Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Acp-comparison of surgically repaired achilles tendon tears using platelet-rich fibrin matrices
Comparison of Surgically Repaired Achilles Tendon Tears Using Platelet-Rich Fibrin Matrices
Mikel Sánchez, Eduardo Anitua, Juan Azofra, Isabel Andía, Sabino Padilla and Iñigo Mujika
2007; 35; 245 originally published online Nov 12, 2006;
The online version of this article can be found at:
http://ajs.sagepub.com/cgi/content/abstract/35/2/245
Additional services and information for can be found at: American Journal of Sports Medicine
(this article cites 24 articles hosted on the
Citations
SAGE Journals Online and HighWire Press platforms):
2007 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. The American Journal of Sports Medicine
during the healing process of tendinous tissue.10,14
Furthermore, the healing tendon is also responsive to localapplication of growth factors.1,13,20,24,27,34 An autologous
platelet-rich fibrin (prepared from platelet-rich plasma)
Twelve athletes with spontaneous complete rupture of
secretes a complex mixture of biological mediators essen-
the Achilles tendon were treated operatively at the
tial to natural repair, including transforming growth
Arthroscopic Surgery Unit, USP–La Esperanza Clinic,
factor-β1 (TGF-β1), platelet-derived growth factor (PDGF),
Vitoria-Gasteiz, Spain, between 1997 and 2004. Approval
vascular endothelial growth factor (VEGF), epithelial
by the local ethics committee for the prospective use of
growth factor (EGF), hepatocyte growth factor (HGF), and
PRGF and written informed consent were obtained.
insulin-like growth factor (IGF-I). Because most of these
Exclusion criteria were previous tendon injury, history of
growth factors have been identified as playing key roles in
diabetes mellitus, platelet abnormality, hematologic abnor-
tendon healing,15,24 the use of autologous platelet-rich
mality, serum hemoglobin concentration <11 g/dL or hema-
plasma has been proposed as a strategy for enhancing the
tocrit <34%, use of systemic cortisone, and current use of
cellular response to injury within the tendon and, ulti-
anticoagulants. A 2-step application method of platelet-
rich therapy in conjunction with reconstructive surgery
An interesting new feature of the physiologic function of
was performed in 6 athletes treated from 2002 to 2004
platelets is their role as vehicles for the local delivery of
(Figure 1). Six of 11 athletes treated from 1997 to 2001,
growth factors in wound healing.4 At sites of vascular
selected by the same mechanism of injury, matched by age,
injury, platelets adhere and aggregate and also generate
gender, and physical activities, and who had the identical
thrombin, which triggers the production of a fibrin matrix
surgery procedure but without the application of platelet-
rich therapy, were identified retrospectively.
To derive benefit from this natural mechanism, we have
Two experienced orthopaedic surgeons of our group (M.S.
developed a procedure in which Ca2+ is added to plasma
and J.A.) performed all surgeries. All patients were male;
enriched in platelets, triggering the formation of a fibrin
descriptors of both groups are summarized in Table 1.
matrix containing embedded platelets. The resulting prepa-
Clinical evaluation and a positive Thompson sign, followed
ration rich in growth factors (PRGF) allows the slow release
by complementary ultrasound study (Logic 400 MD, GE
of biologically active proteins that initiate and modulate
Medical Systems, Milwaukee, Wis) or magnetic resonance
wound healing in both soft and hard tissues.4,6
imaging (high-resolution 1.5-T Magnetom Vision unit,
Previous studies by our group have shown that tendon
Siemens, Erlangen, Germany) were used to diagnose and
cells in vitro respond to the secreted pool of growth factors
confirm the complete Achilles tendon rupture in all
by proliferating, a basic response fundamental for repair.
patients. All cases were operated on no later than 2 weeks
Moreover, and also crucial for tissue healing, this treatment
elicited an angiogenic response based on the synthesis ofVEGF and HGF by tendon cells.5 This could be especiallyrelevant to the vascular status of tendons, assuming that the
low healing capability of tendons is associated with a reducedblood supply when compared with other tissues. From a
We studied quantitative aspects of PRGF in a group
kinetic point of view, fibrin matrix exerts a control of growth
of 21 volunteers affected by ligament, tendon, or muscle
factor release mimicking natural expression patterns; this
traumatic injuries, including the 6 athletes operated on
fact promoted a further examination of tendon cells cultured
with PRGF. The mean age of donors was 30.7 ± 7.1 years.
