Tadalafil zeigt eine ausgepr√§gte Proteinbindung von √ľber 90 %, was eine gleichm√§ssige Verteilung im Gewebe erm√∂glicht. Das Verteilungsvolumen betr√§gt rund 63 Liter, was auf eine deutliche extravaskul√§re Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau √ľber CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivit√§t mehr besitzen. Die Exkretion erfolgt √ľberwiegend f√§kal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverf√ľgbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen f√ľhren cialis generikum schweiz regelm√§ssig als Beispiel f√ľr PDE5-Hemmer mit verl√§ngerter Halbwertszeit auf.
Jvim_17_303.304_310.tp
J Vet Intern Med 2003;17:304‚Äď310
Diazepam as a Treatment for Metronidazole Toxicosis in Dogs: A Retrospective Study of 21 Cases
Jason Evans, Donald Levesque, Kim Knowles, Randy Longshore, and Scott Plummer
The currently recommended treatment for metronidazole toxicosis is drug discontinuation and supportive therapy. Reported recoverytimes are 1‚Äď2 weeks. The records of 21 dogs with metronidazole toxicosis were retrospectively analyzed to determine whetherdiazepam improved recovery. The dosage and duration of metronidazole therapy and the response and recovery times of 13 dogstreated with diazepam were compared to those of 8 dogs receiving only supportive care. Response time was defined as the timeto resolution of the debilitating clinical signs. Recovery time was the time to resolution of all residual clinical signs. The averagedosage and duration of metronidazole administration for the diazepam-treated and untreated groups were 60.3 mg/kg/d for 44.9days and 65.1 mg/kg/d for 37.25 days. The protocol for diazepam administration consisted of an initial IV bolus and then diazepamPO q8h for 3 days. The average dosage of both the IV and PO diazepam was 0.43 mg/kg. The average response time for thediazepam-treated dogs was 13.4 hours compared to 4.25 days for the untreated group. Recovery time also was markedly shorterfor the diazepam-treated dogs (38.8 hours) compared to the untreated group (11 days). Results of this study showed that dogs withmetronidazole toxicosis recover faster when treated with diazepam. Although the mechanism of metronidazole toxicosis or howdiazepam exerts its favorable effect is not known, it is likely related to modulation of the ‚ź•-aminobutyric acid (GABA) receptorwithin the cerebellar and vestibular systems. Key words: Benzodiazepine; Cerebellar disease; Drug toxicity; ‚ź•-Aminobutyric acid; Vestibular syndrome. Metronidazolea is a nitroimidazole antibacterial and an-
In humans, the centrally acting benzodiazepine diaze-
tiprotozoal compound1 used routinely in the treat-
pamb has long been used in the symptomatic treatment of
ment of giardiasis,2 anaerobic infections,3,4 and inflamma-
vertigo or disequilibrium secondary to diseases of the ves-
tory bowel disease.5 It has high bioavailability for most
tibular system such as benign paroxysmal vertigo (BPV)13,14
tissues, including bone and the central nervous system.
and endolymphatic hydrops (Meniere’s disease).15 Diaze-
Metronidazole is metabolized by the liver and has a half-
pam is believed to exert its antivertiginous effects by fa-
life of 3‚Äď13 hours in the dog.1 The adverse effects of met-
cilitating the effects of the inhibitory neurotransmitter
ronidazole in humans, which include seizures, ataxia, pe-
‚ź•-aminobutyric acid (GABA) within the vestibular sys-
ripheral neuropathy, and hematuria, are well document-
tem.16‚Äď21 Diazepam is principally used in veterinary medi-
ed.1,6,7 Adverse effects of metronidazole in the dog8,9 and
cine for its anticonvulsant, muscle-relaxant, sedative, an-
cat10,11 have been reported and include vomiting, hepato-
xiolytic, and appetite-stimulating properties.22,23 It has been
toxicity, neutropenia, and neurologic signs such as seizures,
suggested for use as a sedative in animals with severe dis-
head tilt, falling, paresis, ataxia, vertical nystagmus, trem-
equilibrium secondary to vestibular syndromes,24 but re-
ors, and rigidity.8‚Äď10 Neurologic adverse effects in cats have
ports suggesting its application as an antidote to a specific
a greater tendency to reflect forebrain dysfunction (disori-
entation and seizures) than brain stem dysfunction.10,11
At the Veterinary Neurological Center (VNC), dogs pre-
Neurologic toxicity from metronidazole has been report-
senting with signs of metronidazole toxicosis that were
ed in dogs receiving Ōĺ60 mg/kg/d for an average of 3‚Äď14
treated symptomatically with diazepam appeared to have a
days,8 but reports of toxicity at lower dosages have been
more rapid resolution of clinical signs than dogs in various
cited.10,11 The mechanism of the toxic effects of metroni-
published reports that had been treated with conservative
dazole has not been identified. The currently recommended
therapy alone. To evaluate potential differences in the re-
therapy for treating metronidazole toxicosis is discontinu-
covery time between dogs with metronidazole toxicosis
ation of the drug and supportive therapy. No specific treat-
treated with diazepam and a similar group that did not re-
ment to counteract the toxic effects of metronidazole has
ceive diazepam as part of the therapy, the following param-
been reported. Reported recovery times of dogs with neu-
eters were compared: dosage of metronidazole, duration of
rologic manifestations of metronidazole toxicosis are 1‚Äď2
therapy, time to resolution of the debilitating clinical signs
(response time), and time to final resolution of all residualclinical signs (recovery time).
