Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Pii: s0190-9622(99)70006-x
Changes in hair weight and hair count in men with androgenetic alopecia, after application of 5% and 2% topical minoxidil, placebo, or no treatment
Vera H. Price, MD,a Emory Menefee, PhD,b and Paul C. Strauss, MDc
San Francisco and Richmond, California, and Kalamazoo, Michigan
Quantitative estimation of hair growth using hair weight and number was recorded for 120 weeks in 4groups of 9 men with androgenetic alopecia. Three double-blind groups applied either 2% or 5% minoxidilsolution, or vehicle. The fourth group, unblinded, received no treatment. Measurements of hair weight andnumber were continued for 96 weeks, when treatment (if any) was stopped, though measurements werecontinued for another 24 weeks. Although not compared statistically, the placebo and untreated groupsbehaved in a similar fashion. In contrast, the 5% and 2% minoxidil treatment groups showed a statisticallysignificant increase in mean percentage change in interval weight from baseline compared with placebo;results for number counts were usually less significant. Over 96 weeks, topical minoxidil induced andmaintained an increase in interval weight over baseline of about 30%. After treatment was stopped, hairweight and number counts for the minoxidil groups returned to about the same levels as placebo in 24weeks. (J Am Acad Dermatol 1999;41:717-21.)
We previously recommended total hair surements were continued for 24 additional weeks.
weight from a defined scalp area as the pri-
Concurrently, a group of men with androgenetic
mary estimator for hair growth.1 The effi-
alopecia received no treatment and their hair growth
cacy of a hair growth–promoting agent can be estab-
was compared with the treated groups over the
lished in 24 weeks by comparing the total hair
same 120-week period (this group was perforce not
weight of hair grown in a small, carefully maintained
part of the blinded study). A preliminary account of
area on the scalp in subjects given either a hair
part of this study was previously published in con-
growth promoter or a placebo. We now extend the
method to longer times, more subjects, and a widerrange of treatments. In this study, quantitative esti-
mation of hair growth was recorded for 120 weeks
Subject selection
for a group of men with androgenetic alopecia. Our
Eligible subjects for this study were 18- to 40-year-old
purpose was to compare the effect of 5% and 2%
men with androgenetic alopecia as evidenced by
topical minoxidil solution and placebo, in a random,
frontal/parietal thinning defined by the Hamilton Scale as
double-blind protocol, on both hair growth promo-
type III or IV. They had to be in good health and have dark,
tion and retardation of the hair loss process, using
undyed hair, with no gray or white hair. Exclusion criteria
total hair weights and counts. After 96 weeks, treat-
included use of topical minoxidil within the previous 6
ment was stopped, although the hair growth mea-
months; use of any investigational drug within the previous6 months; concomitant use of steroids, vasodilators, antihy-pertensives, calcium channel blockers, antiepileptic drugs,
From the Department of Dermatology, University of California, San
cytotoxic agents, “hair restorers,” or other medications that
Franciscoa; Trichos Research, Richmondb; and Pharmacia &
could influence hair growth; or prior participation in a top-
ical minoxidil study. Pre-enrollment laboratory studies
Supported by a grant from Pharmacia & Upjohn.
included a complete blood cell count with differential, uri-
Accepted for publication June 24, 1999.
nalysis with microscopic examination, liver function tests,
Reprint requests: Vera H. Price, MD, Department of Dermatology,
University of California, San Francisco, 350 Parnassus Ave, Suite
and determination of levels of lactic dehydrogenase, calci-
um, phosphorus, creatinine, uric acid, blood urea nitrogen,
Copyright 1999 by the American Academy of Dermatology, Inc.
