Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Mw3538-andrews
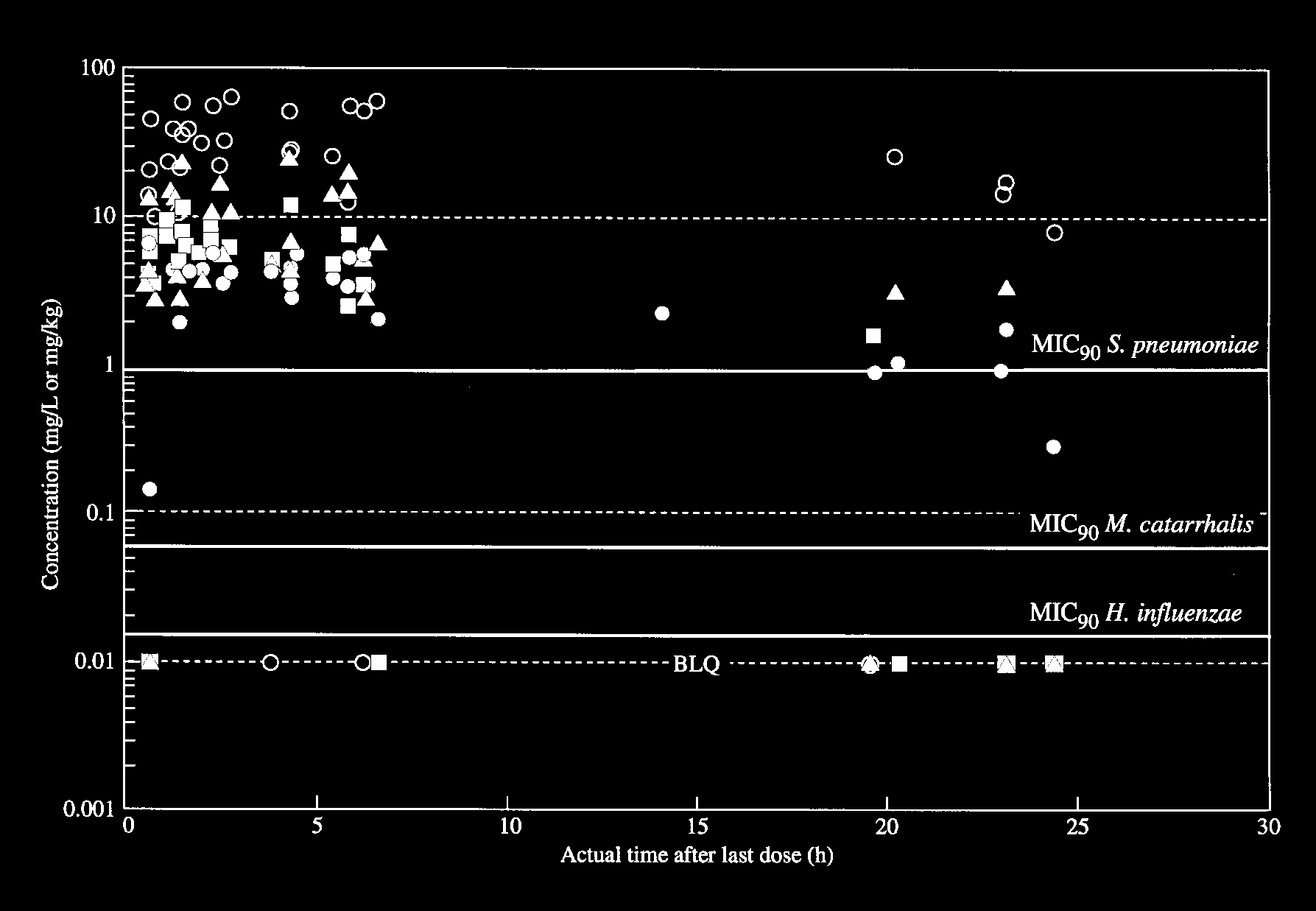
Journal of Antimicrobial Chemotherapy (1997) 40, 573–577 Concentrations of levofloxacin (HR 355) in the respiratory tract following a single oral dose in patients undergoing fibre-optic bronchoscopy J. M. Andrewsa, D. Honeybourneb, G. Jevonsa, N. P. Brenwalda, B. Cunninghamb and R. Wisea Departments of aMedical Microbiology and bThoracic Medicine, City Hospital NHS Trust, Birmingham, UKConcentrations of levofloxacin were measured in bronchial biopsies, alveolar macrophages (AM), epithelial lining fluid (ELF) and serum following a single oral dose. Concentrations were measured by a microbiological assay method. A total of 35 patients undergoing fibre-optic bronchoscopy were studied. Mean serum, AM, ELF and biopsy concentrations were as follows. 0.5 h: 4.73 mg/L, 19.1 mg/L, 4.74 mg/L and 4.3 mg/kg; 1 h: 6.6 mg/L, 32.5 mg/L, 10.8 mg/L and 8.3 mg/kg; 2 h: 4.9 mg/L, 41.9 mg/L, 9.0 mg/L and 6.5 mg/kg; 4 h: 4.1 mg/L, 27.7 mg/L, 10.9 mg/L and 6.0 mg/kg; and 6–8 h: 4.0 mg/L, 38.4 mg/L, 9.6 mg/L and 4.0 mg/kg respectively. Mean serum and AM concentrations at 12–24 h were 1.2 and 13.9 mg/L respectively (con- centrations in biopsy and ELF were only measurable in three of the six patients). These concentrations exceed the MIC90s of the common respiratory pathogens, Haemophilus influenzae (0.015 mg/L), Moraxella catarrhalis (0.06 mg/L) and Streptococcus pneumoniae (1 mg/L) and suggest that levofloxacin should be efficacious in the treatment of community- and hospital-acquired respiratory infection. Introduction
Levofloxacin (HR 355), a quinolone antibacterial, is the bilirubin
85 mol/L or a history of encephalopathy).