Although the exact mechanism of metronidazole toxicity
From the Veterinary Neurological Center, Las Vegas, NV (Evans,Levesque); and the Veterinary Neurological Center, Phoenix, AZ
is not known, the neurologic adverse effects are indicative
(Knowles, Longshore, Plummer). The work was performed at both of
of cerebellar and central vestibular dysfunction. The neu-
the above addresses. A poster abstract was presented at the 2002
roinhibitory actions of benzodiazepines on the brain have
been shown to be mediated by GABA. Because GABA is
Reprint requests: Jason Evans, DVM, MS, Veterinary Neurological
the major inhibitory neurotransmitter of the cerebellar and
Center, 4445 N Rainbow Boulevard, Las Vegas, NV 89108; e-mail:
vestibular systems25‚Äď27 and because benzodiazepines such as
diazepam have their major effect on this neurotransmit-
Submitted July 12, 2002; Revised September 12, 2002; Accepted
ter,16‚Äď21 a possible relationship between metronidazole and
Copyright Š≠ß 2003 by the American College of Veterinary Internal
diazepam was postulated. Further speculation for metroni-
dazole’s affinity for the GABA receptor site was based on
the similarity of both the chemical structure and clinical
Summary statistics of dogs with metronidazole toxicosis in the treated and untreated groups.a
N/A, not applicable. a Mean Ōģ standard deviation. b The response and recovery times for the untreated group are listed in days, and the response and recovery times for the treated group are
signs of toxicity of metronidazole and the benzodiazepine
Statistical Analysis
antagonist flumazenil,c which also is known to attach to the
All statistical comparisons between the 2 groups were made by the
Student‚Äôs t-test. The level of significance was chosen as P ŌĹ .05. Correlation analysis was applied to the scatterplot (Fig 1) to measure
Materials and Methods
the correlation coefficient (r) of the relationship between dosage and
Criteria for Case Selection
duration of metronidazole administration and the onset of clinical signsof metronidazole toxicosis.
Medical records of 33 dogs at the VNC with a diagnosis of met-
ronidazole toxicosis between 1997 and 2001 were reviewed. Twenty-
one dogs were selected for this study on the basis of the availabilityof data regarding metronidazole dosage and duration of therapy before
The ages of the dogs in this study ranged from 10 months
the onset of clinical signs, response time, and recovery time. Thirteen
to 13 years, and the weight of the dogs ranged from 4.1 to
of the 21 dogs had been treated with diazepam, whereas the other 8
47.3 kg. Only 1 breed of dog (Shih Tzu) was represented
dogs had not received diazepam as part of their therapy. Response
more than once (twice) in this study.
time was defined as the time to resolution of debilitating clinical signs
The results of routine physical examinations did not iden-
and was determined by physical examination. For the purpose of thisstudy, debilitating clinical signs were those signs that resulted in the
tify any other major abnormality except for the neurologic
loss of vestibular function, motor function, or both to the degree that
signs. Nearly all of the neurologic problems were acute,
ambulation, eating, or drinking could not be performed. Debilitating
and the dogs were presented to a veterinarian within 24
clinical signs typically were related to the profound disequilibrium
hours of the onset of signs. Additionally, the final dose of
often associated with vestibular syndromes. Recovery time was de-
metronidazole had been given to all dogs within 24 hours
fined as the time to resolution of residual clinical signs of metroni-
of presentation to the VNC for examination. CBCs and se-
dazole toxicosis, which was the point at which the dog was considered
rum biochemistry were performed in 11 of 21 dogs, and
normal by either clinical examination or owner evaluation. Data con-
the most common abnormalities were mild-to-moderate in-
cerning breed, age, history, manifestations of metronidazole toxicosis,
creases in alkaline phosphatase activity and stress leuko-
and previous treatments were collected but not considered in the sta-
grams. Serum titers for Coccidioides immitis and Ehrlichiacanis had been performed on 7 and 8 dogs, respectively,
Treatment
and were negative. In addition, serum bile acid concentra-tions had been measured in 3 dogs, whereas computed tom-
The treatment for 13 patients with a tentative diagnosis of metro-
ographyd brain scans and cerebrospinal fluid analyses were
nidazole toxicosis at the VNC included an initial bolus of diazepam
performed on 2 dogs. All results were within normal limits.
administered IV and then PO q8h for 3 days. Metronidazole was dis-
The most common neurological signs were vertical nys-
continued in all animals, and supportive care including IV fluid ad-
tagmus (17 of 21), truncal ataxia (15 of 21), inability to
ministration was given to animals that were admitted to the hospital.
walk (10 of 21), upper motor neuron (UMN) paraparesis
Treatment for the group of dogs that did not receive diazepam after adiagnosis of metronidazole toxicosis primarily consisted of discontin-
(7 of 21), hypermetria (5 of 21), extensor rigidity of all 4
uation of the drug and supportive care. Summary information of the
limbs (5 of 21), UMN tetraparesis (5 of 21), intention trem-
dosages of both IV and PO diazepam administered is listed in Table 1.
ors (4 of 21), right head tilt (2 of 21), left head tilt (1 of21), right torticollis (2 of 21), and opisthotonos (2 of 21). Diagnosis of Metronidazole Toxicosis
Of the 10 dogs that were nonambulatory, 5 were unable towalk without assistance because of cerebellovestibular dys-
Blood concentrations of metronidazole were not measured, but all
function, but these dogs were not tetraparetic.
