Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Uhc roundup: emerging products and services
24/7 Care Delivery Models Research Project UHC / RAND Collaboration Joanne Cuny RN, BSN, MBA Quality & Risk Councils Meeting Director of Quality February 19 – 20, 2009
2009 University HealthSystem Consortium
UHC/RAND Received AHRQ ACTION Grant to Examine 24x7 Care Delivery Models
AHRQ “Accelerating Change and Transformation in Organizations and
Networks (ACTION)" grant awarded to UHC and RAND Corp to support
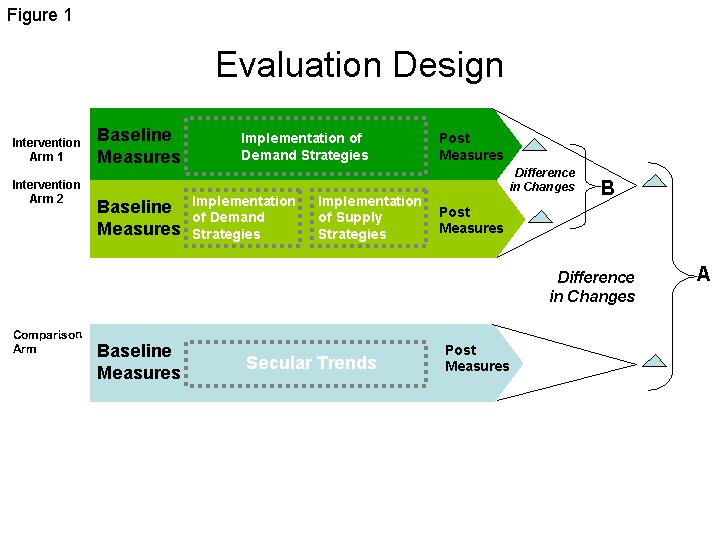
The study evaluated strategies designed to reduce workload demand on
medical and surgical service teams in academic medical centers; and
then reallocate staffing supply to match that demand around the clock. Key areas of inquiry included:
How does staffing supply and demand vary around the clock?
What interventions are effective in minimizing demand?
What workforce strategies best fit with optimal demand?
What are the consequences of care redesign on clinical quality?
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
A Quasi-experimental Study Model
Steering Committee consultation on scope and design Study site recruitment and group assignment
Demand and supply intervention design (best practice details)
Sites participate in implementation collaborative
Pre-implementation (baseline) data capture
Participation in improvement collaborative
- Gap analysis (current state vs best practices)
*Commit to ACTion
Data capture to measure compliance to plan
Analyze data and evaluate plan effectiveness
*UHC’s rapid cycle improvement collaborative
Maintain system change for duration of study
methodology
Analysis of performance measures data
Formative evaluation of implementation model
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Study Design
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Participating Organizations (# of pilot units) Study Arms: Intervention Arm 1: Demand only University of Maryland Medical Center (4) University of Florida-Shands HealthCare (2) University Hospitals Case Medical Center (1) Medical College of Georgia Health (3) Intervention Arm 2: Demand plus Supply West Virginia University Hospitals (3) University of Kentucky Hospital (1) Mount Sinai Medical Center (2) Stony Brook University Medical Center (2) Northwestern Memorial Hospital (1) New York-Presbyterian Hospital – Columbia (2) Comparison Arm 3 Emory Crawford Long (2) University of Iowa Hospitals & Clinics (2) UMass Memorial Medical Center (2) 15 UHC hospitals The Methodist Hospital (2) 30 pilot units Rush University Medical Center (1)
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Demand Intervention: Discharge Planning GOAL: Improve patient flow and throughput
Ensure integrated communication across disciplines
Review and discuss plan for care and discharge with patient
Confirm patient disposition and, if appropriate, complete discharge
Determine tasks to be accomplished and assign responsibility
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Demand Intervention: Structured Handoffs GOAL: Improve quality and safety of patient care
Standardize information to be included in every handoff
Protocol followed when patient moves and when staff changes
Mandated use of the handoff form for study
Ensure integrated process across disciplines, with handoff report
Handoffs to be scheduled at a regular time and place
Identify a location where interruptions and distractions are limited
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Demand Intervention: Managed Paging Process GOAL: Minimize service team distractions from patient care
Determine a signal to indicate level of urgency for response:
Assign responsibility to triage pages for urgency level to senior
Cluster delivery of non-emergent/urgent pages to scheduled
Consider eliminating pages for information only by
implementing message boards/clipboards/notebooks on units
or utilizing e-mail (must establish method to determine message received)
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Demand Intervention: Common Complaint PRN Order Sets GOAL: Eliminate interruptions in patient care to order medications to relieve symptoms that are common to hospitalized patients
Develop a common complaints order set to include as needed
Headache or mild pain (e.g. acetaminophen)
Mandate the use of the common complaints order set unless
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Supply Intervention: Matching Supply to Demand GOAL: Match supply to demand around-the-clock
Determine hourly workload demand (Staffing Planner)
Study the hours of activity demand related to admissions and
discharges for the pilot unit (Activity Curves)
Review staffing profile (available service team members)
Evaluate current care delivery team competencies relative to
Create a staffing schedule, moving human resources with
appropriate competencies to cover the observed demand
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Comparison Arm
Matched to geographic location and Case Mix Index (CMI)
Each site identified medical and/or surgical pilot units
Provided the same data elements collected from interventional sites from the time period identified as
Participated in Formative Evaluation telephone interviews
Without the interventions, changes noted in comparison site outcomes should indicate secular trends
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Research Questions A. Primary Research Questions:
Does implementing the redesign intervention improve EFFICIENCY
What are the consequences of implementing the system redesign strategies on CLINICAL QUALITY? B. Secondary Research Questions:
How does EFFICIENCY differ in demand-only intervention hospitals compared to demand & supply intervention hospitals?
How do the consequences on CLINICAL QUALITY differ in demand-only
intervention hospitals as compared to demand & supply intervention
How is the BUSINESS CASE different in the demand-only intervention hospitals as compared with demand & supply intervention hospitals?
How do the consequences on PROVIDER JOB SATISFACTION differ in the
demand-only intervention hospitals as compared to the demand and supply
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Hypotheses Related to Primary Research Questions System redesign by full implementation of study interventions will: EFFICIENCY outcomes
Move average discharge time to earlier in the day
CLINICAL QUALITY outcomes
Have no ill-effects on glycemic control or # of PSIs
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Questions? Please share your experiences with 24/7 care delivery models
Quality/Risk Council Meeting, February 2009
2009 University HealthSystem Consortium
Please visi for more inspiring lectures The Significance of Purim Purim is a Rabbinic holiday celebrated on the 14th of Adar to commemorate the survival of the Jewish people against the decree of Haman around 2500 years ago after the destruction of the first temple. It is important to keep in mind that at the time almost the entire Jewish population was under the rule of Achashverosh. This
Severe adverse reactions to Infliximab therapy are common in young children with inflammatory bowel disease K-L Kolho (kaija-leena.kolho@helsinki.fi)1, T Ruuska2, E Savilahti1 1.Hospital for Children and Adolescents, University of Helsinki, Box 281, FIN-00029 HYKS, Helsinki, Finland2.Department of Pediatrics, Tampere University Hospital, Box 2000, FIN-33014, Tampere, Finland Keywords Abstra
 Study Design
Study Design