on autologous fibrin matrices and the effects of their admin-
Blood was collected in tubes with 5 mL trisodium citrate,
istration in vivo. Results demonstrated that PRGF is a safe
and then centrifuged at 460g for 8 minutes (PRGF System
strategy to accelerate tendon cell proliferation, stimulate
II, BTI, Vitoria-Gasteiz, Spain). The 1-mL fractions imme-
the synthesis of type I collagen, and promote neovascular-
diately above the erythrocyte pellet were collected from
ization both in vivo and in vitro.8 Moreover, other studies
each tube and transferred to sterile tubes, and the platelet
have reported the potential impact of platelet-rich fibrin on
count was determined. Care was taken to avoid collecting
impaired wound healing,12 which is considered the major
potential complication associated with operative treatment
For the in vitro determinations, a platelet-rich fibrin
matrix was formed by adding calcium chloride at a final
All these arguments provided the fundamentals for test-
concentration of 22.8 mM; clots were allowed to retract for
ing the defined PRGF in conjunction with the surgical treat-
1 hour at 37°C. The released supernatants were assayed
ment of a ruptured Achilles tendon in a preliminary
to provide relevant information about the concentration of
observational study in athletes, for whom accelerated func-
potentially therapeutic growth factors in platelet-rich
tional recovery is essential. Before February 2002, Achilles
plasma preparations such as PDGF-AB, TGF-β1, VEGF,
tendon surgery was performed using a surgical procedure
EGF, and plasmatic factors such as IGF-I and HGF. All
previously described.31 After February 2002, a method for
these factors were assessed utilizing commercially available
the application of PRGF during surgery was introduced.
enzyme-linked immunosorbent assay kits (Quantikine col-
Thus, we were able to study and compare 2 groups of
orimetric ELISA kits, R&D, Minneapolis, Minn), used accord-
patients: those who underwent the conventional surgical
ing to the manufacturer’s instructions. All measurements
procedure and those who underwent the same procedure
were performed in triplicate, and no unexpected scattering
combined with autologous PRGF therapy. 2007 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. Enhanced Tendon Healing With Autologous PlasmaFigure 1. The surgical procedure applying preparation rich in growth factors (PRGF). A, the ruptured ends of the Achilles tendon are approximated and sutured. B, injection of calcified unclotted plasma within the fascicles; the fibrin matrix develops in situ. C, the affected area is covered with an autologous platelet-rich fibrin matrix before closure of the overlying skin. D, subcutaneous infiltration of calcified unclotted PRGF before suturing.
For the surgical procedure, 40 mL of blood was drawn by
puncture from an antecubital vein 20 to 30 minutes before
surgery and before the administration of anesthesia.
Platelet-rich plasma was separated as explained above.
Four milliliters were supplemented with calcium chlorideat a final concentration of 22.8 mM and left to rest for 30
minutes in a glass container, allowing the fibrin scaffoldto develop before grafting. In addition, 4 mL of injectable
PRGF, in which calcium chloride was added just before
The same surgical technique was used in both groups.
Briefly, after debridement of the tendon edges, a polydiox-
anone (PDS) tape 5 mm large and 60 cm in length (Ethicon
Inc, Johnson & Johnson, Brussels, Belgium) is placed with
a V-40 half-circle needle using a Kessler technique in the
proximal stump. A second suture is placed in the distalstump. The knee is then flexed, and the foot is plantar
aPRGF, preparation rich in growth factors. Applicable values are
flexed; the ends of the suture can be tied without tension.31
mean (SD); no significant differences were found. 2007 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. The American Journal of Sports Medicine
The repair is then augmented using a 0-coated Vicril (CP
Medical, Johnson & Johnson, Belgium) vertical locking circumferential suture. In the platelet-rich treated group,
All patients underwent standardized ultrasound evalua-
approximately 4 mL of the activated plasma was injected
tion by 2 experienced musculoskeletal radiologists blinded
among the tendon fibers after the tendon was sutured.