dogs in this study were diagnosed with metronidazole toxicosis on thebasis of a history of having received metronidazole, clinical signs
The most common reasons for administration of metro-
compatible with metronidazole toxicosis, absence of other clinical dis-
nidazole were for treatment of gastrointestinal signs such
ease, and eventual recovery of all dogs upon discontinuation of met-
as diarrhea (7 of 21) or vomiting (4 of 21), for suspected
inflammatory bowel disease (5 of 21), for high liver en-
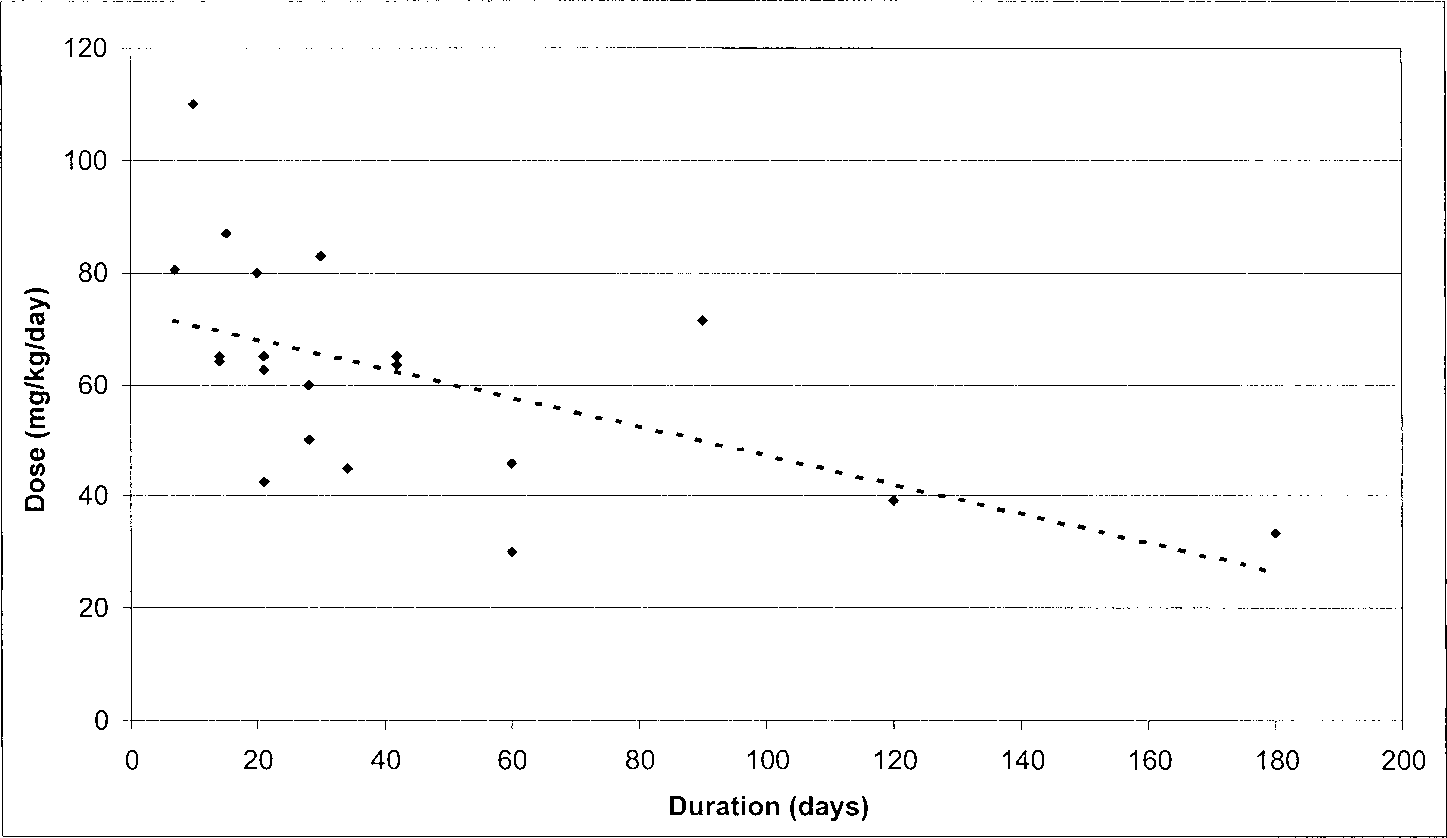
A scatterplot analysis of the doses and durations of metronidazole therapy for the dogs in this investigation. Higher dosages generally
require shorter duration of administration to produce clinical signs of metronidazole toxicosis (r Ō≠ Ō™.56). The data from dog 13 of the treatedgroup were omitted from this chart because the dog had been on metronidazole therapy for 1,099 days, which was, individually, markedly differentfrom the other dogs in this study.
zyme activities (2 of 21), for giardiasis (2 of 21), and for
diazepam was 0.2‚Äď0.625 and 0.31‚Äď0.69 mg/kg, respective-
dental disease (1 of 21). Before the diagnosis of metroni-
dazole toxicosis, medical treatments for the neurologic
Dogs treated with diazepam had an average response
signs consisted of one or more of the following: corticoste-
time of 13 hours and an average recovery time of 38.7
roids (16 of 21), antibiotics (8 of 21), methocarbamole (5
hours. The response times for dogs treated with diazepam
of 21), carprofenf (3 of 21), meclizineg (2 of 21), and bu-
ranged from 20 minutes to 24 hours, and the recovery times
ranged from 24 to 72 hours. Dogs that were not treated
Table 1 lists the summary statistics of dosages and du-
with diazepam had an average response time of 4.25 days
ration of metronidazole administration, dosages of IV and
and an average recovery time of 11.6 days. Response times
PO diazepam, if applicable, and response and recovery
for the dogs in the untreated group ranged from 2 to 10
times for dogs in the untreated and treated groups.
days, and recovery times ranged from 5 to 21 days. Both
The average daily dosage of metronidazole for dogs that
the response and recovery times for the animals treated with
received diazepam was 60.3 mg/kg/d; for dogs that were
diazepam were significantly shorter than those for the un-
not treated with diazepam, the average daily dosage of met-
ronidazole was 65.1 mg/kg/d. The range of the individualdosages of metronidazole for dogs that were given diaze-
Discussion
pam was 33‚Äď83 mg/kg/d. The range of the metronidazoledosages for dogs in the untreated group was 45‚Äď110 mg/
The neurologic adverse effects of metronidazole are well
kg/d. The average daily dosage of metronidazole was not
documented in humans1,7 and companion animals.8‚Äď11 There
significantly different between the 2 groups (P Ōĺ .05).
is currently no recommended treatment other than with-
The average duration of metronidazole administration for
drawing the drug and providing supportive care. Diazepam,
dogs treated with diazepam was 127 days, with a range of
a centrally acting benzodiazepine, is used in human medi-
7‚Äď1,099 days. The average duration of metronidazole ad-
cine for symptomatic treatment of signs of vestibular sys-
ministration was 37 days for animals in the untreated group,
tem dysfunction,13‚Äď15,28,29 but reports have not indicated any
with a range of 10‚Äď120 days. If the data from dog 13 of
curative effect for an underlying disease or toxicity. In one
the diazepam-treated group that had been on metronidazole
study, guinea pigs undergoing unilateral labyrinthectomy
therapy for 1,099 days are disregarded, the average duration
and treated with diazepam had milder signs than the un-
of metronidazole use for the diazepam-treated group be-
treated group, but there was no marked difference between
comes 44 days. The resulting calculation is closer to the
the groups in the time to complete vestibular compensa-
37-day average of the untreated group; however, including
tion.28 Similar findings regarding vestibular compensation
the data from this dog does not alter the statistical analysis
are reported in humans with BPV treated with diazepam.14,29
in comparing the 2 groups. The duration of metronidazole
Diazepam has been recommended for alleviating signs of
administration was not significantly different between the 2
vestibular dysfunction in humans and animals, but indica-
tions for the use of diazepam other than for palliative ther-
The average single, initial IV dosage of diazepam was
0.43 mg/kg, and the average subsequent PO dosage was
The results of this investigation demonstrate that diaze-
0.43 mg/kg. The range for IV and PO administration of
pam dramatically improves recovery times for dogs with
metronidazole toxicosis. Recovery times for dogs in thisstudy that did not receive diazepam were consistent withprevious reports. Dogs 1 and 3 in the untreated group hadprolonged recovery times, which greatly increased the av-erage overall recovery time for animals in this group. Bothof these dogs suffered pronounced paraparesis, which lin-gered long past the resolution of the acute vestibular signs. Although these 2 dogs may have adversely influenced theaverage overall time to clinical resolution for the untreatedgroup, there still was a marked difference in the responseand recovery times compared to the diazepam-treated ani-mals if data from these 2 dogs are discarded.