L-isomer of the racemate ofloxacin.1 In general, it has a
Patients with a history of allergy to quinolones, multiple
broad spectrum of activity and is equal to or up to four-
drug sensitivity or photosensitivity were also excluded.
fold more active than ofloxacin.2 The aim of this study was
Patients were also excluded if they were taking antacids,
to compare concentrations of levofloxacin at potential sites
anticoagulants, iron salts or anti-epileptic drugs.
of respiratory infection, bronchial mucosa, epithelial liningfluid (ELF) and alveolar macrophages (AM) with simulta-neous serum concentrations, up to 24 h after a single 500
This was an open study designed to measure concentra-tions of levofloxacin in bronchial tissues and fluids follow-
Materials and methods
ing the administration of a single 500 mg oral dose. Afterovernight fasting (depending on time of administration
A total of 35 patients (24 males, 11 females) undergoing
of drug) a single 500 mg oral dose was administered with
elective diagnostic bronchoscopy were studied. All of the
50 mL of non-aerated water. Patients were allocated
patients were over 18 years of age and all of the females
randomly into six bronchoscopy groups as follows: Group
were post-menopausal. The study was approved by the
1, 0.5 h post-dose; Group 2, 1 h post-dose; Group 3, 2 h
Hospital Ethicis Committee and all patients gave written
post-dose; Group 4, 4 h post-dose; Group 5, 6–8 h post-
Patients were excluded from the study if there was
evidence of an active lung infection, if they were receiving
antibiotic therapy or if their respiratory status was severelycompromised. Subjects with significant renal impairment
A standard pre-medication of 160 mg of 4% nebulized
(determined by a serum creatinine of more than 220
lignocaine, 0.6 mg atropine intramuscularly and 2.5–5 mg
mol/L), serious hepatic disease (reflected by any one of
1997 The British Society for Antimicrobial Chemotherapy
J. M. Andrews et al.
Assay plates were incubated for 18–20 h at 30°C and,
after incubation, zones of inhibition were measured and
A standard bronchoalveolar lavage (BAL) was performed
calculated using an image analyser (Vidas 2.5, Imaging
using 200 mL of pre-warmed 0.9% sodium chloride
Associates, Thame, UK) programmed to construct a line
(divided into four 50 mL aliquots) followed by gentle
of best fit using Bennett’s calculation.5 The lower limit of
aspiration. The aspirate from the first 50 mL was discarded
detection of the assay was 0.06 mg/L. All measurable
to avoid contamination of the sample with larger airway
concentrations were within the standard curve. Antibiotic
fluids and cells,3 and any residual lignocaine which might
concentration in the bronchial biopsy was calculated from
affect the microbiological assay. The remaining three
aspirates were pooled, and then divided into two Tefloncontainers (to avoid the loss of macrophages sticking to
surfaces) for analysis. Immediately, in the endoscopy suite,
a small sample was removed using silanized glassware and
placed in an improved Neubauer counting chamber so that
A is the assayed concentration (mg/L), CT is the
tissue concentration (in mg/kg), V is the diluent volume (in
the number and type of cells present could be determined
mL), and W is the weight of tissue (mg).
microscopically. The remaining sample was centrifuged at 400g for 5 min. After centrifugation the supernatant was separated immediately from the cells. Approximately Calculation of antibiotic concentration in ELF 2 mL of the supernatant was removed for urea estimation.
