Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Webguild.com
Public Dollars for Private Profit Taxmoxifen as a case study for how drugs developed at taxpayer-expenseare sold to Americans at inflated prices to fuel corporate earnings
Compiled by the Office of Rep. Bernard Sanders
The NIH and Drug Industry Profits: An Overview
Right now, the federal government gives away billions of dollars worth of taxpayer-financed intellectualproperty to huge, profitable pharmaceutical companies.
The National Institutes of Health are the jewel of American science, producing lifesaving drugs of enormousvalue to our nation and the world. From 1955 to 1992, for example, 92% of drugs approved by the FDA to treatcancer were researched and developed by NIH. However, much of the financial value of these drugs is givenaway to pharmaceutical corporations in an outrageous example of corporate welfare.
Currently, once NIH has successfully developed a new drug it signs over monopoly commercial rights to largepharmaceutical companies which then can – and do - charge American consumers as much as they want. In thearea of breast cancer, this corporate giveaway is particularly egregious. After the NIH used millions of taxpayerdollars to conduct more than 140 clinical trials of the critical drug Tamoxifen, the drug is now sold to Americanconsumers at almost 10 times the price as sold in other nations.
It is absurd that Americans must pay twice for lifesaving drugs, first as taxpayers to develop the drug and thenas consumers to pad pharmaceutical profits. These costs fall hardest on those least able to bear the burden, suchas cancer patients, AIDS patients and senior citizens, nearly half of whom must pay the full cost of prescriptiondrugs out of pocket. This is particularly outrageous because, unlike the Americans who must bankruptthemselves to get lifesaving medicines, the pharmaceutical industry is extremely healthy and hardly in need oftaxpayer support. From 1988 through 1995, pharmaceuticals surpassed all other Fortune 500 industries in profitrates, and they have ranked in the top two for 31 of the past 39 years.
In the case of AstraZeneca, the monopoly owner of Nolvadex (the trade name of Tamoxifen), the situation is obscene. Currently, Nolvadex sells for around $1200 for a year’s supply of the drug. The industry claims it needs to charge high prices for drugs in order to pay for expensive research and development, yet in the case of Tamoxifen, it is the NIH – not private industry – that has funded and continues to fund most of the clinical research. In 1999 alone, AstraZeneca pocketed more in pre-tax profit ($3.7 billion) and spent more on advertising and administration ($4.8 billion) than it spent on R&D (only $2.4 billion). Put in real terms, just 1.5% of the amount AstraZeneca profited in 1999 is enough to pay for a full year of Tamoxifen treatment for 45,000 women with breast cancer – the same amount of Americans that die each year of the disease according to the American Cancer Society.
The Sanders legislation requires the NIH to insure that drugs developed at taxpayer expense are provided to thepublic on reasonable terms. This anti-corporate welfare legislation is not a radical proposal; former NIHDirector Bernadine Healy called pharmaceutical overpricing of taxpayer-financed drugs “inhuman,” andPresident Bush instituted a reasonable pricing clause for drugs developed largely with government resources atNIH. TABLE OF CONTENTS PAGE 4: THE HISTORY OF TAMOXIFEN FROM DISCOVERY TO THE PRESENT PAGE 5: THE IMPORTANCE OF TAMOXIFEN IN FIGHTING BREAST CANCER PAGE 6: THE TAMOXIFEN PRICE GAP: HOW AMERICANS PAY THE HIGHEST PRICES IN THE WORLD PAGE 7: TAMOXIFEN AS DRUG INDUSTRY CASH COW: PROFITS AND FACTS PAGE 8:GRAPH: PROFITS FROM TAMOXIFEN OVER THE LAST 3 YEARS SKYROCKETING PAGE 9: GRAPH: GEOGRAPHY OF ASTRAZENECA PROFITS PAGE 10: FY1999 ASTRAZENECA ANNUAL FINANCIAL REPORT