The results of this investigation show a positive corre-
lation between dosage and duration of treatment relative tothe time of onset of signs of metronidazole toxicosis (Fig
Diagrammatic representation of a ‚ź•-aminobutyric acid
1). There did not appear to be an increased susceptibility
(GABA) receptor. The GABA receptor is a multisubunit ligand-gatedchloride (ClŌ™) ion channel composed of
to adverse effects of metronidazole administration on the
increase in chloride conductance from the release of GABA from the
basis of either age or breed. The average dosage of met-
presynaptic membrane results in the inhibitory modulation of neural
ronidazole that induced toxicity in the dogs of this study
activity through membrane hyperpolarization.
(60.3 and 65.1 mg/kg/d for diazepam-treated and untreatedgroups, respectively) was consistent with published reports.
Ours was a retrospective study, and a specific protocol
for the administration of diazepam was not used. All ani-
facilitates inhibitory transmission in the cerebral cortex and
mals in the diazepam-treated group, however, received an
between the substantia nigra and caudate nucleus.27,34
initial, single IV bolus and then diazepam PO q8h for 3
Because of the prevalence of GABA-minergic receptors
days. The average dosage of both the IV and PO diazepam
in those tracts damaged by metronidazole and the knownrelationship of GABA receptors and benzodiazepines, the
was 0.43 mg/kg, but there was no apparent correlation be-
following mechanism may be postulated: benzodiazepines,
tween the dosages of either the IV or PO routes and the
such as diazepam, potentiate GABA influence on chloride
conductance, thereby enhancing an inhibitory effect on ex-
Neither the mechanism of metronidazole toxicity nor the
citatory neurons.38‚Äď40 Conversely, inhibition of GABA re-
precise mechanism of action of diazepam in the reversal of
lease, such as seen in the neurological adverse effects of
signs is known. Because the neurological effects of met-
enrofloxacin,i ciprofloxacin,j and imipenem,k can lead to hy-
ronidazole are referable to both cerebellar and central ves-
perexcitability of the central nervous system, resulting in
tibular dysfunction, literature regarding the histology and
seizures or tremors.41,42 It may therefore be speculated that
physiology of these systems was reviewed for a relationship
interference of the GABA receptor at the postsynaptic
membrane also may result in central nervous system hy-
Histological examinations of brain tissue in dogs with
metronidazole toxicosis have demonstrated Purkinje cell
The benzodiazepines have specific binding sites on
loss8,30 and axonal degeneration in vestibular tracts.8 His-
GABA receptors within the brain, particularly in the cere-
topathologic studies in mice given toxic dosages of met-
bellum, cerebral cortex, and limbic system.41,43 The imida-
ronidazole showed cerebellar Purkinje cell loss and degen-
zobenzodiazepine flumazenil is a selective, competitive an-
erative changes in the vestibular, cochlear, deep cerebellar,
tagonist (also known as an inverse agonist) of the benzo-
and olivary nuclei as well as in the rostral colliculi.31 These
diazepine receptor.40,41,44‚Äď47 Both flumazenil and metronida-
nuclei and their associated tracts are involved primarily
zole have an imidazole component, and it is possible that
with equilibrium, hearing, and fine motor control.32,33 These
metronidazole also may bind specifically to benzodiazepine
nuclei, particularly the Purkinje cells, mediate an inhibitory
sites on GABA receptors in the cerebellar and central ves-
influence on postsynaptic receptors,34,35 and their principal
tibular systems, resulting in loss of inhibition, similar in
neurotransmitter is GABA,25,26,34 which is the major inhib-
effect to flumazenil (Fig 3). That the adverse reactions of
itory neurotransmitter of the central nervous system.25‚Äď27,36
flumazenil in humans, such as seizures, vertigo, and atax-
Activation of the GABA receptor by GABA or GABA mi-
ia,45‚Äď47 are similar to the neurological adverse effects of
metics, such as benzodiazepines, increases chloride (ClŌ™)
metronidazole in dogs lends additional credence to this pro-
conductance at the postsynaptic membrane, resulting in hy-
posed mechanism of metronidazole toxicity. Regardless of
perpolarization (Fig 2).37 The majority of GABA-minergic
whether metronidazole specifically binds to the benzodi-
receptors in the central nervous system are located between
azepine receptor inhibiting the effects of GABA or selec-
the neurons of the cerebellum and their associated brain-
tively destroys these cells by another mechanism, it is the
stem nuclei, especially the Purkinje cells and the lateral
GABA-dependent interactions of the cerebellar and central
vestibular nuclei. Other major sites of GABA receptors are
vestibular systems that are affected. It can be therefore pos-
in the tracts between the vestibular nuclei and the trochlear
tulated that diazepam either competes with metronidazole
motor neurons and within the olfactory bulbs, cuneate nu-
for the benzodiazepine receptor site or supplements GABA
clei, hippocampus, and lateral septal nuclei.27 GABA also
propagation via unaffected receptors, whereas the remain-
Diagrammatic representation of the proposed mechanism of
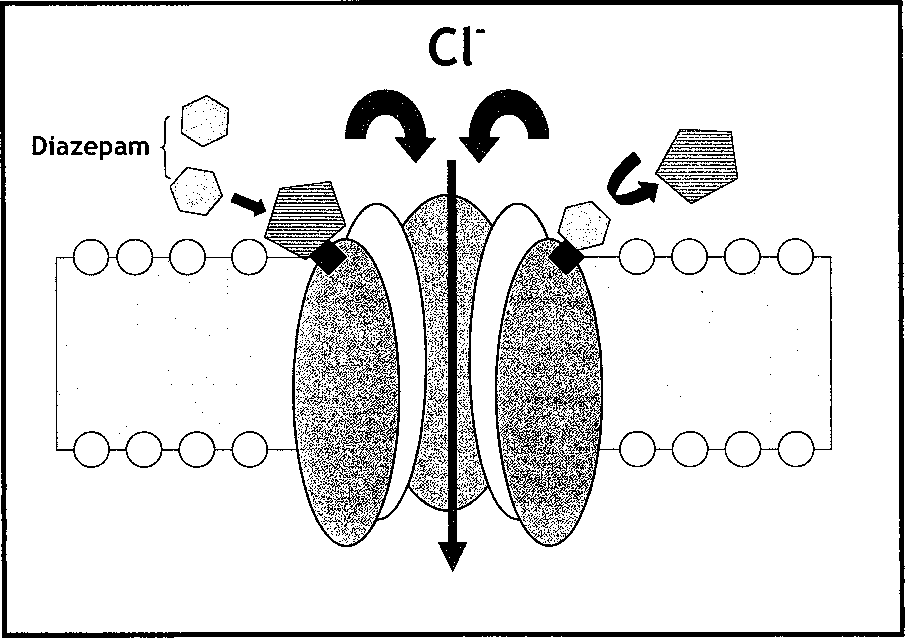
Diagram of the proposed mechanism for the therapeutic effect
metronidazole toxicity. Metronidazole binds to the ‚ź•-aminobutyric
of diazepam in metronidazole toxicosis. Metronidazole produces its