to the surgical treatment (Logic 400 MD, GE Medical
After closing the paratenon and before closing the overly-
Systems, with 7.5-12.0 MHz linear array transducer). The
ing skin, the affected area was covered with the fibrin scaf-
interval between surgery and this examination was differ-
fold prepared as described above (Figure 1). Patients
ent between groups (control, 50 ± 11 months; PRGF, 32 ±
received a single preoperative dose of 2 g intravenous
10 months); however, both time intervals are long enough
cefonicid (Rottapharm, Valencia, Spain); a subcutaneous
to ensure complete remodeling of the scar. Patients were
dose of 2500 UI bemiparine (Hibor, Laboratorios Rovi,
examined in the prone position with the affected foot hang-
Madrid, Spain) was administered daily for 3 weeks postop-
ing over the end of the examination table. For each subject,
eratively, and 500 mg diclofenac was administered twice
ultrasound scans were performed at both Achilles tendons,
daily for a period up to 10 days or longer postoperatively as
4 to 5 cm proximal to the insertion with the ankle in neu-
tral position (90° of flexion). The Achilles tendon wasscanned transversely with the transducer perpendicular to
the Achilles tendon. The transducer was angled craniallyand caudally until the scan plane showed an Achilles ten-
A below-knee plaster cast with neutral position of the
don with maximum echogenicity. The cross-sectional area
ankle was used for 2 to 3 weeks; patients were allowed to
of the Achilles tendon was measured by trace ellipse
walk with elbow crutches for this period. At 2 to 3 weeks,
method so that the ellipse just surrounded the echogenic
the cast was removed, and the patients commenced an
boundary of the Achilles tendon.33 The intraclass correla-
active rehabilitation protocol instructed and supervised by
tion coefficient (ICC) of the cross-sectional area was 0.891;
a physical therapist blinded to the surgical treatment.
the upper 95% confidence interval (CI) was 0.915; the
A reduction in heel size (1.5 cm), followed by a gradual
lower 95% CI was 0.841, indicating a reproducibility of
increase in active and passive dorsiflexion, was begun.
89%. The cross-sectional area of the contralateral asymp-
Unloaded stationary bicycling and swimming were
tomatic tendon was used as a reference to calculate the
included later in this phase. Patients were authorized to
begin running daily for about 10 minutes based on tactileexploration, recovery of movement and calf strength
(based on the 1-footed tiptoe test, in which subjects arerequired to stand on tiptoes of the injured side for 5 sec-
All results are expressed as mean ± SD. Significant dif-
onds, 10 times), and examination of ultrasonographic
ferences among groups were evaluated using the Mann-
scans; intensity and duration were increased gradually as
Whitney U test. The mean cross-sectional area was
compared using the Student t test. Scatter plots andPearson correlations were used to examine the relation-ship between platelet counts and growth factor concentra-
tions. A difference of P < .05 was considered to be
Patients were examined by the operating surgeons; in
statistically significant (Statgraphics Plus, Manugistic,
general, time frames of follow-up were scheduled every
other week during the first month, every 4 to 6 weeks upto 6 months, and then after 9 and 12 months. Functional
outcome evaluation was based on the following 3 indica-tors: time necessary to reach full range of motion, time
needed to take up gentle running, and time to resumetraining activities. The range of motion of the ankle was
All ruptures were localized in the main body of the tendon,
measured using a goniometer (Biomet Inc, Warsaw, Ind)
at 4 to 5 cm proximal to the calcaneus insertion. Hospital
and compared with the contralateral ankle. The date on
stay was 48 hours for all patients. No patient had major
which surgeons authorized gentle running according to
complications such as rerupture or deep infection. All
the criteria above was used as an outcome indicator.
wound complications appeared in the control group. Two
Complications such as infections, wound healing defects,
patients presented keloid scars, but they did not require
subcutaneous tendon adhesions, symptoms of sural nerve
further treatment. Another patient suffered a superficial
injury, and calcifications were evaluated in both groups.
skin and subcutaneous infection 6 weeks after surgery and
Final decisions regarding suitability to return to practice
required surgical debridement that was followed by pri-
and competition remained solely with the sports medicine
mary closure. We did not find any calcification or altered
staff of each club. Data derived from closed questions to
the patients based on a simplified construct of Cincinnati
As shown in Table 1, sports activities were different
function scales30 were used to define the elapsed time
between the 2 groups, and patients in the PRGF group had
to get back to sporting activities, normal training, and
a higher demand of running and jumping. Figure 2 shows
the differences in the functional recovery of both groups. 2007 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. Enhanced Tendon Healing With Autologous Plasma
are particularly important because the growth factors aredirectly implicated in the healing process. For this aim,growth factor concentration was determined in the PRGFobtained from a total of 21 donors. The PRGF prepared asdescribed resulted in an increase in platelet concentration. In fact, the count of platelets in peripheral blood rangedfrom 142 × 103 to 379 × 103 (mean, 223 × 103 ± 71 × 103platelets/µL) and from 421 × 103 to 1314 × 103 (mean, 634
× 103 ± 217 × 103) in the PRGF. These data reflect thatPRGF had a 3.10-fold (SD, 0.58) increase in the meanplatelet concentration. Furthermore, the leukocyte contentwas also determined in the whole blood and in the PRGF. Results showed that white blood cell content in PRGF was
Figure 2. Differences in the functional recovery of 6 athletes
below the detection limit of the coulter, confirming the
treated with preparation rich in growth factors (PRGF) during
absence of leukocytes in the PRGF, which improves the
surgical reconstruction and a matched group that followed
homogeneity of the product and reduces donor-to-donor
conventional surgical procedure. Indices of functional out-
variability. The content of growth factors released from the
come: time necessary to reach total motion, take up gentle
activated PRGF was also measured for each donor. Mean
running, and resume training activities (mean ± SD). *P < .05.