PAGE 11: CAROLYN TAPP, PRESIDENT, WOMEN OF COLOR BREAST CANCER SURVIVORS SUPPORT PROJECT, DESCRIBING WOMEN WHO CANNOT AFFORD TAMOXIFEN THE HISTORY OF TAMOXIFEN 1962: Tamoxifen patented by the British company Imperial Chemical Industries, Ltd. as a birth control pill 1971-1973: Dr. Mary Cole and England’s Christie Hospital begins early trials using Tamoxifen to treat advanced breast cancer in post-menopausal women 1978-1980: Study conducted at University of Pittsburgh as part of the taxpayer-funded National Surgical Adjuvant Breast and Bowel Project (NSABP) 1981-1988: NSABP studied 2,892 patients who received 5 years worth of Tamoxifen (“The Tamoxifen Story,” NCI website) 1987-1993: NSABP second phase of study included 1,166 patients (“The Tamoxifen Story,” NCI website) 1992-1998: Taxpayers fund a massive “Breast Cancer Prevention Trial,” studying 13,388 women over the course of more than 6 years. The study was conducted through the National Cancer Institute, a subsidiary of the NIH (Altman, NY Times, April 7, 1998) 1999: The American Society of Clinical Oncology – the nation’s largest group of cancer specialists – suggested that physicians should consider prescribing Tamoxifen to tens of millions of healthy women to help prevent the disease. PRESENTLY: The NIH is currently recruiting subjects for 25 new clinical trials to study new ways of using Tamoxifen in fighting breast cancer (NIH, www.clinicaltrials.gov) THE IMPORTANCE OF TAMOXIFEN HOW THE DRUG WORKS THE IMPORTANCE OF TAMOXIFEN LATEST STUDY: An eight-year National Cancer Institute study concluded in 1998 found that Nolvadex, the trade name of Tamoxifen, reduces breast cancer by up to 44% in women at high risk of developing the disease. This study was taxpayer-funded. STUDY DETAILS: 13,388 healthy women aged 35 years or older are at high risk of developing breast cancer at 131 clinical sites. The study had a 5-year duration, with a median follow-up of 4.2 years. In total 25% of patients took Nolvadex therapy or placebo for 5 years. EXPERT RECOMMENDATIONS: The American Society of Clinical Oncology - the nation’s largest group of cancer specialists - suggested on May 18th, 1999 that physicians should consider prescribing Tamoxifen to tens of millions of healthy women to help prevent the disease. The group said Tamoxifen "may be offered" to women who have at least a 1.7% risk of getting breast cancer over the next five years. About 29 million women, or 20 percent of the U.S. female population, are in this category, including all women over age 60. (Associated Press, May 19th, 1999) THE TAMOXIFEN PRICE DISCREPANCY How American taxpayers are charged the highest price for a drug they paid to develop UNITED STATES vs. CANADA: On average, Tamoxifen costs nearly 10 times more in the United States than in Canada, despite the fact that U.S. taxpayers paid huge sums of money over the course of two decares to develop the drug.
- BUS TRIPS: Several bus trips confirm that the prices for Tamoxifen in the United States are
significantly higher than anywhere else in the world. On Rep. Sanders’ bus trip fromVermont to Montreal in February, 2000, American consumers were able to purchase 180tablets of Tamoxifen at a price of $34, or less than 19 cents a pill. In Vermont, the same drugcost these consumers $241.67, or $1.34 per pill. In data from another trip from the Montanaborder, American consumers found that a $325 bottle of Tamoxifen in the United States, costless than $32 in Canada.
- LOWER PRICES IN CANADA STILL GET COMPANIES A PROFIT: After Sanders led
the first ever congressional bus trip to purchase drugs, the Montreal Gazette reported that eventhe low price offered at the Canadian pharmacy was 50% higher than the profitable pricecharged by the drug company. “[The prices] may sound cheap by American standards. But it's50% more than the $33.70 [the pharmacist] paid his wholesaler for the same pills.”
