.
Jain KK. 1993. Investigation and management of loss of effi-
Methylphenidate therapy improves cognition, mood, and func-
cacy of an antiepileptic medication using carbamazepine as
tion of brain tumor patients. J Clin Oncol 16:2522–2527.
an example. J R Soc Med 86:133–136.
Neef C, de Voogd-van der Straaten I. 1988. An interaction be-
Kaiko RF, Foley KM, Grabinski PY, et al. 1983. Central ner-
tween cytostatic and anticonvulsant drugs. Clin Pharmacol
vous system excitatory effects of meperidine in cancer pa-
Newelt EA, Dahlborg SA. 1987. Chemotherapy administered in
Kapoor WN. 1991. Diagnostic evaluation of syncope. Am J Med
conjunction with osmotic blood–brain barrier modification
in patients with brain metastases. J Neurooncol 4:195–207.
Kapoor WN. 1992. Evaluation and management of the patient
Nieto Y, Cagnoni PJ, Bearman SI, et al. 1999. Acute en-
cephalopathy: a new toxicity associated with high-dose pa-
Karp BI, Yang JC, Khorsand M,, et al. 1996. Multiple cerebral
clitaxel. Clin Cancer Res 5:501–506.
lesions complicating therapy with interleukin-2. Neurology
Patronas NJ, Argyropoulou M. 1992. Intravascular thrombo-
sis as a possible cause of transient cortical brain lesions:
Kramer ED, Packer RJ, Ginsberg J, et al. 1997. Acute neuro-
CT and MRI. J Comput Assist Tomogr 16:849–855.
logic dysfunction associated with high-dose chemotherapy
Perry JR, Warner E. 1996. Transient encephalopathy after pa-
and autologous bone marrow rescue for primary malignant
clitxel (Taxol) infusion. Neurology 46:1596–1599.
brain tumors. Pediatr Neurosurg 27:230–237.
Pihko H, Tyni T, Virkola K, et al. 1993. Transient ioschemic
Kronenberg MF, Laimer I, Rifici C,, et al. 1998. Epileptic
cerebral lesions during induction chemotherapy for acute
seizures associated with intracerebroventricular and in-
lymphoblastic leukemia. J Pediatr 123:718–724.
trathecal morphine bolus. Pain 75:383–387.
Plum F, Posner JB. 1982. The Diagnosis of Stupor and Coma,
Lackner TE. 1991. Interaction of dexamethasone with pheny-
3rd ed. Philadelphia: FA Davis, pp 210–211.
Priest JR, Ramsay NK, Latchaw RE,, et al. 1980. Thrombotic
Lee AC, Wong K W, Fong K W, So K T. 1997. Intrathecal
and hemorrhagic strokes complicating early therapy
methotrexate overdose. Acta Paediatr 86:434–437.
for childhood acute lymphoblastic leukemia. Cancer
Lehmann DF, Hurteau TE, Newman N, Coyle TE. 1997. Anti-
convulsant usage is associated with an increased risk of
Pruitt AA. 1991. Central nervous system infections in cancer
procarbazine hypersensitivity reactions in patients with
brain tumors. Clin Pharmacol Ther 62:225–229.
Quinn CT, Griener JC, Bottiglieri K, Hyland K, Farrow A, Ka-
Lieschke GJ, Cebon J, Morstyn G. 1989. Characterization of the
men BA. 1997. Elevation of homocysteine and excitatory
clinical effects after the first dose of bacterially synthesized
amino acid neurotransmitters in the CSF of children who
recombinant human granulocyte-macrophage colony-stim-
receive methotrexate for the treatment of cancer. J Clin On-
ulating factor. Blood 74:2634–2643.
Lim SH, So NK, Luders H, Morris HH, Turnbull J. 1991. Etio-
Resar LM, Phillips PC, Kastan MB, Leventhal BG, Bowman PW,
logic factors for unitemporal vs bitemporal epileptiform dis-
Civin CI. 1993. Acute neurotoxicity after intrathecal cyto-
charges. Arch Neurol 48:1225–1228.
sine arabinoside in two adolescents with acute lym-
Lordo CD, Stroude EC, Del Maestro RF. 1987. The effects of
phoblastic leukemia of B-cell type. Cancer 71:117–123.
diphenylhydantoin on murine astrocytoma radiosensitivity.
Richardson GE. 1995. Hyponatremia of malignancy. Crit Rev
3601_e20_p438-453 2/19/02 8:59 AM Page 453
Seizures and Syncope in the Cancer Patient
Rider WD. 1963. Radiation damage to the brain—a new syn-
Spencer MD. 1998. Leukoencephalopathy after CNS prophy-
drome. J Can Assoc Radiol 14:67–69.
laxis for acute lymphoblastic leukaemia. Pediatr Rehabil
Ritch PS. 1988. Cis-dichlorodiammineplatinum II–induced
syndrome of inappropriate secretion of antidiuretic hor-
Stein DA, Chamberlain MC. 1991. Evaluation and management
of seizures in the patient with cancer. Oncology (Huntingt)
Rogers LR, Morris HH, Lupica K. 1993. Effect of cranial irra-
diation on seizure frequency in adults with low-grade as-
Stewart DJ, Belanger JM, Grahovac Z, et al. 1992. Phase I study
trocytoma and medically intractable epilepsy. Neurology
of intracarotid administration of carboplatin. Neurosurgery
Rosen P, Armstrong D. 1973. Nonbacterial thrombotic endo-
Szeto HH, Inturrisi CE, Houde R, Saal S, Cheigh J, Reidenberg
carditis in patients with malignant aneoplastic diseases. Am
MM. 1977. Accumulation of normeperidine, an active me-
tabolite of meperidine, in patients with renal failure of can-
Rosner D, Nemoto T, Lane WW. 1986. Chemotherapy induces
regression of brain metastases in breast carcinoma. Can-
Tahsildar HI, Remler BF, Creger RJ, et al. 1996. Delayed, tran-
sient encephalopathy after marrow transplantation: case re-
Salloum E, Khan KK, Cooper DL. 1997. Chlorambucil-induced
ports and MRI findings in four patients. J Neurooncol
Sasaki M, Ichiya Y, Kuwabara Y, et al. 1996. Hyperperfusion
Trillet V, Biron P. 1989. [Brain metastases: diagnostic and
and hypermetabolism in brain radiation necrosis with
therapeutic strategy]. Presse Med 18:1471–1475.
epileptic activity. J Nucl Med 37:1174–1176.