levels of EGF, VEGF, and HGF were 481.5 ± 187.5 pg/mL,383.0 ± 374.9 pg/mL, and 593.87 ± 155.8 pg/mL, respectively.
All 3 indices of functional outcome (attainment of full
On the other hand, mean IGF-I, PDGF, and TGF-β concen-
range of ankle motion, time needed to be able to run gen-
trations were higher than the above-mentioned factors,
tly, and time to resume normal training activities) were
reaching 94.53 ± 32.84 ng/mL, 35.62 ± 14.57 ng/mL, and
significantly faster in the PRGF-treated group. At the indi-
74.99 ± 27.48 ng/mL, respectively. Another feature
vidual level, 2 professional athletes (soccer and basketball)
of this therapy is the significant positive correlation found
treated with PRGF returned to competition at a level sim-
between platelet count and the levels of TGF-β1 (r = .6157,
ilar to preinjury within 14 weeks after surgery. Two of the
P = .003), PDGF-AB (r = .6831, P < .001), VEGF (r = .5966, P=
amateur athletes in the PRGF group (soccer and basket-
.023), EGF (r = .5910, P = .029), and HGF (r = .6544,
ball) attained preinjury level by 6 months, whereas the 2
P = .008). Interestingly, IGF-I showed a significant inverse
remaining athletes (soccer) retired from competitive sports
correlation with age (r = –.6897, P < .001).
for reasons other than the injury; however, their level ofactivity was high (level 1 to 2, Cincinnati Scale). Beforeinjury, the Cincinnati Sports Activity Scale30 was similar
for control (90 ± 12 points) and PRGF athletes (88 ± 11
Surgical repair of the foot and ankle is now advancing
points). PRGF patients attained the same sports activity
toward minimally invasive surgery that tends to allow for
scores at 14 weeks (range, 2 weeks), while control athletes
a more rapid recovery with less pain. If operative treat-
scored 82 ± 11 points at 22 weeks (range, 8 weeks). In the
ment is the right solution, the goal is to minimize compli-
control group, 1 amateur athlete (basketball) returned to
cations related to the surgery and promote healing with
competitive participation and 5 athletes retired; this was a
early functional recovery that does not compromise repair.
common feature in Achilles tendon repairs during this
In clinical conditions such as Achilles tendon tears, the
period. Despite retiring from competitive participation, all
operative treatment offers a significant reduction in the
subjects reported they were in good fitness and continued
risk of rerupture and produces better functional results
performing in sport activities at a lower level and did not
when compared with nonoperative treatment, rendering
surgery the most recommended option in athletes.3,9However, the number of complications has been estimated
as 15% to 20%, rising in parallel with the increasing inci-
dence of ruptures in active people.3,18,21,26
Concerns about unpredictable impairment in healing
In both groups, the cross-sectional area of the operated
led us to treat tendon tears combining the principles of
tendon was significantly greater than the contralateral
biology and surgery by applying an autologous platelet-
tendons. The mean increase in cross-sectional area of the
rich fibrin during the operative treatment. The delivery of
repaired Achilles tendon 4 to 5 cm from the insertion in the
a complex pool of factors and proteins from the fibrin
calcaneus was 298% ± 90% and 499% ± 91% for the PRGF
matrix seeks to better meet the expected need for the
and the control group, respectively (t = 3.44, P = .009).
The idea of using fibrin as a therapeutic tool is not new.
