Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Microsoft word - estradiol nacda final.doc
Estradiol Salivary Estradiol Measurement in Wave I of the Social Life Health & Aging Project Authors: Karl Mendoza, BS, University of Chicago, Department of Ob/Gyn Mary Curran, Salimetrics LLC Stacy Tessler Lindau, MD, MAPP, University of Chicago, Departments of Ob/Gyn and Medicine – Geriatrics* * Corresponding author. Fax: +1 773 834 5664. E-mail address: slindau@uchicago.edu (S.T. Lindau). Suggested Citation: Mendoza, K., M. Curran, and S.T. Lindau. (2007). Salivary Estradiol Measurement in Wave I of the National Social Life, Health & Aging Project (NSHAP). Chicago Core on Biomarkers in Population-Based Aging Research http://biomarkers.uchicago.edu/pdfs/TR-Estradiol.pdf Date: December 17, 2007 Contents Rationale
Estradiol (17-beta-estradiol or E2), a steroid hormone derived from cholesterol, targets a variety of
tissues, located in the female and male reproductive tracts, mammary gland, and skeletal and cardiovascular systems (Hall, Couse et al. 2001). Among women, it is primarily synthesized from testosterone in the ovarian follicles, whereas among men, it is produced by the testes and extraglandular conversion of androgens (Tivis, Richardson et al. 2005; Salimetrics 2006).
In women, estradiol synthesis normally declines after menopause (Manly, Merchant et al. 2000; Meston and Frohlich 2000). This causes decreased vaginal lubrication and atrophy of the vaginal epithelium, due to diminished genital vasocongestion (Meston and Frohlich 2000). Though the
role of estrogens in female sexual desire is not fully understood, they may influence sexual desire (Dennerstein, Gotts et al. 1994; Meston and Frohlich 2000); estrogen replacement therapy may indirectly enhance female sexuality, by restoring vaginal lubrication (Meston and Frohlich 2000) or promoting positive body image and overall sense of well-being.
A number of studies have linked higher levels of serum estradiol to increased risk for developing breast cancer (Clemons and Goss 2001; Chlebowski, Hendrix et al. 2003; Tivis, Richardson et al. 2005) and coronary problems (Manson, Hsia et al. 2003; Tivis, Richardson et al. 2005). For women, higher estradiol levels have also been associated with improved cognition (Maki and Resnick 2000; Carlson, Zandi et al. 2001; Tivis, Richardson et al. 2005), mood, and memory (Tivis, Richardson et al. 2005). Estradiol’s effects on women’s skeletal health, however, are inconclusive.
For elderly men, estradiol may have a role, in combination with testosterone and other factors, in preservation of memory and cognitive function (Barrett-Connor, Goodman-Gruen et al. 1999; Carlson and Sherwin 2000).
Measurement
Sex hormone assays, particularly in the clinical setting, are typically performed on a serum specimen (Kaufman and Lamster 2002). Salivary measures have been developed and offer a relatively convenient and minimally-invasive approach for obtaining sex hormone data (Worthman, Stallings et al. 1990; Kaufman and Lamster 2002; Granger, Shirtcliff et al. 2004). These measures are representative of active, unbound steroid concentrations in the blood (Worthman, Stallings et al. 1990; Lu, Bentley et al. 1999). In the case of estradiol, good correlation between salivary and serum levels have been reported (Worthman, Stallings et al. 1990), including one study of people ages 18 to 28 (Shirtcliff, Granger et al. 2000) (n = 31) finding a correlation of r = 0.68 (p < 0.001), where a stronger, significant association was detected among women (n = 16, r = 0.60, p < 0.013) than men (n = 15, r = 0.60, p>0.05). Reported salivary concentrations, relative to free serum concentrations, have varied (Worthman, Stallings et al. 1990) from 0.2% to 7.90% (Lu, Bentley et al. 1999). In one study, salivary estradiol concentrations accounted for, on average, 1.65% of serum concentrations among men, and 3.33% among women (Shirtcliff, Granger et al. 2000). Among premenopausal women, salivary estradiol levels vary significantly across the menstrual cycle (Shirtcliff, Granger et al. 2000), with the lowest levels occurring during menstruation (Shirtcliff, Granger et al. 2000; Salimetrics 2006).