serum electrolytes, thyroxine, and thyroid-stimulating hor-
16/1/100949
mone. These studies, as well as an electrocardiogram, and
718 Price, Menefee, and Strauss
fully hand clipped and collected under magnification inthe manner previously described.1
Measurement method
Hair samples were degreased in trichlorotrifluo-
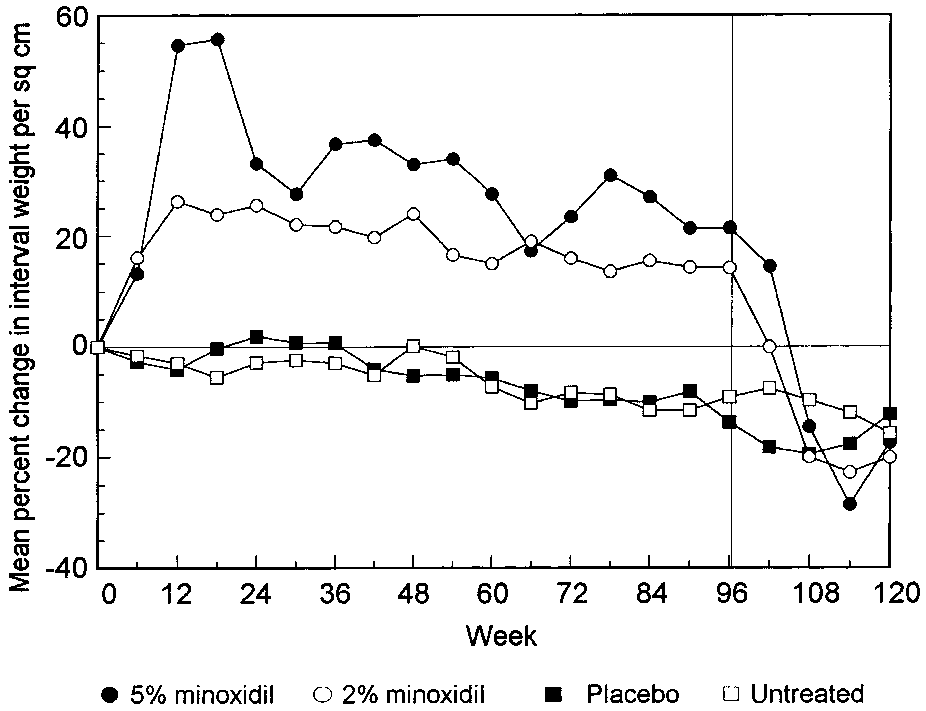
roethane (Freon TF) and dried. The total hair sample wasspread out on a grid and counted. The hair sample wasthen placed in the chamber of an analytical balance having0.01 mg readability. After conditioning for at least 1 hour inthe balance chamber, the ambient relative humidity wasrecorded, and the samples weighed. Sample weights werecorrected to a standard humidity of 65%.1 Weightsobtained by this method are termed interval weights todistinguish them from total (cumulative) weights. They areequivalent to growth rates (weight produced per 6-weekinterval). Fig 1. Comparison of mean percentage change in interval Protocol
weight per square centimeter for 4 treatment groups: 5%
Following their hair clipping on the second visit, 27
minoxidil, 2% minoxidil, placebo, and untreated. Vertical
subjects were assigned test solutions that were a solution
line at 96 weeks marks cessation of treatment.
of either 2% minoxidil (in a vehicle of 20% vol/vol propyl-ene glycol, 60% ethanol, and water) or 5% minoxidil (in avehicle of 50% vol/vol propylene glycol, 30% ethanol, and
chest x-ray if not taken in the prior 6 months, all had to have
water), or the 5% vehicle solution referred to as placebo.
normal results or findings to qualify for eligibility in the
The subjects were assigned the test solutions in a ran-
study. Thirty-six men 24 to 40 years of age qualified for the
domized, double-blind manner as follows: 9 men received
study and signed an informed consent.