Taking advantage of its adhesive properties was proposed
years ago as an alternative to suturing in Achilles tendonruptures.32 However, clinical results indicated that the
Initially, a full characterization of the main growth factors
procedure was not good enough to be recommended in
released from activated PRGF was performed. These data
2007 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. The American Journal of Sports Medicine
Concepts that have evolved since the development of fibrin
as matrix metalloproteinase-8, and release reactive oxygen
glues have given rise to the new platelet-rich technology that
species that destroy surrounding injured or healthy cells.6
overcomes some of the drawbacks associated with fibrin
Because part of this therapeutic strategy is to increase
glues. Although fibrin glues provide adhesive properties and
growth factor concentration at the injured site, we have
scaffolding function, they lack signaling factors. In fact, they
assessed the most relevant growth factors to tendon heal-
are prepared by polymerization of homologous lyophilized
ing.24 Although some of the individual roles of these factors
fibrinogen through the addition of massive thrombin. In con-
have been described in the scientific literature, their func-
trast, PRGF provides a bioactive scaffold offering a highly
tions could be modified by the presence of other molecules.
complex pool of signaling factors critical to ensure cell acti-
For example, the presence of TGF-β1 could provide some
vation and the successful growth of healthy tissue. In previ-
concerns about application of this therapeutic strategy, as
ous studies, we showed that tendon cells seeded on
this protein is associated with excessive collagen deposi-
autologous PRGF proliferate and synthesize type I collagen,
tion and scar tissue formation, damaging the mechanical
in contrast to fibrin glue. Moreover, tenocytes elicited an
properties of the repaired tissue. We addressed this issue
angiogenic response by synthesizing VEGF and HGF.8
in previous experimental studies and showed that the
Assuming these effects, PRGF treatment would enhance the
effect of TGF-β1 on collagen synthesis was counteracted
quality of tendon repair and the time of healing.
by the presence of other platelet-secreted molecules.7
We explored the relevance of applying PRGF during
Furthermore, when several doses of this plasma were
open surgery in a group of athletes. The treatment con-
injected weekly in Achilles tendons in sheep, no signs of
sisted of replacing the natural hematoma, containing a
fibrosis were observed, implying that the use of fibrin
bulk of red blood cells (about 94%) and a little proportion
matrices may be a safe strategy to initiate and promote
of platelets (6%) and <1% leukocytes, with PRGF, which
healing in damaged tendons.8 Supporting these findings,
merely contains platelets embedded in a fibrin matrix.
our preliminary clinical evidence with PRGF resulted in
The fact that tendons are often subjected to high or
less increase in width and cross-sectional area in platelet-
unusual loads during sports participation reflects better
rich–treated tendons in contrast with the control group,
the functional efficacy of this novel procedure. Our study
indicating a more physiologic repair with less scar tissue.
population included 12 carefully matched athletes with
In addition, it has been reported that platelets also store
total tears of the Achilles tendon. The functional results
antibacterial and fungicidal proteins that could prevent
using this surgical repair and postoperative rehabilitation
infection, although this has yet to be proved.19
protocol were within the reported outcomes for this
The method described for the preparation of PRGF is
injury.22,25 Despite the fact that all athletes did well with
easy to implement and to handle and is applied in a sim-
Achilles repair, the PRGF group required a shorter time in
ple way. The risk of disease transmission or an antigenic
the recovery of motion and return to sporting activities; the
reaction is nonexistent because autologous blood is not
latter was a decision that came solely from the sports med-
mixed with any other component of animal or human
icine staff rather than the operating surgeons.
We report 100% healing without any delayed wound
Based on this preliminary study, we suggest that the
healing, sural nerve injury, or superficial or deep infection
operative management of Achilles tendon tears associated
in the PRGF-treated group. In contrast, minor complica-
with the application of autologous platelet-rich fibrin could
tions including 1 superficial infection and 2 keloids were
present new possibilities for enhanced healing and func-
described in the control group. Although this study is
tional recovery. Although these preliminary results need
merely observational, the reported results are in accor-
confirmation in a large cohort of patients, they provide
dance with the proven efficacy of platelet-rich derived
useful information about the safety of this new surgical
therapies in other clinical areas,4 including the treatment
procedure and open new perspectives in the area of sports
of chronic leg ulcers,23 articular cartilage surgery,29 and
medicine, where acceleration of healing is paramount.
anterior cruciate ligament reconstruction.28
Our study has some inherent weaknesses. It is a retro-
spective study, and although it represents the first descrip-
tion of tendon treatment with an autologous platelet-
The authors are grateful to Dr Yangüela and Dr Orive for
rich preparation reported in the literature, the number of
their magnetic resonance imaging and ultrasonography
patients is small. Further clinical studies are needed to
expertise. The work of this group is partially funded by the
determine the validity of the procedure.