Population Norms
To our knowledge, population-based, published literature on salivary estradiol levels, particularly for postmenopausal women and older men, are limited. Table 1. Mean Serum and Salivary Estradiol Levels SALIVARY Age Range Perimenopausal women, mean age: 46.25 (SD = 2.63)
*Women who were undergoing estrogen therapy had a significantly higher serum estradiol level (p < 0.0001) [1] Shirtcliff et al. 2000 [2] Tivis et al. 2005 [3] Lasley et al. 2002 [4] Randolph et al. 2003
Specimen Collection
All respondents were asked to provide a salivary specimen; 90.8% (N=2,721) agreed, 2,640 respondents were able to provide a salivary specimen. This involved production of approximately 2 milliliters of saliva (unstimulated passive drool) into a small, code-labeled polypropylene collection vial via a 5-centimeter section of a household plastic straw, following procedures recommended by Salimetrics, LLC. The procedure required approximately 5 minutes. The time of last food or water consumption prior to saliva collection was recorded. Storage and Shipping
The salivary specimens were transported from the interview to a freezer using cold packs. Salivary specimens were stored in a freezer until they were shipped. The salivary samples were shipped to the lab on dry ice according to instructions. Upon receipt at Salimetrics, specimens were stored at -80°C in lab grade freezers.
Shipping Address 101 Innovation Blvd., Suite #302 (see Salimetrics Salivary Estradiol Enzyme Immunoassay Kit package insert for details http://salimetrics.com/pdf/HS%20Estradiol%20E2%20Kit%20Insert.pdf )
On day of assay, the specimens were thawed completely, vortexed, and centrifuged at 1500 x g (@3000 rpm) for 15 minutes. Clear samples were pipetted into wells. The enzyme immunoassay was conducted at Salimetrics, LLC. The assay range was > 1 pg/ml. Assays were conducted in the following priority order: 1) estrogen, 2) progesterone, 3) DHEA, 4) testosterone, 5) cotinine and underwent 2 to 3 freeze-thaw cycles:
thaw #1: sex hormone assays thaw #2: a subset underwent repeat sex hormone testing based on quality indicators thaw #3: cotinine assay
Table 2. NSHAP Salivary Testing Performed at Salimetrics detected Interference likely if Calibrator*Calibrator* sensitivity reported if * Calibrator values are used to adjust instrumentation by establishing the relationship (under specified conditions) between known, standard values and the values indicated by a particular measuring instrument. See package insert for calibration curve.Scoring
Values reported in picograms per milliliter (pg/mL). Assay range ≥ 1 pg/mL.
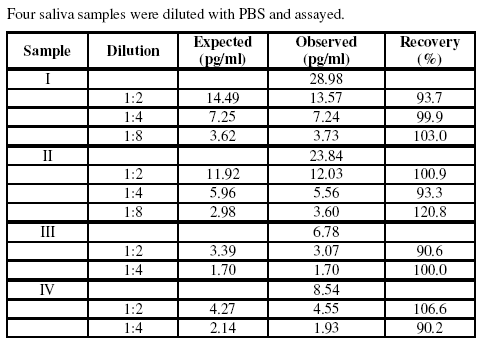
Performance Characteristics A. Precision Table 3. Reproduced with permission from Estradiol Quantitative Immunoassay Kit, 1-3702/1-3712, 96-Well Kit, April 10, 2006 (Salimetrics 2006)B. Sensitivity The lower limit of sensitivity was determined by interpolating the mean minus 2 SD’s of the optical densities of 10 sets of duplicates at the 0 pg/mL standard. The minimal concentration of estradiol that can be distinguished from 0 is less than 1.0 pg/mL. C. Correlation with Serum The correlation between saliva and serum estradiol in females was determined by assaying 11 matched samples. Samples were screened for pH and blood contamination. The magnitude of the saliva-serum correlation, r= 0.80, p <0.001, is consistent with the literature, in that the saliva- serum correlation is stronger among women, than men (Shirtcliff, Granger et al. 2000), and intra- subject correlation is higher, compared to between-subjects (Ellison and Lipson 1999). The conversion equation from salivary concentration to serum concentration for this particular estradiol assay is: Serum E2 (pg/mL) = 2.171*salivary E2 (pg/mL) +7.1846. D. Specificity of Antiserum Table 4. Reproduced with permission from Estradiol Quantitative Immunoassay Kit, 1-3702/1-3712, 96-Well Kit, April 10, 2006 (Salimetrics 2006)E. Recovery Table 5. Reproduced with permission from Estradiol Quantitative Immunoassay Kit, 1-3702/1-3712, 96-Well Kit, April 10, 2006 (Salimetrics 2006) F. Linearity of Dilution Table 6. Reproduced with permission from Estradiol Quantitative Immunoassay Kit, 1-3702/1-3712, 96-Well Kit, April 10, 2006 (Salimetrics 2006) Quality Control (see Table 2)