acid (GABA) receptor on the postsynaptic membrane and disrupts the
toxic effects by binding to the benzodiazepine site on the ‚ź•-amino-
inhibitory influence of GABA. Benzodiazepine antagonists, such as
butyric acid (GABA) receptor on the postsynaptic membrane, dis-
flumazenil, bind to the benzodiazepine site, competitively inhibiting
rupting inhibitory neurotransmission. We postulate that diazepam has
the actions of benzodiazepines. Metronidazole and flumazenil share
a higher affinity for the benzodiazepine site than metronidazole and
both similar chemical structure and toxic adverse effects such as ataxia
therefore displaces metronidazole. Removal of metronidazole not only
restores normal chloride conductance but also increases benzodiaze-pine-induced chloride conductance (inhibition).
der of the metronidazole in the system is metabolized. It ismore likely that diazepam at therapeutic concentrations
existent. The 2 dogs that had received the H -antagonist
competitively reverses the binding of metronidazole to the
meclizine, which generally is used to treat signs of motion
benzodiazepine site on the GABA receptor, because re-
sickness in humans,48 and the 2 dogs that underwent general
bound manifestations of metronidazole toxicosis were not
anesthesia all were in the untreated group. Four dogs from
observed in the dogs of this study (Fig 4).
each group had been given either an aminopenicillin or a
The average response time for the resolution of debili-
1st-generation cephalosporin; methocarbamol had been giv-
tating clinical signs in animals receiving diazepam in this
en to 3 dogs of the treated group and 2 dogs of the untreated
study was 13 hours, with a final resolution of the remaining
group; and butorphanol had been administered to 1 dog
clinical signs (usually mild ataxia) over the next 24‚Äď48
from each group. Neurological adverse effects such as sei-
hours. The plasma half-life of metronidazole in the dog is
zures, sedation, and ataxia have been described for each of
3‚Äď13 hours1; given this fact, the question of why the clinical
these medications, but these adverse effects have been re-
signs of metronidazole toxicosis are not resolved in this
ported rarely and only with prolonged use or very high
time simply after discontinuation of the drug also is raised.
dosages.42,49‚Äď51 Corticosteroids, which had been adminis-
It is possible that metronidazole at toxic doses either alters
tered to 6 of 8 dogs in the untreated group and to 10 of 13
the GABA receptor sufficiently to prevent a return to nor-
dogs in the diazepam-treated group, could theoretically
mal function within the anticipated time or firmly binds to
have induced the oxidative metabolism of metronidazole,52
the receptor and therefore is not subject to normal metab-
but the effect of corticosteroids was not believed to be im-
olism. From the similarities in the plasma half-life of met-
portant because their use was common in both groups, and
ronidazole and the average response time of the diazepam-
only 1‚Äď2 doses had been given. All dogs in this study had
treated group, it could be speculated that once metronida-
neurological manifestations consistent with metronidazole
zole is displaced from the benzodiazepine receptor by di-
toxicosis before administration of any of these drugs and
azepam, normal metabolism of the displaced drug then
were diagnosed with metronidazole toxicosis within 24
occurs, resulting in the rapid clinical improvement ob-
hours of the onset of the neurological signs. Administration
served. Furthermore, once metronidazole is displaced, the
of the above ancillary medications was discontinued after
exogenous benzodiazepine not only restores but also en-
the diagnosis was established, making it unlikely any med-
hances normal benzodiazepine-induced chloride conduc-
ication other than diazepam influenced the outcome of these
tance. Blood metronidazole concentrations were not mea-
sured in the dogs of this study but may have been useful
A dose-dependent or duration-dependent relationship be-
as an ancillary test to further confirm the diagnosis of met-
tween actual neuronal cell death or leukomalacia of the
ronidazole toxicosis; additionally, serial posttreatment con-
vestibulocerebellar tracts and metronidazole administration
centrations could give additional insight into the metabolic
could not be determined from this study because no histo-
fate of metronidazole after administration of diazepam.
pathologic evaluations were performed. Clinical and exper-
Nineteen of the 21 dogs of this investigation received 1
imental studies reported neuronal changes in subjects re-
or more medications as treatment for the acute onset of
ceiving much higher dosages than the 60.3-mg/kg/d dosage
neurological signs before definitive diagnosis of metroni-
received by dogs in this investigation.8,30,31 Vestibulocere-
dazole toxicosis, but the influence of these medications on
bellar axonal degeneration with no loss of neurons, how-
the results of this study was thought to be minimal to non-
ever, has been reported in dogs receiving 63 mg/kg/d.8 Al-
though the animals in this investigation recovered, the po-
12. Dow SW. Management of anaerobic infections. Vet Clin North
tential for permanent, subclinical damage to neurons and
white matter tracts in all cases of metronidazole toxicosis
13. McClure JA, Lycett P, Baskerville JC. Diazepam as an anti-
exists, thereby increasing the probability that these animals
motion sickness drug. J Otolaryngol 1982;4:253‚Äď259.