Fully understanding the influence of platelet-rich
therapy on healing is an area of developing research. However, advancement in this technology is hindered by
REFERENCES
the lack of a suitable qualitative and quantitative stan-dardization of the different preparations. Our group has
1. Abrahamsson SO. Similar effects of recombinant human insulin-like
growth factor-I and II on cellular activities in flexor tendons of young
developed an optimized and standardized product known
rabbits: experimental studies in vitro. J Orthop Res. 1997;15:256-262.
as PRGF that avoids the use of exogenous thrombin.
2. Ambacher T, Kuhn P, Schmidt R, Disselhorst-Klug C, Paar O. Muscle
From a safety point of view, PRGF does not contain neu-
strength and functional results after surgical repair of Achilles tendon
trophils, which express matrix-degrading enzymes, such
rupture with fibrin gluing. Zentralbl Chir. 2001;126:989-994.
2007 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. Enhanced Tendon Healing With Autologous Plasma
3. Amendola N. Surgical treatment of acute rupture of the tendon
20. Kurtz CA, Loebig TG, Anderson DD, Demeo PJ, Campbell PG. Insulin-
Achillis led to fewer reruptures and better patient-generated ratings
like growth factor I accelerates functional recovery from Achilles
than did nonsurgical treatment. J Bone Joint Surg Am. 2002;84:324.
tendon injury in a rat model. Am J Sports Med. 1999;27:363-369.
4. Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous
21. Leppilahti J, Forsman K, Puranen J, Orava S. Outcome and prognos-
platelets as a source for healing and tissue regeneration. Thromb
tic factors of Achilles rupture repair using a new scoring method. ClinOrthop Relat Res. 1998;364:152-161.
5. Anitua E, Andia I, Sanchez M, et al. Autologous preparations rich in
22. Maffulli N, Tallon C, Wong J, Peng Lim K, Bleakney R. No adverse
growth factors promote proliferation and induce VEGF and HGF produc-
effect of early weight bearing following open repair of acute tears of
tion by human tendon cells in culture. J Orthop Res. 2005;23:281-286.
the Achilles tendon. J Sports Med Phys Fitness. 2003;43:367-379.
6. Anitua E, Sanchez M, Nurden AT, Nurden P, Orive G, Andia I. New
23. Margolis DJ, Kantor J, Santana J, Strom BL, Berlin JA. Effectiveness
insights into and novel applications for platelet-rich therapies. Trends
of platelet releasate for the treatment of diabetic neuropathic foot
ulcers. Diab Care. 2001;24:483-488.
7. Anitua E, Sanchez M, Nurden AT, et al. Reciprocal actions of platelet-
24. Molloy T, Wang Y, Murrell GAC. The roles of growth factors in tendon
secreted TGF-b1 on the production of VEGF and HGF by human ten-
and ligament healing. Sports Med. 2003;33:381-394.
don cells. Plast Reconstr Surg. In press.
25. Mortensen NHM, Skov O, Jensen PE. Early motion of the ankle after
8. Anitua E, Sanchez M, Nurden AT, et al. Autologous fibrin matrices:
operative treatment of a rupture of the Achilles tendon: a prospective,
a potential source of biological mediators that modulate tendon cell
randomized clinical and radiographic study. J Bone Joint Surg Am.
activities. J Biomed Mater Res A. 2006;77:285-293.
9. Bhandari M, Guyatt GH, Siddiqui F, et al. Treatment of acute Achilles
26. Pajala A, Kangas J, Ohtonen P, Leppilahti J. Rerupture and deep
tendon ruptures: a systematic overview and metaanalysis. Clin
infection following treatment of total Achilles tendon rupture. J BoneOrthop Relat Res. 2002;400:190-200. Joint Surg Am. 2002;84:2016-2021.
10. Boyer MI, Watson JT, Lou J, Manske PR, Gelberman RH, Cai SR.
27. Rickert M, Jung M, Adiyaman M, Richter W, Simank HG. A growth
Quantitative variation in vascular endothelial growth factor mRNA
and differentiation factor-5 (GDF-5)-coated suture stimulates tendon
expression during early flexor tendon healing: an investigation in a
healing in an Achilles tendon model in rats. Growth Factors.
canine model. J Orthop Res. 2001;19:869-872.