Run on each EIA test plate were six (6) standard calibrators ranging from 2 pg/mL to 64 pg/mL and two sets of high and low controls. The control ranges were established using a minimum of 10 sets of data points across 10 plates. The mean and standard deviations were calculated and a range was established (mean +/- 2 S.D.). A sufficient number of assay kits and controls were sequestered for the project to minimize any lot-to-lot variations over the course of the study. Subjects’ saliva samples were run in duplicate (saliva pipetted into side-by-side wells) on a single EIA plate. Assay results for each subject were acceptable when the values: 1.) fell within the range of the calibrators (2 pg/mL - 64 pg/mL) , 2.) were >1 pg/mL, and 3.) the coefficient of variation (%CV) between the duplicate results (result 1 and result 2) was <15%. In instances where the %CV between duplicates was >15%, results were accepted if the absolute value between result 1 and result 2 was <2 pg/mL. Values greater than the upper
assay limit of 64 pg/mL were run on dilution to bring the OD readings within acceptable range (2 pg/mL - 64 pg/mL). In instances when a sample returned an extremely high result, dilutions were made up to 320 pg/mL and a flag (**) and comment “interference likely” were added to the report. Samples with results < 1pg/mL were also repeated. Values falling between 0.5 pg/mL and 1 pg/mL were reported and flagged (*) with the comment “below lower limit of assay”. Estradiol values less than 0.5 pg/mL were reported as “none detected”. Estradiol data were compiled in ExcelTM by the testing manager and checked for accuracy by the technical supervisor before final reports were emailed. Data was supplied with corresponding assay plate number to facilitate the calculation of intra-assay and inter-assay control values. Availability
Product Name
High Sensitivity Salivary Estradiol Enzyme Immunoassay Kit
Manufacturer Location of Manufacturer
State College, PA 16803 USA 800-790-2258 (USA & Canada only)
Catalog No. References
Barrett-Connor, E., D. Goodman-Gruen, et al. (1999). "Endogenous sex hormones and cognitive
function in older men." J Clin Endocrinol Metab 84(10): 3681-5.
Carlson, L. E. and B. B. Sherwin (2000). "Higher levels of plasma estradiol and testosterone in
healthy elderly men compared with age-matched women may protect aspects of explicit memory." Menopause 7(3): 168-77.
Carlson, M. C., P. P. Zandi, et al. (2001). "Hormone replacement therapy and reduced cognitive
decline in older women: the Cache County Study." Neurology 57(12): 2210-6.
Chlebowski, R. T., S. L. Hendrix, et al. (2003). "Influence of estrogen plus progestin on breast
cancer and mammography in healthy postmenopausal women: the Women's Health Initiative Randomized Trial." Jama 289(24): 3243-53.
Clemons, M. and P. Goss (2001). "Estrogen and the risk of breast cancer." N Engl J Med 344(4):
Dennerstein, L., G. Gotts, et al. (1994). "The relationship between the menstrual cycle and female
sexual interest in women with PMS complaints and volunteers." Psychoneuroendocrinology 19(3): 293-304.
Ellison, P. T. and S. F. Lipson (1999). "Salivary estradiol--a viable alternative?" Fertil Steril 72(5):
Granger, D. A., E. A. Shirtcliff, et al. (2004). "The "trouble" with salivary testosterone."
Psychoneuroendocrinology 29(10): 1229-40.
Hall, J. M., J. F. Couse, et al. (2001). "The multifaceted mechanisms of estradiol and estrogen
receptor signaling." J Biol Chem 276(40): 36869-72.
Kaufman, E. and I. B. Lamster (2002). "The diagnostic applications of saliva--a review." Crit Rev
Oral Biol Med 13(2): 197-212.
Lasley BL, Santoro N, Randolf JF, Gold EB, Crawford S, Weiss G, et al. The relationship of
circulating dehydroepiandrosterone, testosterone, and estradiol to stages of the menopausal transition and ethnicity. Journal of Clinical Endocrinology & Metabolism 2002;87(8):3760-7.