The urea concentration in the BAL was determined using
The remaining fluid was used to measure the concentra-
a modified Sigma Diagnostic kit (UV-66, Sigma Chemi-
tion of levofloxacin present by freeze drying and reconsti-
cals, Poole, UK). The assay was linear over the range
tution in HPLC grade distilled water to one-tenth of the
0.01–0.09 mmol/L. The concentration of levofloxacin was
original volume. Macrophages were ultrasonicated on ice
calculated using the method described by Renard et al.,6 as
in a known volume of chilled pH 7 phosphate buffer
(100% duty cycles, Misonix Model XL2015, Life ScienceLaboratories, Luton, UK) before assay. Bronchial biopsy
tissue was collected into a humidity chamber to avoid loss
of moisture from the tissue before weighing.4 Tissue was
weighed (discarding any blood-stained tissue) and then
BAL is the concentration of antibiotic in BAL
ultrasonicated in buffer as previously described. Blood
ELF is the concentration of antibiotic in ELF
samples were taken at the end of the endoscopy for
the assay of levofloxacin and urea. All samples for assay
were stored at 4°C in the dark. With the exception of thelavage supernatant, all samples were assayed within 1 h ofcollection. Calculation of antibiotic concentration inmacrophages
Using data derived by Johnson et al.7 antibiotic concentra-tion was determined assuming a mean AM cell volume of
Concentrations of levofloxacin were measured using
methodology previously externally validated by the R. W. Johnson Pharmaceutical Research Institute (Raritan, NJ,USA). Briefly, levels were determined using Iso-Sensitest
agar (CM471i Unipath, Basingstoke, UK) and Escherichiacoli 4004 (Bayer AG, Wuppertal, Germany). Calibrators,
In Table I are summarized the results for the internal
internal controls (fixed concentrations prepared from controls and quality assurance samples. These data con-a different weighing of standard material) and quality
firm the reliability of the urea and microbiological assay
assurance samples (variable concentrations similar to
those expected from the patient samples), were prepared
The mean lavage volume, lavage urea, macrophage
in pooled human serum (Bradsure Biologicals, Lough-
count and biopsy weight for the patient samples were
borough, UK) for human serum samples, pH 7 phosphate
44.44 mL (S.D. 18.15), 0.052 mmol/L (S.D. 0.034), 2.13
buffer for tissue and macrophage samples and 9% sodium
cells/mL (S.D. 2.13) and 8.5 mg (S.D. 3.31), respectively.
chloride for the concentrated BAL samples. The calibrator
Concentrations of levofloxacin in serum, biopsy, ELF
concentrations were 0.125, 0.25, 0.5, 1 and 2 mg/L. The
and AM including site:serum ratios, are summarized in
internal control samples were 1.5 and 0.2 mg/L and the
Table II. A plot of the corresponding data is shown in the
quality assurance samples ranged from 0.15 to 1.8 mg/L.
All samples were assayed in triplicate.
The highest serum and biopsy concentration were seen
Levafloxacin concentrations in respiratory tract Table I. Results for urea and levofloxacin internal controls and levofloxacin quality Table II. Summary of mean levofloxacin concentrations in serum, biopsy, epithelial
lining fluid (ELF) and alveolar macrophages (AM) in patients undergoing fibre-optic
bronchoscopy following a single 500 mg oral dose
J. M. Andrews et al. Figure. Concentrations of levofloxacin in patients undergoing fibre-optic bronchoscopy following a single oral 500 mg dose.
, biopsy; ▲, epithelium lining fluid; , alveolar macrophages; BLQ, below limit of quantification.
1 h post-dose (mean levels 6.6 mg/L and 8.3 mg/L, respec-
comparable site:serum ratios (at 4 h post-dose) were found
tively). Mean ELF concentrations were very similar at 1, 2,
for all three agents except that the AM ratio for levo-
4 and 6–8 h post-dose (10.8, 9.0, 10.9 and 10.1 mg/L, respec-
floxacin (9.1:1) was greater than those of ciprofloxacin
tively). Highest AM concentrations were recorded 2 h
post-dose (mean 41.9 mg/L). In the 12–24 h group levo-
The mean serum, biopsy, ELF and AM concentrations
floxacin was not detected in biopsy samples in four of the
in all of the groups up to 6–8 h exceeded the MIC90s of the
six subjects and in ELF from three of the six subjects.
common respiratory pathogens (MIC90s for Streptococcus.
Assuming a site:serum ratio of 1 for the biopsy samples
pneumoniae, Moraxella catarrhalis and Haemophilus
and using the equation to calculate the amount of tissue
influenzae were 1, 0.06 and 0.015 mg/L respectively;
needed to measure the level of levofloxacin, in all cases the
unpublished data), by at least two-fold; this is important
amount of tissue obtained at biopsy was insufficient for
because earlier quinolones such as ciprofloxacin have only
borderline activity. The concentration of levofloxacin
Five subjects experienced mild headaches and eight within the AM suggests that the agent will be clinically
subjects reported mild dizziness which the investigators
active against ‘atypical’ pathogens associated with commu-
felt may have been due to the antibiotic.
nity-acquired infections (Chlamydia pneumoniae andMycoplasma pneumoniae MIC90s of 0.5 mg/L).9,10
Discussion
This study suggests that levofloxacin at a dose of 500 mg
given twice a day should be effective in a wide range of
This study has shown clinically significant pulmonary
concentrations of levofloxacin following a single 500 mgdose. Concentrations were below the limit of quantifica-
Acknowledgements
tion in the majority of ELF and biopsy samples taken inthe 12–24 h post-dose group.