11. Bruggeman NB, Turner NS, Dahm DL, et al. Wound complications after
28. Sánchez M, Azofra J, Aizpurúa B, Elorriaga R, Anitua E, Andía I. Use
open Achilles tendon repair. Clin Orthop Relat Res. 2004;427:63-66.
of autologous plasma rich in growth factors in arthroscopic surgery [in
12. Carter CA, Jolly DG, Worden CE, Hendren DG, Kane CJM. Platelet-
Spanish]. Cuadernos de Artroscopia. 2003;10:12-19.
rich plasma gel promotes differentiation and regeneration during
29. Sánchez M, Azofra J, Anitua E, et al. Plasma rich in growth factors to
equine wound healing. Exp Mol Pathol. 2003;74:244-255.
treat an articular cartilage avulsion: a case report. Med Sci Sports
13. Chan BP, Fu SC, Qin L, Lee KM, Rolf CG, Chan KM. Effects of basic
fibroblast growth factor (bFGF) on early stages of tendon healing:
30. Smith FW, Roselund EA, Aune AK, MacLean JA, Hillis SW. Subjective
a rat patellar tendon model. Acta Orthop Scand. 2000;71:513-518.
functional assessments and the return to competitive sport after
14. Dahlgren LA, Mohammed HO, Nixon AJ. Temporal expression of
anterior cruciate ligament reconstruction Br J Sports Med.
growth factors and matrix molecules in healing tendon lesions.
31. Wapner KL. Acute repair of the Achilles tendon. In: Johnson KA, ed.
15. Hsu CH, Chang J. Clinical implications of growth factors in flexor ten-
The Foot and Ankle. New York, NY: Raven Press; 1991:299-309.
don wound healing. J Hand Surg [Am]. 2004;29:551-563.
32. Winter U. Treatment of fresh Achilles tendon ruptures with fibrin glue.
16. Kannus P, Jósza L, Järvinen M. Epidemiology and histology of
Aktuelle Traumatol. 1985;15:219-221.
Achilles tendon rupture. Foot Ankle Clin. 1997;2:475-500.
33. Ying M, Yeung E, Li B, Li W, Lui M, Tsoi CW. Sonographic evaluation
17. Kannus P, Natri A. Etiology and pathophysiology of tendon ruptures
of the size of Achilles tendon: the effect of exercise and dominance of
in sports. Scand J Med Sci Sports. 1997;7:107-112.
the ankle. Ultrasound Med Biol. 2003;29:637-642.
18. Khan RJ, Fick D, Brammar TJ, Crawford J, Parker MJ. Interventions for
34. Yoshikawa Y, Abrahamsson O. Dose-related cellular effects of
treating Achilles tendon ruptures. The Cochrane Library. 2005;2:1-54.
platelet-derived growth factor-BB differ in various types of rabbit ten-
19. Krijgsveld J, Zaat SA, Meeldijk J, et al. Thrombocidins, microbicidal
dons in vitro. Acta Orthop Scand. 2001;72:287-292.
proteins from human blood platelets, are C-terminal deletion prod-ucts of CXC chemokines. J Biol Chem. 2000;265:20374-20381. 2007 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution.
Nebulisers Nebulisers You should only use a nebuliser if your doctor has advised you to do so. This information sheet is designed for people already using a nebuliser and is only intended to be used as a guide. You should always discuss the use of your medicines with your doctor or nurse. A nebuliser is a powerful drug delivery system. It should only be used if your doctor has
B.C.’S ECONOMIC ADVISORY COUNCIL David Emerson, chair David Emerson is CEO and chair of the BC Transmission Corporation and senior advisor for CAI Capital Management, a private equity firm. He was a federal Member of Parliament from 2004-2008, during which time he served as Minister of Industry, Minister of International Trade and Minister of Foreign Affairs. He has served in chief e

 Comparison of Surgically Repaired Achilles Tendon Tears Using Platelet-Rich Fibrin Matrices
Comparison of Surgically Repaired Achilles Tendon Tears Using Platelet-Rich Fibrin Matrices The American Journal of Sports Medicine
during the healing process of tendinous tissue.10,14
Furthermore, the healing tendon is also responsive to localapplication of growth factors.1,13,20,24,27,34 An autologous
platelet-rich fibrin (prepared from platelet-rich plasma)
Twelve athletes with spontaneous complete rupture of
secretes a complex mixture of biological mediators essen-
the Achilles tendon were treated operatively at the
tial to natural repair, including transforming growth
Arthroscopic Surgery Unit, USP–La Esperanza Clinic,
factor-β1 (TGF-β1), platelet-derived growth factor (PDGF),
Vitoria-Gasteiz, Spain, between 1997 and 2004. Approval
vascular endothelial growth factor (VEGF), epithelial
by the local ethics committee for the prospective use of
growth factor (EGF), hepatocyte growth factor (HGF), and
PRGF and written informed consent were obtained.