Lu, Y., G. R. Bentley, et al. (1999). "Salivary estradiol and progesterone levels in conception and
nonconception cycles in women: evaluation of a new assay for salivary estradiol." Fertil Steril 71(5): 863-8.
Maki, P. M. and S. M. Resnick (2000). "Longitudinal effects of estrogen replacement therapy on
PET cerebral blood flow and cognition." Neurobiol Aging 21(2): 373-83.
Manly, J. J., C. A. Merchant, et al. (2000). "Endogenous estrogen levels and Alzheimer's disease
among postmenopausal women." Neurology 54(4): 833-7.
Manson, J. E., J. Hsia, et al. (2003). "Estrogen plus progestin and the risk of coronary heart
disease." N Engl J Med 349(6): 523-34.
Meston, C. M. and P. F. Frohlich (2000). "The neurobiology of sexual function." Arch Gen
Psychiatry 57(11): 1012-30.
Randolph, J. F., Jr., M. Sowers, et al. (2003). "Reproductive hormones in the early menopausal
transition: relationship to ethnicity, body size, and menopausal status." Journal of Clinical Endocrinology & Metabolism 88(4): 1516-22.
Salimetrics (2006). High Sensitivity Salivary Estradiol Enzyme Immunoassay Kit. State College,
PA, Salimetrics LLC: 3.
Salimetrics (2006). Salivary Testosterone Enzyme Immunoassay Kit. Shirtcliff, E. A., D. A. Granger, et al. (2000). "Assessing estradiol in biobehavioral studies using
saliva and blood spots: simple radioimmunoassay protocols, reliability, and comparative validity." Horm Behav 38(2): 137-47.
Tivis, L. J., M. D. Richardson, et al. (2005). "Saliva versus serum estradiol: implications for
research studies using postmenopausal women." Prog Neuropsychopharmacol Biol Psychiatry 29(5): 727-32.
Worthman, C. M., J. F. Stallings, et al. (1990). "Sensitive salivary estradiol assay for monitoring
ovarian function." Clin Chem 36(10): 1769-73.
Las elecciones en Colombia: una perspectiva europea (Elections in Colombia: a European perspective) Afligidos por una profunda crisis financiera, los gobiernos europeos difícilmente se atreven a levantar la vista de sus propias cuentas públicas. Las tijeras de Italia y España ya han cortado los recursos dedicados a la ayuda para el desarrollo. La voz europea en los grandes asunto
Early Release TABLE 2. Drug therapy for treatment and chronic maintenance therapy of AIDS-associated opportunistic infections in adults and adolescents Preferred therapy, duration of therapy, Opportunistic infection chronic maintenance Alternative therapy Other options/issues Preferred treatment for moderate to severe Alternative therapy for moderate to severe Indica
 Estradiol
Estradiol 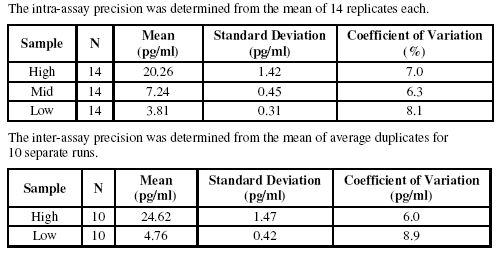 Table 2. NSHAP Salivary Testing Performed at Salimetrics
Table 2. NSHAP Salivary Testing Performed at Salimetrics 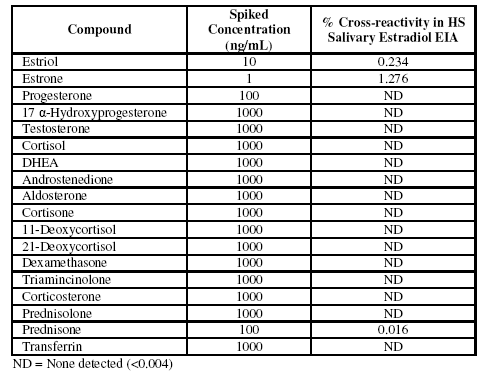 B. Sensitivity
B. Sensitivity 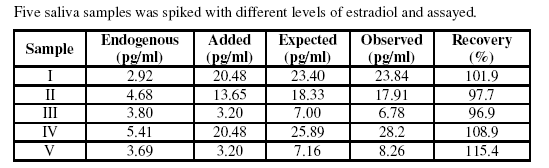
 E. Recovery
E. Recovery