5% topical minoxidil solution, 8 men received 2% topicalminoxidil solution, and 10 men received placebo. They
Scalp site selection and sampling frequency
were instructed to apply 1 mL of the assigned solutions
A representative site was selected on the thinning
with a metered dropper twice daily to the frontal/parietal
frontal/parietal scalp. Hair in the designated area was care-
scalp, beginning at the clipped site. Applications were
fully hand clipped under magnification on the screening
made with the scalp dry, spread with one fingertip, and
visit (designated as week –6) and at 6-week intervals there-
then allowed to dry without a hair dryer. After 96 weeks,
after, for a total of 120 weeks. No treatment was given dur-
treatment was stopped and the hair growth measurements
ing the first 6 weeks, so that the sample collected at the
were continued for 24 additional weeks. Nine additional
end of this interval represented baseline growth (week 0).
men with similar scalp hair thinning were followed up con-
For the men assigned to one of the treated groups, treat-
currently without treatment for 120 weeks.
ment was started on the second visit (week 0) and contin-
All 36 subjects were well matched in age, duration and
ued for 96 weeks. After 96 weeks, treatment was stopped
extent of alopecia, and original target area hair density. To
and hair clippings were continued at 6-week intervals for
avoid accidental hair cutting in the test site, hair cuts for
24 additional weeks. Concurrently, the group of untreated
the purpose of hair styling were permissible only during
men had their hair clipped with the same method every 6
the 7 days after a clipping procedure.
During the study, vital signs, medical events, and skin
tolerance were monitored, and serum minoxidil levels,
Marking and clipping procedure
hematology, and blood chemistries were measured.
During the screening (week –6) clipping, a template
consisting of a plastic sheet with a square hole (1.34 cm2)was placed over the selected site. All hairs within the tem-
plate square were pulled through it, with the help of a
Thirty-three subjects completed the first 96 weeks
magnifying lamp to ensure that only hair originating with-
and 32 subjects the entire 120-week study. One
in the square was included. The hairs were grasped and
untreated subject withdrew at week 6, two treated
hand clipped to about l mm in length with small straight
subjects (assigned to 2% minoxidil solution and
surgical scissors. Four small dots were then placed in the
placebo) withdrew at week 48 because of scheduling
corners of the square with a fine ballpoint pen. After the
problems, and one treated subject (assigned to 2%
template was removed, the 4 corners were permanently
minoxidil solution) dropped out at week 96 because
marked using ink and the Spalding and Rodgers marking
he did not wish to stop treatment. Occasionally, a
On subsequent visits at 6-week intervals, the plastic
subject was unable to appear on the exact scheduled
template was laid in exact correspondence with the per-
date for clipping. To facilitate statistical analysis, the
manent markings, and the hair in the marked square care-
measured weight from these erratic intervals was
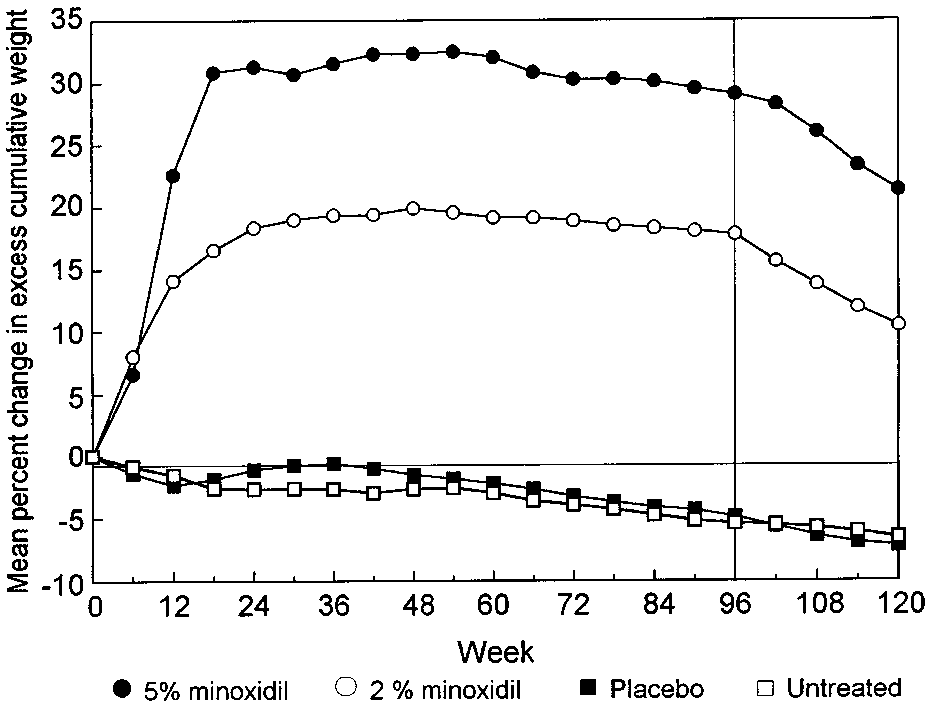