UNITED STATES vs. BRITAIN: According to the Oxford University School of Clinical Medicine, the price of 5 years of Tamoxifen costs between $333 - $666, and in most other countries it costs between $200-$800. However, in the United States, it costs about $6,000 for the same supply. (Oxford University School of Clinical Medicine, http://www.ctsu.ox.ac.uk/tamoxifen/tamqa.htm) EFFECTS OF HIGH PRICES IN U.S.: Though there is no comprehensive data on how many American breast cancer patients are unable to afford Tamoxifen, it is safe to say that thousands exist. Carolyn Tapp, who is the President of the Women of Color Breast Cancer Survivors Support Project in Los Angeles, described at a recent Congressional hearing how members of her group of 125 women were forced to share dosages of Tamoxifen and loan each other money because the price of the medication was so high (see page 11). OVERALL DISCREPANCY IN DRUG PRICES: Prices for prescription drugs in the United States continue to be much higher than in any other nation on earth. On average, a drug which costs $1 in the United States costs 60 cents in Germany, 57 cents in Canada, 51 cents in France and 49 cents in Italy. At the same time, each of these nations ranks higher than the United States in the latest World Health Organization’s report on overall health care systems. THE GROWING GAP: Overall, the gap in drug prices between the United States and the rest of the world continues to grow at an alarming rate. According to the Canadian Government, the gap in prices has grown nearly 12% in only 2 years. In other words, whereas American drug prices were 156% higher than the rest of the world in 1997, they are now more than 174% higher in 1999. TAMOXIFEN AS DRUG INDUSTRY CASH COW The multinational conglomerate AstraZeneca PC holds the monopoly in production of Nolvadex (the trade name ofTamoxifen). It will continue to hold the patent on Nolvadex until 2002. As these figures show, the industry is using theinflated prices for Nolvadex in the U.S. to fuel profits. Currently, the NIH spends millions of taxpayer dollars oncontinuing research on Nolvadex. At the same time, AstraZeneca charges Americans the highest prices for Nolvadex inthe world, and spends less on R&D than it allocates to advertising and pure profit.FY2000 FACTS OVERALL FIGURES: In the first quarter of 2000, AstraZeneca reported $632 million in overall profits. Nolvadex was responsible for $139 million in sales. GROWTH IN U.S. SALES: With drug prices rising, AstraZeneca’ s more than $2 billion in U.S. sales in the first quarter of 1999 represents a 16% over the first quarter of 1999. TAXPAYERS CONTINUE TO FUND MOST TAMOXIFEN BREAST CANCER R&D: According to NIH’s website which documents most clinical trials, the federal government is currently sponsoring at least 25 clinical trials to study Tamoxifen’s effects against against breast cancer, while none are being sponsored by private industry. (NIH website, www.clinicaltrials.gov) FY1999 FACTS OVERALL FIGURES: AstraZeneca reported more than $15.4 billion in sales, pocketing 24%, or nearly $3.7 billion, in pure profit before taxes. This is higher than the Fortune 500 pharmaceutical industry average 18.9% profit – the highest profit margin for any industry (AstraZeneca FY1999 Annual report, see page 10). NOLVADEX SALES JUMP: In just one year, AstraZeneca’s sales of Nolvadex jumped 7%, reaping $573 million in 1999 NOLVADEX SALES FUELED BY TAXPAYER-FUNDED RESEARCH: In 1998, the taxpayer- funded Breast Cancer Prevention Trial was completed, showing the positive effects of Tamoxifen in the fight against breast cancer. This was one of the largest studies ever conducted. According to AstraZeneca, this new data was instrumental in fueling Nolvadex’s profits: “The growth of Nolvadex sales represents increased prescribing in the USA following the publication of positive data across a range of indications, including reduction of risk of developing breast cancer.” (AstraZeneca annual report to shareholders, 1999) DEBUNKING THE “R&D” MYTH: Despite drug industry claims that high prices are needed to fuel research and development, companies profits and spending on advertising far outweigh spending on R&D. In FY1999 AstraZeneca reported spending only 16% ($2.4 billion) on research and development. In comparison, it reported pocketing more than 24% ($3.69 billion) in before-tax profits while spending more than 31% ($4.8 billion) on marketing and administration. MASSIVE SPENDING ON ADVERTISING NOLVADEX: As reported by the New York Times, AstraZeneca spent approximately $54.5 million on advertising Nolvadex in 1999. This amount is enough to pay for full treatments for more than 45,000 women – the same number of women who die each year of breast cancer (New York Times, June 30, 2000). U.S. SALES PROVIDE LION’S SHARE: In the United States, where the prices for its products are highest, AstraZeneca’s sales were up a whopping 23% over the year before. With prices for Nolvadex and other drugs substantially higher than anywhere else in the world, AstraZeneca made nearly half (48%) of its overall drug sales in the United States. In real dollars, the company made $7.1 billion in pharmaceutical revenues in the U.S., while making $7.6 billion in the rest of the world combined (see graph on page 9).