The American Journal of Sports Medicine
during the healing process of tendinous tissue.10,14
Furthermore, the healing tendon is also responsive to localapplication of growth factors.1,13,20,24,27,34 An autologous
platelet-rich fibrin (prepared from platelet-rich plasma)
Twelve athletes with spontaneous complete rupture of
secretes a complex mixture of biological mediators essen-
the Achilles tendon were treated operatively at the
tial to natural repair, including transforming growth
Arthroscopic Surgery Unit, USP–La Esperanza Clinic,
factor-β1 (TGF-β1), platelet-derived growth factor (PDGF),
Vitoria-Gasteiz, Spain, between 1997 and 2004. Approval
vascular endothelial growth factor (VEGF), epithelial
by the local ethics committee for the prospective use of
growth factor (EGF), hepatocyte growth factor (HGF), and
PRGF and written informed consent were obtained.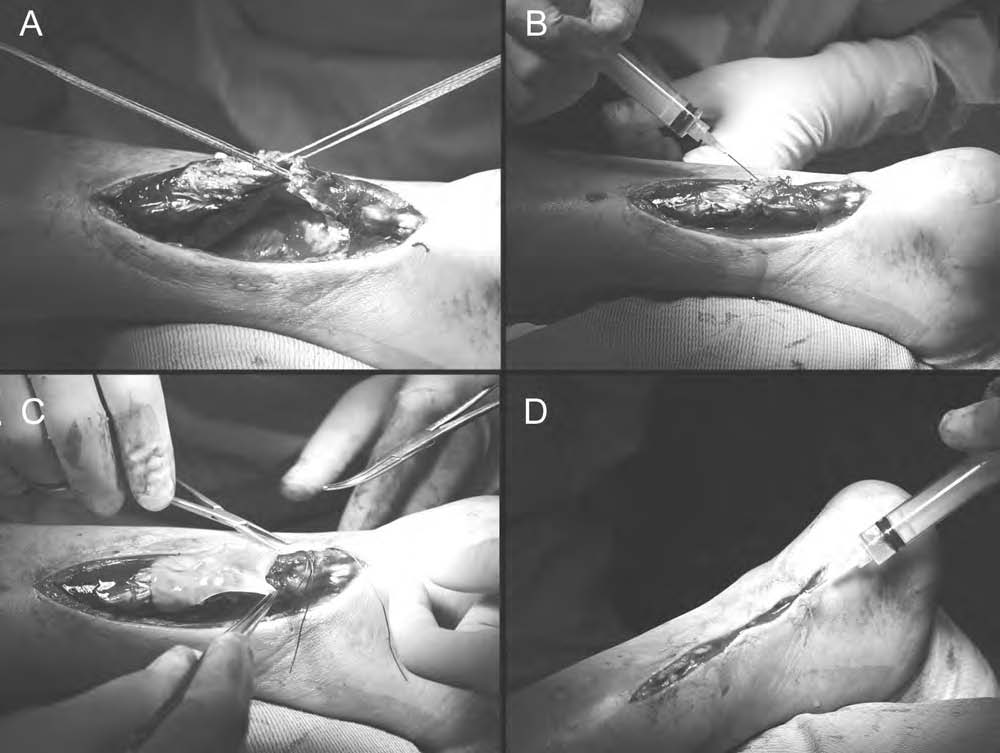 Enhanced Tendon Healing With Autologous Plasma
Figure 1. The surgical procedure applying preparation rich in growth factors (PRGF). A, the ruptured ends of the Achilles tendon
Enhanced Tendon Healing With Autologous Plasma
Figure 1. The surgical procedure applying preparation rich in growth factors (PRGF). A, the ruptured ends of the Achilles tendon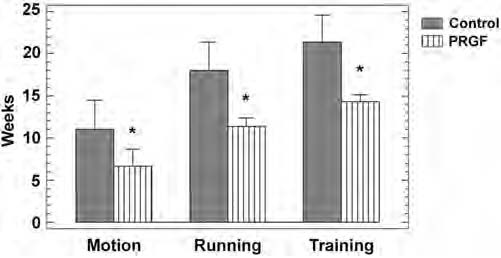 Enhanced Tendon Healing With Autologous Plasma
are particularly important because the growth factors aredirectly implicated in the healing process. For this aim,growth factor concentration was determined in the PRGFobtained from a total of 21 donors. The PRGF prepared asdescribed resulted in an increase in platelet concentration.
Enhanced Tendon Healing With Autologous Plasma
are particularly important because the growth factors aredirectly implicated in the healing process. For this aim,growth factor concentration was determined in the PRGFobtained from a total of 21 donors. The PRGF prepared asdescribed resulted in an increase in platelet concentration.