Price, Menefee, and Strauss 719 Fig 2. Comparison of mean percentage change in num- Fig 3. Comparison of the mean percentage change in
ber per square centimeter for 4 treatment groups: 5%
excess cumulative weight for 4 treatment groups: 5%
minoxidil, 2% minoxidil, placebo, and untreated. Vertical
minoxidil, 2% minoxidil, placebo, and untreated. Vertical
line at 96 weeks marks cessation of treatment.
line at 96 weeks marks cessation of treatment.
adjusted by a multiplying factor of 42/D, where D is
Another representation, which we have called
the actual number of days in the interval. This adjust-
excess cumulative weight, has been found to be use-
ment assumes that the growth rate remains constant
ful for discriminating among different treatments. It
during the short period needing correction. Interval
is defined as the difference between the actual
weights used in this article have been adjusted by
cumulative mean weight and the hypothetical cumu-
this method when necessary. No correction was
lative weight that would accrue if growth continued
made to number counts from subjects who did not
at the same rate as during the baseline pretreatment
return at an exact 6-week interval. The numbers of
period (from week –6 to week 0). Thus excess cumu-
subjects in the calculation groups were as follows: 7
lative weight represents the aggregate change in
subjects in the 2% group (6 after week 96), 9 subjects
weight, if any, caused by treatment. Expressed differ-
in the 5% group, 9 subjects in the placebo group,
ently, the excess cumulative weight reflects the total
and 8 subjects in the untreated group.
cumulative hair protein production induced by treat-
Results of the measurements of interval weights
ment. In number counts, the equivalent of a cumu-
and number counts are summarized in Figs 1 and 2,
lative function is simply the baseline value subtract-
respectively. Each point on these figures represents
ed from the count at a particular time. The mean
the mean percentage change from baseline of all
percent change in excess cumulative weight is illus-
subjects in the designated group (2% and 5% minox-
trated in Fig 3 for the 4 treatment groups.
idil treatments, placebo, and untreated). Treatment,if any, was stopped at week 96 (indicated in the fig-
DISCUSSION
ures by a vertical line). Percentage changes are plot-
For statistical comparison, the 3 treatments were
ted rather than the primary measurements of inter-
considered as a group, and a one-sided analysis of
val weight and number count to remove baseline
variance test was used to determine whether there is
variation and more accurately isolate effects caused
significant difference among any of the 3 treatments
by treatment. The primary measurements are not
(overall P value < .05). In this test, it was found that
useful for statistical comparison owing to differences
all trials up to week 96 showed significant differences
in their baseline values at week 0. Over all subjects,
for 2 of the 3 measurement variables: mean percent-
baseline interval weights ranged from 2.9 to 15.0
age weight change and mean percentage change in
mg/cm2, with a standard deviation of 40% and base-
excess cumulative weight. However, for mean per-
line number counts ranged from 79 to 251 per
centage number change, about one third of the trials
square centimeter, with a standard deviation of 21%.