- ASTRAZENECA PAYS TINY AMOUNT OF TAXES: On top of the high drug prices and high
profits, the company paid only 7% in taxes on its $3.9 billion in profit. Breast Cancer Profiteering Revenues from Tamoxifen have skyrocketed into $500 million-a-year cash cow n (millions) ife 540 mox a 530 s of T 520 Fleecing America: AstraZeneca’s Profits AstraZeneca charges Americans up to 700% more forTamoxifen than in other countries - not surprisingly, nearlyhalf of its overall profits are made in the U.S.ASTRAZENECA CONSOLIDATED PROFIT AND LOSS ACCOUNT – FY1999 Continuing Operations Discontinued operations Operations Exceptional operations discontinued For the year ended 31 December 1998
Selling, general and administrative expenses
Group operating profit
Share of joint ventures’ and associates’ operating profits
Profits less losses on sale and closure of operations
Profit on ordinary activities before taxation Profit on ordinary activities after taxation Net profit for the financial year Profit retained for the financial year
Earnings per Ordinary Share before exceptional items
Weighted average number of Ordinary Shares in issue (millions)
Diluted average number of Ordinary Shares in issue (millions)
TRANSCRIPT OF THE HEARING IN THE SUBCOMMITTEE HEALTH AND
STATEMENT OF CAROLYN TAPP (Contact at 310-216-3200) President, Women of Color Breast Cancer Survivors Support Project
Good afternoon everyone. I am Carolyn Tapp, and I am President of the Women of Color Breast CancerSurvivor Support Project in Los Angeles. I appreciate the opportunity of being able to speak on behalf ofwomen of color and the underserved women in the Los Angeles area. Many of the women who are in ourgroup were screened through the CDC program, and they must have been the ones that fell through thecracks, because it wasn’t as easy as I have heard, you know, to get treatment. Some of the women I knowtook about 6 months to actually get treatment. And I think this is just unheard of.
I know of one lady who was diagnosed, and the day she was treated she found out that she qualified for theprogram, she passed away the very next day. So it really didn’t do her any good to go through this screeningand all that. And a lot of women do voice the fact that why should they be screened when they don’t gettreatment? And most times when they get treatment it is inadequate treatment. We are women who want tolive just like everyone else in this country.
This is a rich country, and we should be able to live and to go through the storm of breast cancer. I have known women who have had to borrow medication from other women in the group, because they couldn’t afford to buy the medication. I know that I loaned many women some of my medication Tamoxifen especially, because they were left out to get this kind of medication, and it costs hundreds of dollars. So they couldn’t afford to buy it. So we share. And we share a lot of things together in the group. Our group--we have about 125 women in the group; and, last year, we lost 13 women to breast cancer. And this year we have lost four, including our vice president of the organization, Mary Lee Matthews.
The majority of the women last year were screened through the program or they had found some other kindof treatment, and this leaves our women vulnerable to groups of people who come out and say I have atreatment or I have a cure, and we can take care of you, and they are so open and so--knowing that they don’thave money to be treated through the system, they go out and they get these different things--well, one thingis a kind of water they drink or some kind of root. And this is what is happening in our country. And a lot oftimes they are never offered reconstruction.
I have had women come in and tell me that they are using balloons with water to use as a prothesis. And thisshould not happen in our country. And like the lady this morning said, we have a $12 million grant ofmoneys, that money ran out. She should have said we had and we have. We had it. We don’t have it anymore. So I don’t know where to turn now when a woman comes in and tells me that she has been diagnosedor she is diagnosed through this program. I don’t know where or how to turn or where to tell her to go,because this program is running out. We must have adequate care for every woman in this country, no matterwhat her race is, what her financial standings are. We just must eradicate breast cancer, and we must havesome type of treatment, whether she is capable of paying or not, she shouldn’t be turned down. Because mostwomen in my community are heads of households.
They don’t have money. They have to make decisions. Should I go and get a treatment or should I stay athome? And this is because they know that nothing is out there, nothing is out there. So we must have a bill totake care of all of our women. All of our women in this country deserve--I know I deserve and I know all ofmy women deserve adequate treatment. Thank you.
2013 Minnesota Veterinary Fee Study – Written Submission Guide Thank you for your interest and participation in the 2013 Minnesota Veterinary Fee Study from VMS! This written submission guide is a print version of the survey that you may use to jot down answers and PLEASE NOTE: This is only a guide to assist in collecting the data you will need to complete the survey online.
The first thing we need to solve this question is to determine the relative length of amicrosecond. A quick search on the web determines the conversions we need:• 1 day = 24 hours × 60 minutes × 60 seconds = 8.64 ×1010 microseconds• 1 year = 365.25 days ≈ 3.16 × 1013 microsecondsNow if each function takes f (n) microseconds to complete and we wish to find the largestn such that the fu
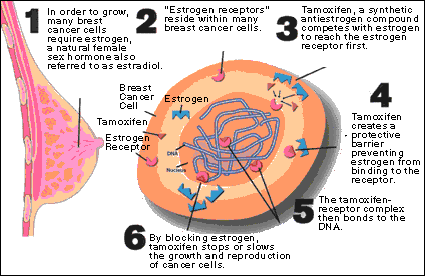 THE IMPORTANCE OF TAMOXIFEN
THE IMPORTANCE OF TAMOXIFEN