We would like to acknowledge the help of Dr W. Weber
When the results obtained with levofloxacin are and also Dr P. Mendes from Hoechst AG, Frankfurt,
compared with those of ciprofloxacin and temafloxacin8
Levafloxacin concentrations in respiratory tract References 7. Johnson, J. D., Hand, W. L., Francis, J. B., King-Thompson, N. L. & Corwin, R. W. (1980). Antibiotic uptake by alveolar 1. Fujimoto, T. & Mitsuhashi, S. (1990). In vitro antibacterial macrophages. Journal of Laboratory Clinical Medicine
activity of DR-3355, the S-(–) isomer ofloxacin. Chemotherapy 36, 8. Wise, R., Baldwin, D. R., Andrews, J. M. & Honeybourne, D. 2. Fu, K. P., Lafredo, S., Foleno, B., Isaacson, D. M., Barrett, J. F.,
(1991). Comparative pharmacokinetic disposition of fluoroquino-
Tobia, A. J. & Rosenthale, M. E. (1992) In vitro and in vivo anti-
lones in the lung. Journal of Antimicrobial Chemotherapy 28,
bacterial activities of levofloxacin (L-ofloxacin), an optically active
ofloxacin. Antimicrobial Agents and Chemotherapy 36, 860–6. 9. Hammerschlag, M. R., Qumei, K. K. & Roblin, P. M. (1992). In 3. Kelly, C. A., Kotre, C. J., Ward, C., Hendrick, D. J. & Walters,
vitro activities of azithromycin, clarithromycin, L-ofloxacin and other
E. H. (1987) Anatomical distribution of bronchoalveolar lavage fluid
antibiotics against Chlamydia pneumoniae. Antimicrobial Agents
as assessed by digital subtraction radiography. Thorax 42, 624–8. and Chemotherapy 36, 1573–4. 4. Cars, O. & Ogren, S. (1981). A microtechnique for the determi- 10. Sanghrajka, M., Felmingham, D. & Ridgway, G. L. (1991).
nation of antibiotics in muscle. Journal of Antimicrobial Chemo -
Comparative in vitro activity of the quinolone DR-3355 against
therapy 8, 39–48. Mycoplasma pneumoniae, Mycoplasma hominis and Ureaplasmaurealyticum. In Proceedings of the Third International Symposium5. Bennett, J. V., Broche, J. L., Benner, E. J. & Kirby, W. M. M. on New Quinolones (Rubinstein, E., Ed.), Vancouver, Canada,
(1966). Simplified, accurate method for antibiotic assay of clinical
1990. European Journal of Clinical Microbiology and Infectious
specimens. Applied Microbiology 14, 170–7. Diseases, Special Issue, pp. 237–8. 6. Rennard, S. I., Basset, G., Lecossier, D., O’Donnell, K. M., Martin, P., Pinkston, P. et al. (1986). Estimation of volume of epithelial lining fluid recovered by lavage using urea as a marker Received 7 January 1997; returned 27 February 1997; returned 21
of dilution. Journal of Applied Physiology 60, 532–8.
PLEASE POST THIS PAGE IN AREAS WHERE NON-HUMAN PRIMATES AND PRIMATE TISSUES ARE USED IN RESEARCH LABORATORIES UNIVERSITY OF CALIFORNIA, SAN FRANCISCO ENVIRONMENTAL HEALTH AND SAFETY/BIOSAFETY HERPES B VIRUS EXPOSURE/INJURY RESPONSE PROTOCOL Organism or Agent: Macacine herpesvirus 1 Exposure Risk: Herpes B virus UCSF Occupational Health Services: 415/885-75
Federazione Energia Moda Chimica e Affini della CISL Segreteria Territoriale dell’Udinese e Bassa Friulana F e d e r a t i o n o f E n e r g y F a s h i o n C h e m i c a l a n d S i m i l a r I n d u s t r i e s ' W o r k e r s LA PROVINCIA DI UDINE E LA REGIONE FRIULI VENEZIA GIULIA CREDONO NELL’INDUSTRIA CHIMICA AD ALTO CONTENUTO TECNOLOGICO E INNOVATIVO? La domanda pone una seri
 J. M. Andrews et al.
J. M. Andrews et al.