showed no significant difference among the 3 treat-
This variability is a reflection of the wide range of
ment groups (5% and 2% minoxidil, and placebo);
normal growth among a sampling of subjects and is
these trials are shown as italicized numbers in Table
approximately maintained throughout subsequent
I. We interpret this decreased significance in mean
percentage number change (as contrasted with the
720 Price, Menefee, and Strauss Table I. P values from Fisher least significant difference comparisons of 2%-5% (2-5), 2%-placebo (2-P), and 5%- placebo (5-P)* Mean percentage Mean percentage Mean percentage weight change number change excess cumulative weight change
*0 represents P < .0005; (P > .05), nonsignificant. Analysis of variance intergroup tests are italicized.
weight variables) to the large fluctuation in the num-
Mean percentage changes in interval weights
ber of small hairs during the growth changes
from baseline are shown in Fig 1. The placebo and
induced by minoxidil. The effect of small hairs is not
untreated groups appear to behave similarly, show-
as pronounced in weight measurements. This pro-
ing a steady decrease in hair weight from baseline
vides confirmation of our suggestion that weight
over the 120 weeks. This decrease can be taken as
measurements offer a more reliable estimation of
the “normal” hair loss for this group of subjects with
androgenetic alopecia and amounts to about a 6%
The Fisher least significant difference test was
decrease in weight per year. The 2% and 5% minoxi-
used to determine which of the 3 treatment groups
dil groups appear to decrease with nearly the same
show significantly different means. P values from this
average downward slope, once the peak rate of
growth has been passed. The treatments appear to
For the two weight variables (mean percentage
induce a consistent increased growth offset (above
weight change and mean percentage excess cumula-
placebo or untreated groups) of roughly 25% for the
tive weight change), differences between either the
2% minoxidil treatment and 35% for the 5% minoxi-
2% and 5% treatment levels and placebo were gen-
dil treatment, an average increase of about 30%,
erally significant (P ≤ .05) after only 6 weeks of treat-
maintained during the 96 weeks of treatment. These
ment. The incremental increase in hair growth over
growth offsets represent a long-term retardation of
placebo seen after week 6 was maintained through
the hair loss process by both 5% and 2% topical
the 96 weeks of treatment for both the weight vari-
ables. Comparison of the 2% minoxidil treatment
Mean percentage changes in number counts from
with placebo was not generally significant for the
baseline are shown in Fig 2. Despite what appears as
mean percentage change in number counts; howev-
a somewhat erratic response, the fluctuations in
er, the 5% minoxidil treatment showed a consider-
number counts for 5% and 2% minoxidil (apparently
ably greater significant difference in number counts
greater than those for weights) reflect a distinct
over placebo, though not at all treatment times.
series of events that occur after the onset of treat-
Differences between the 2% and 5% treatments
ment. We hypothesize that the first stage of regrowth
themselves were not statistically significant for
appears to involve enlargement of a number of
weight changes or number change (P > .05), though
miniaturized hairs, which also have shortened
a difference appears visually apparent in Figs 1-3.
growth cycles, as well as the probable nudging of
Price, Menefee, and Strauss 721
many older anagen hairs into telogen. Hence the
paring Fig 3 with Figs 1 and 2, but also from the sta-
first indication of treatment efficacy is a large
tistical comparisons in Table I, where P values reach
increase in total hair count within 12 weeks. This
lower levels at earlier treatment times for excess
spurt is particularly evident with 5% minoxidil, an
cumulative weight changes than for either weight or
effect seen with both interval weights and number
number count changes. This sharper discrimination
counts. Because the cycles are mostly still short,
makes the excess cumulative weight useful for rapid
these “new” anagen hairs enter telogen and fall out
quickly, to be replaced with another wave of hairs
After treatment was stopped at week 96, the 5%
that have somewhat longer growth cycles. This
and 2% minoxidil groups showed a rapid loss of hair
process repeats, and no strong decline seems evi-
weight and decreased hair counts. Vertical lines
dent through 96 weeks, although the long-term
drawn at week 96 in Figs 1-3 indicate when treat-
number counts should eventually decrease. A “place-
ment was stopped. By 24 weeks after treatment had
bo effect” appears to occur more markedly for num-
been stopped, the weight and number counts of the
ber counts than for weights, for reasons at present
treated groups decreased to become similar to those
of the placebo and untreated groups, showing the
If we can ignore the fluctuations, the changes in
growth offset produced by topical minoxidil. This
number counts from baseline of the treated sub-
loss of treatment-stimulated hair growth is expected
jects generally parallel the changes in weight. We
since treatment does not alter the underlying genet-
believe that the weight measurements have more
ic predisposition for androgenetic alopecia.