will be more susceptible to the adverse effects of metro-
14. McClure JA, Willett JM. Lorazepam and diazepam in the treat-
ment of benign paroxysmal vertigo. J Otolaryngol 1980;6:472‚Äď477.
nidazole in the future. Administration of metronidazole to
15. Uchide K, Suzuki N, Takiguchi T, et al. The possible effect of
animals previously diagnosed with metronidazole toxicosis
pregnancy on Meniere’s disease. J Otorhinolaryngol Relat Spec 1997;
Although the exact mechanism is not known, the use of
16. Matsuoka I, Chikamori Y, Takaori S, Morimoto M. Effects of
diazepam markedly improved the recovery of animals with
chlorpromazine and diazepam on neuronal activities of the lateral ves-
metronidazole toxicosis. Consequently, we recommend the
tibular nucleus in cats. Arch Otorhinolaryngol 1975;209:89‚Äď95.
use of diazepam for the treatment of metronidazole toxi-
17. Pettorossi VE, Troiani D, Petrosini L. Diazepam enhances cer-
ebellar inhibition on vestibular neurons. Acta Otolaryngol 1982;93:363‚Äď373.
18. Matsuoka I, Takahashi H, Sasa M, Takaori S. Experimental ves-
tibular pharmacology: A minireview with special reference to neuro-
Footnotes
active substances and antivertigo drugs. Acta Otolaryngol 1984;419(Suppl):62‚Äď70.
a Metronidazole, FlagylŗĮ°, GD Searle & Co, Chicago, IL
19. Barmack NH, Pettorossi VE. The influence of diazepam on the
b Diazepam, ValiumŗĮ°, Roche, Division of SmithKline Beecham, Ex-
activity of secondary vestibular neurons in the rabbit. Neurosci Lett
c Flumazenil, RomazinconŗĮ°, Roche, Division of SmithKline Beecham,
20. Ryu JH, McCabe BF. Effects of diazepam and dimenhydrinate
on the resting activity of the vestibular neuron. Aerospace Med 1974;
d Model 9800 GE HiLite AdvantageŗĮ° CT Scanner, GE Medical Sys-
21. Steiner FA, Felix D. Antagonistic effects of GABA and ben-
e Methocarbamol, RobaxinŗĮ°, Fort Dodge Animal Health, Fort
zodiazepines on vestibular and cerebellar neurons. Nature 1976;260:
f Carprofen, RimadylŗĮ°, Pfizer Animal Health Inc, New York, NY
22. Overall KL. Fears and phobias‚ÄĒDogs. In: Tiley LP, Smith
g Meclizine, AntivertŗĮ°, Solvay Animal Health Inc, Mendota
FWK, ed. The Five-Minute Veterinary Consult. Baltimore, MD: Wil-
h Butorphanol, TorbugesicŗĮ°, Fort Dodge Animal Health, Fort Dodge, IA
23. Polzin DJ, Osborne CA. Diseases of the urinary tract. In: Davis
i Enrofloxacin, BaytrilŗĮ°, Miles Inc, Shawnee, KS
LE, ed. Handbook of Small Animal Therapeutics. New York, NY:
j Ciprofloxacin, CiproŗĮ°, Miles Inc, Shawnee, KS
Churchill Livingstone; 1985:333‚Äď395.
k Imipenem-Cilastatin, PrimaxinŗĮ°, Merck & Co, West Point, PA
24. Cochrane SM. Geriatric vestibular disease. In: Tiley LP, Smith
FWK, ed. The Five-Minute Veterinary Consult. Baltimore, MD: Wil-liams & Wilkins; 1997:1150‚Äď1151. References
25. MacDonald RL, McLean MJ. Cellular basis of barbiturate and
phenytoin anticonvulsant drug action. Epilepsia 1982;23:s7‚Äďs18.
1. Finegold SM. Metronidazole. Ann Intern Med 1980;93:585‚Äď587.
26. Bonanno G, Raiteri M. Multiple GABA receptors. Trends Phar-
2. Johnson G. Giardiasis. In: Kirk RW, ed. Current Veterinary Ther-
apy VI. Philadelphia, PA: WB Saunders; 1977:969.
27. Bloom F. Neurotransmission and the central nervous system. In:
3. Garvey MS, Aucoin DP. Therapeutic strategies involving anti-
Hardman JG, Limbird LE, ed. Pharmacological Basis for Therapeutics,
microbial treatment of disseminated bacterial infection in small ani-
9th ed. New York, NY: McGraw Hill; 1996:267‚Äď293.
mals. J Am Vet Med Assoc 1984;185:1185‚Äď1189.
28. Martin J, Gilchrist DP, Smith PF, Darlington CL. Early diaze-
4. Dow SW, Jones RL, Adney WA. Anaerobic infections in dogs
pam treatment following unilateral labyrinthectomy does not impair
and cats and response to treatment: 36 cases (1985‚Äď1986). J Am Vet
vestibular compensation of spontaneous nystagmus in guinea pig. J
5. Tams TR. Feline inflammatory bowel disease. In: Kirk RW, ed.
Current Veterinary Therapy IX. Philadelphia, PA: WB Saunders; 1986:
29. Ishikawa K, Igarashi M. Effect of diazepam on vestibular com-
pensation in squirrel monkeys. Arch Otorhinolaryngol 1984;240:49‚Äď
6. Rosenblatt JE, Edson RS. Metronidazole. Mayo Clin Proc 1983;
30. Scharer K. Selective Purkinje-Zellschadigungen nach oraler
7. Kusumi RK, Plouffe JF, Wyatt RH, et al. Central nervous system
Verabreichung grosser Dosen von Nitroimidazol-Derivaten am Hund.
toxicity associated with metronidazole therapy. Ann Intern Med 1980;
Verh Dtsch Ges Pathol 1972;56:407‚Äď410.