Vanhees SL, Raridaens K, Vansteenkiste JF. 2000. Syndrome of
Schliamser SE, Cars O, Norrby SR. 1991. Neurotoxicity of beta-
inappropriate antidiuretic hormone associated with chemo-
lactam antibiotics: predisposing factors and pathogenesis.
therapy-induced tumour lysis in small-cell lung cancer. Case
J Antimicrob Chemother 27:405–425.
report and literature review. Ann Oncol 11:1061–1065.
Schroeder H, Ostergaard JR. 1994. Interference of high-dose
Walton GD, Hon JK, Mulpur TG. 1997. Ofloxacin-induced sei-
methotrexate in the metabolism of valproate? Pediatr Hema-
zure. Ann Pharmacother 31:1475–1477.
Wang CH, Ng SH. 1995. Syncope as the initial presentation of
Shapiro MH, Ruiz-Ramon P, Fainman C, Ziegler MG. 1996.
nasopharyngeal carcinoma. J Neurooncol 25:73–75.
Light-headedness and defective cardiovascular reflexes af-
Wasserstrom WR, Glass JP, Posner JB. 1982. Diagnosis and
ter neck radiotherapy. Biol Press Monit 1:81–85.
treatment of leptomeningeal metastases from solid tumors:
Shehata N, Pater A, Tang SC. 1999. Prolonged severe 5-fluo-
experience with 90 patients. Cancer 49:759–772.
rouracil–associated neurotoxicity in a patient with dihydropy-
Weiss HD, Walker MD, Wiernik PH. 1974. Neurotoxicity of
rimidine dehydrogenase deficiency. Cancer Invest 17:201–205.
commonly used antineoplastic agents (first of two parts).
Silverman DA, Chapron DJ. 1995. Lymphopenic effect of car-
bamazepine in a patient with chronic lymphocytic leuke-
Weitzner MA, Meyers CA, Valentine AD. 1995. Methylphenidate
in the treatment of neurobehavioral slowing associated with
Smith DF, Hutton JL, Sandemann D, et al. 1991. The progno-
cancer and cancer treatment. J Neuropsychiatry Clin Neu-
sis of primary intracerebral tumours presenting with
epilepsy: the outcome of medical and surgical management.
Werner-Wasik M, Rudoler S, Preston PE, et al. 1999. Imme-
J Neurol Neurosurg Psychiatry 54:915–920.
diate side effects of radiotherapy and radiosurgery. Int J Ra-
Smith GA, Damon LE, Rugo HS Ries CA, Linker CA. 1997. High-
dose cytarabine dose modification reduces the incidence of
Wroblewski BA, Leary JM, Phelan AM, et al. 1992. Methyl-
neurotoxicity in patients with renal insufficiency. J Clin On-
phenidate and seizure frequency in brain injured patients
with seizure disorders. J Clin Psychiatry 53:86–89.
Snider S, Bashir R, Bierman P. 1994. Neurologic complica-
Zamboni WC, Gajjar AJ, Heideman RL, et al. 1998. Pheny-
tions after high-dose chemotherapy and autologous bone
toin alters disposition of topotecan and N-desmethyl
marrow transplantation for Hodgkin’s disease. Neurology
topotecan in a patient with medulloblastoma. Clin Can-
European Journal of Neurology 2008, 15 (Suppl. 1): 14–20Non-motor symptoms in ParkinsonÕs diseaseW. PoeweDepartment of Neurology, Medical University of Innsbruck, Innsbruck, AustriaAlthough still considered a paradigmatic movement disorder, ParkinsonÕs disease(PD) is associated with a broad spectrum of non-motor symptoms. These includedisorders of mood and affect with apathy, anhedonia a
Psiche e soma: oltre la concezione organicistica della malattia Introduzione I disturbi psicosomatici sono disfunzioni patologiche che si verificano a livello somatico e derivano soprattutto da processi psicologici. Per anni la medicina biologica, organicistica, ha trascurato il ruolo delle emozioni nella genesi delle patologie organiche. La valorizzazione dell'individuo come unit
 3601_e20_p438-453 2/19/02 8:59 AM Page 445
Seizures and Syncope in the Cancer Patient
tetany, transient encephalopathy, transient ischemic
mal lesions. The use of prophylactic antiepileptic
attacks, and panic attacks, which can all mimic
drugs in patients with brain tumors who do not have
seizures is controversial (Cohen et al., 1988). In suchpatients, antiepileptic drugs may cause adverse ef-fects. Whether or not to use antiepileptic drugs is de-
Treatment
3601_e20_p438-453 2/19/02 8:59 AM Page 445
Seizures and Syncope in the Cancer Patient
tetany, transient encephalopathy, transient ischemic
mal lesions. The use of prophylactic antiepileptic
attacks, and panic attacks, which can all mimic
drugs in patients with brain tumors who do not have
seizures is controversial (Cohen et al., 1988). In suchpatients, antiepileptic drugs may cause adverse ef-fects. Whether or not to use antiepileptic drugs is de-
Treatment