31. Rogulja PV, Kovac W, Schmid H. Metronidazol-Encephalopa-
8. Dow SW, LeCouter RA, Poss ML, Beadleston D. Central ner-
thie der Ratt. Acta Neuropathol (Berl) 1973;25:36‚Äď45.
vous system toxicosis associated with metronidazole treatment of
32. Jenkins TW. Functional Mammalian Neuroanatomy, 2nd ed.
dogs: Five cases (1984‚Äď1987). J Am Vet Med Assoc 1989;195:365‚Äď
Philadelphia, PA: Lea & Febiger; 1978:238‚Äď251.
33. DeLahunta A. Veterinary Neuroanatomy and Clinical Neurol-
9. Fitch R, Moore M, Roen D. A warning to clinicians: Metroni-
ogy, 2nd ed. Philadelphia, PA: WB Saunders; 1983:255‚Äď278.
dazole neurotoxicity in a dog. Prog Vet Neurol 1991;2:307‚Äď309.
34. Chan-Palay V, Palay SL, Wu JY. Gamma amino butyric acid
10. Saxon B, Magne M. Reversible central nervous system toxi-
pathways in the cerebellum studied by retrograde and anterograde
cosis associated with metronidazole therapy in three cats. Prog Vet
transport of glutamic decarboxylase antibody after in vivo injections.
11. Caylor KB, Cassimatis MK. Metronidazole neurotoxicosis in
35. Henneman E. The cerebellum. In: Mountcastle VB, ed. Medical
two cats. J Am Anim Hosp Assoc 2001;37:258‚Äď262.
Physiology, 13th ed. St Louis, MO: CV Mosby; 1974:633‚Äď655.
36. Bowery NG. GABA receptor pharmacology. Annu Rev Phar-
44. Haefely W. Antagonists of benzodiazepines: Functional aspects.
Adv Biochem Psychopharmacol 1983;38:73‚Äď93.
37. Otsuka M. Gamma amino butyric acid and some other trans-
45. Roncari G, Timm U, Zell M, et al. Flumazenil kinetics in the
mitter candidates in the nervous system. In: Acheson GH, Bloom FE,
elderly. Eur J Clin Pharmacol 1993;45:585‚Äď587.
ed. Pharmacology and the Future of Man. Proceedings of the Fifth
46. Brogden RN, Goa KL. Flumazenil: A preliminary review of its
International Congress on Pharmacology, San Francisco, CA, 1973;4:
benzodiazepine antagonist properties, intrinsic activity and therapeutic
38. Schofield PR, Darlison MG, Fujita N, et al. Sequence and func-
47. Hoffman EJ, Warren EW. Flumazenil: A benzodiazepine antag-
tional expression of the GABA receptor shows a ligand-gated receptor
onist. Clin Pharmacol 1993;12:814‚Äď828.
superfamily. Nature 1987;328:221‚Äď227.
48. Cohen B, DeJong JMBV. Meclizine and placebo in treating ver-
tigo of vestibular origin. Relative efficacy in a double-blinded study.
39. Pritchett DB, Sonthiemer H, Shivers BD, et al. Importance of
a novel GABAa receptor subunit for benzodiazepine pharmacology.
49. Mandell GL, Petri WA. Penicillins, cephalosporins and other
beta-lactam antibiotics. In: Hardman JG, Limbird LE, ed. Pharmaco-
40. Burt DR, Kamatchi GL. GABA receptor subtypes: From phar-
logical Basis for Therapeutics, 9th ed. New York, NY: McGraw Hill;
macology to molecular biology. FASEB J 1991;5:2916‚Äď2923.
41. Gardner CR. Functional in vivo correlates of the benzodiaze-
50. Fingeroth JM. Treatment of canine intervertebral disk disease:
pine agonist-inverse agonist continuum. Prog Neurobiol 1988;31:425‚Äď
Recommendations and controversies. In: Kirk RW, ed. Current Vet-
erinary Therapy XII. Philadelphia, PA: WB Saunders; 1995:1148.
42. Semel JD, Allen N. Seizures in patients simultaneously receiv-
51. Jenkins WL. Pharmacological aspects of analgesic drugs in an-
ing theophylline and imipenem or ciprofloxacin or metronidazole.
imals: An overview. J Am Vet Med Assoc 1987;191:1231‚Äď1240.
52. Lau AH, Lam NP, Piscitelli SC, et al. Clinical pharmacokinetics
43. Potokar J, Nutt DJ. Anxiolytic potential of benzodiazepines re-
of metronidazole and other nitroimidazole anti-infectives. Clin Phar-
ceptor partial agonists. CNS Drugs 1994;1:305‚Äď315.
Nei giorni avvenire Giacobbe metter√† radici, e tutto il mondo sar√† pieno del suo prodotto. Raccolti da David Pacifici per il sito www.torah.it e pubblicati in occasione di Yom Haazmaut 2010, 62¬į anniversario dell‚Äôindipendenza del moderno Lo sapevi? Il 2 aprile 2010 l'indice di borsa di Tel Aviv ha superato la quotazione record di tutti i tempi. I motivi in due righe? Nessuna ba
 A scatterplot analysis of the doses and durations of metronidazole therapy for the dogs in this investigation. Higher dosages generally
require shorter duration of administration to produce clinical signs of metronidazole toxicosis (r Ō≠ Ō™.56). The data from dog 13 of the treatedgroup were omitted from this chart because the dog had been on metronidazole therapy for 1,099 days, which was, individually, markedly differentfrom the other dogs in this study.
A scatterplot analysis of the doses and durations of metronidazole therapy for the dogs in this investigation. Higher dosages generally
require shorter duration of administration to produce clinical signs of metronidazole toxicosis (r Ō≠ Ō™.56). The data from dog 13 of the treatedgroup were omitted from this chart because the dog had been on metronidazole therapy for 1,099 days, which was, individually, markedly differentfrom the other dogs in this study.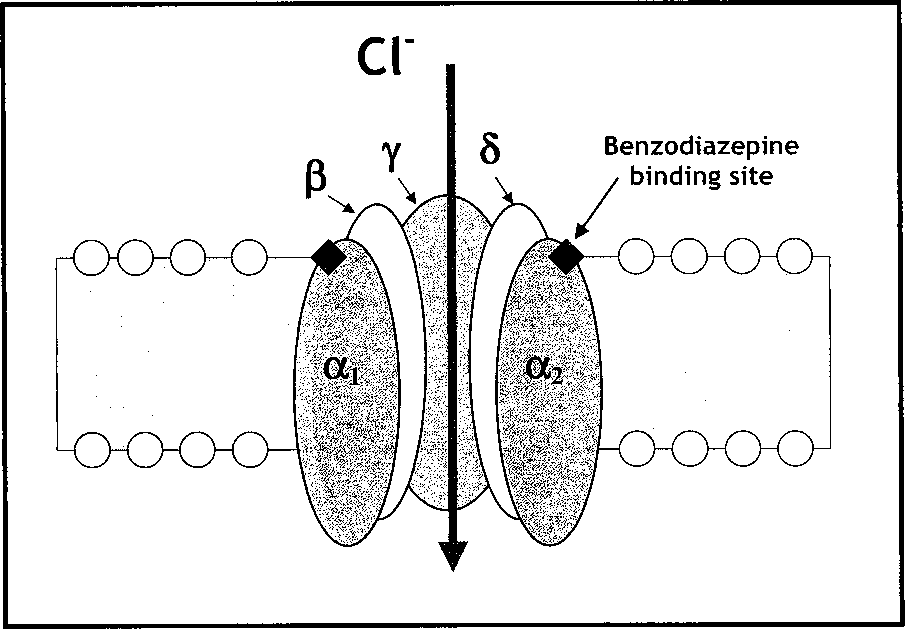 metronidazole toxicosis. Recovery times for dogs in thisstudy that did not receive diazepam were consistent withprevious reports. Dogs 1 and 3 in the untreated group hadprolonged recovery times, which greatly increased the av-erage overall recovery time for animals in this group. Bothof these dogs suffered pronounced paraparesis, which lin-gered long past the resolution of the acute vestibular signs.
metronidazole toxicosis. Recovery times for dogs in thisstudy that did not receive diazepam were consistent withprevious reports. Dogs 1 and 3 in the untreated group hadprolonged recovery times, which greatly increased the av-erage overall recovery time for animals in this group. Bothof these dogs suffered pronounced paraparesis, which lin-gered long past the resolution of the acute vestibular signs.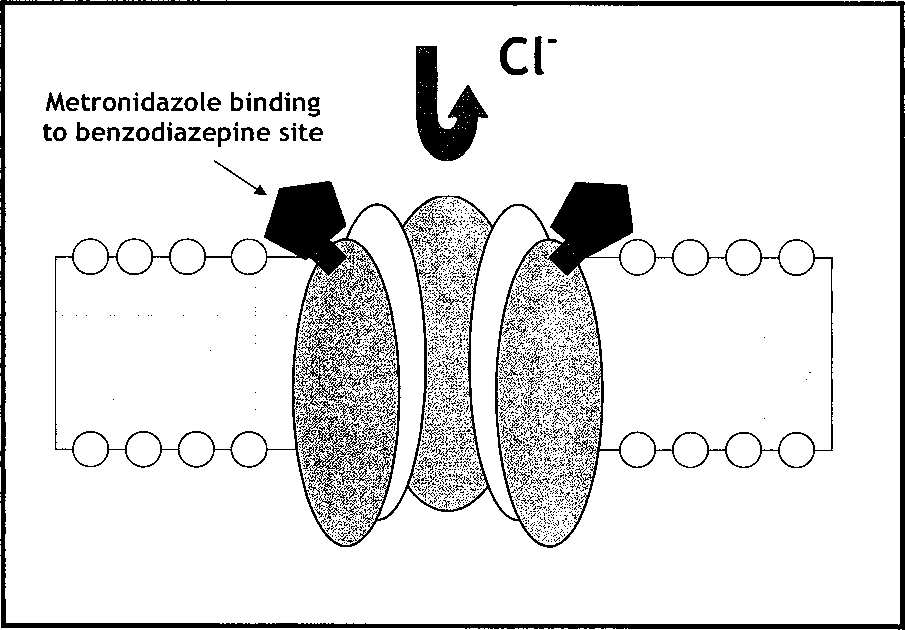
 Diagrammatic representation of the proposed mechanism of
Diagram of the proposed mechanism for the therapeutic effect
metronidazole toxicity. Metronidazole binds to the ‚ź•-aminobutyric
of diazepam in metronidazole toxicosis. Metronidazole produces its
acid (GABA) receptor on the postsynaptic membrane and disrupts the
toxic effects by binding to the benzodiazepine site on the ‚ź•-amino-
inhibitory influence of GABA. Benzodiazepine antagonists, such as
butyric acid (GABA) receptor on the postsynaptic membrane, dis-
flumazenil, bind to the benzodiazepine site, competitively inhibiting
rupting inhibitory neurotransmission. We postulate that diazepam has
the actions of benzodiazepines. Metronidazole and flumazenil share
a higher affinity for the benzodiazepine site than metronidazole and
both similar chemical structure and toxic adverse effects such as ataxia
therefore displaces metronidazole. Removal of metronidazole not only
restores normal chloride conductance but also increases benzodiaze-pine-induced chloride conductance (inhibition).
Diagrammatic representation of the proposed mechanism of
Diagram of the proposed mechanism for the therapeutic effect
metronidazole toxicity. Metronidazole binds to the ‚ź•-aminobutyric
of diazepam in metronidazole toxicosis. Metronidazole produces its
acid (GABA) receptor on the postsynaptic membrane and disrupts the
toxic effects by binding to the benzodiazepine site on the ‚ź•-amino-
inhibitory influence of GABA. Benzodiazepine antagonists, such as
butyric acid (GABA) receptor on the postsynaptic membrane, dis-
flumazenil, bind to the benzodiazepine site, competitively inhibiting
rupting inhibitory neurotransmission. We postulate that diazepam has
the actions of benzodiazepines. Metronidazole and flumazenil share
a higher affinity for the benzodiazepine site than metronidazole and
both similar chemical structure and toxic adverse effects such as ataxia
therefore displaces metronidazole. Removal of metronidazole not only
restores normal chloride conductance but also increases benzodiaze-pine-induced chloride conductance (inhibition).