reliability than number counts when assessing hair
This study demonstrates that 5% and 2% topical
growth, at least in terms of increased hair protein
minoxidil promote hair growth and retard the hair
production. Counts of the smallest hairs are subject
loss process over 96 weeks, with 5% topical minoxi-
to unavoidable uncertainty, though they contribute
dil having the greater efficacy. Although the interval
little to the total hair weight. Furthermore, fluctua-
hair weight eventually began to decrease with time,
tions in numbers of small anagen hairs with short
the minoxidil treatment maintained an increased
growth cycles are not as strongly reflected in the
rate of hair weight (protein) production, over that of
placebo or untreated subjects, of about 25% more
Excess cumulative weight is shown in Fig 3, as
for the 2% minoxidil treatment and about 35% more
percentage change from the extrapolated baseline
for the 5% minoxidil treatment and averaging about
cumulative weight. Fluctuation appears smaller than
30% during the 96-week treatment period.
that of the interval weight, a characteristic of cumu-lative functions. Because earlier interval weight data
We thank The Upjohn Company for continued support.
are carried along in the excess weight function,
We are grateful to Cathy Kavanagh, Andrea Menefee, and
changes or fluctuations in later interval weights tend
Leta Regezi for technical assistance.
to be somewhat masked. This behavior is also appar-ent when treatment is stopped at 96 weeks. The
REFERENCES
1. Price VH, Menefee E. Quantitative estimation of hair growth. I.
excess cumulative weight decreases more gradually
Androgenetic alopecia in women: effect of minoxidil. J Invest
during the 24 weeks after stopping of treatment than
do either the weights or numbers in Figs 1 and 2.
2. Price VH, Menefee E. Quantitative estimation of hair growth:
For discriminating among different treatments,
comparative changes in weight and hair count with 5% and 2%
especially at early times, the excess cumulative
minoxidil, placebo and no treatment. In: Van Neste D, RandallVA, editors. Hair research for the next millenium. Amsterdam:
weight seems to offer a clearer separation of treat-
ment effects than either interval weights or numbercounts. This is apparent not only from visually com-
Neue Vorträge in der Praxis Auch in diesem Herbst wollen wir wieder in einer kleinen Vortragsreihe zur gemeinsamen Diskussion einladen. Drei Termine sind dafür vorgesehen. Wieder am Donnerstag, von 18.00 bis 19.00 in unserem Wartezimmer . Melden Sie sich bitte an. 16. November Sparen am rechten Platz Darf man bei Medikamenten sparen? Und wenn ja, geht das ohne auf Qualitä
R E D U C I N G S E R U M I N S U L I N A N D OVA R I A N CY TO C H RO M E P 4 5 0 c 1 7 a I N P O LYCYST I C OVA RY SY N D RO M E DECREASES IN OVARIAN CYTOCHROME P450c17 a ACTIVITY AND SERUM FREE TESTOSTERONE AFTER REDUCTION OF INSULIN SECRETION IN POLYCYSTIC
 718 Price, Menefee, and Strauss
718 Price, Menefee, and Strauss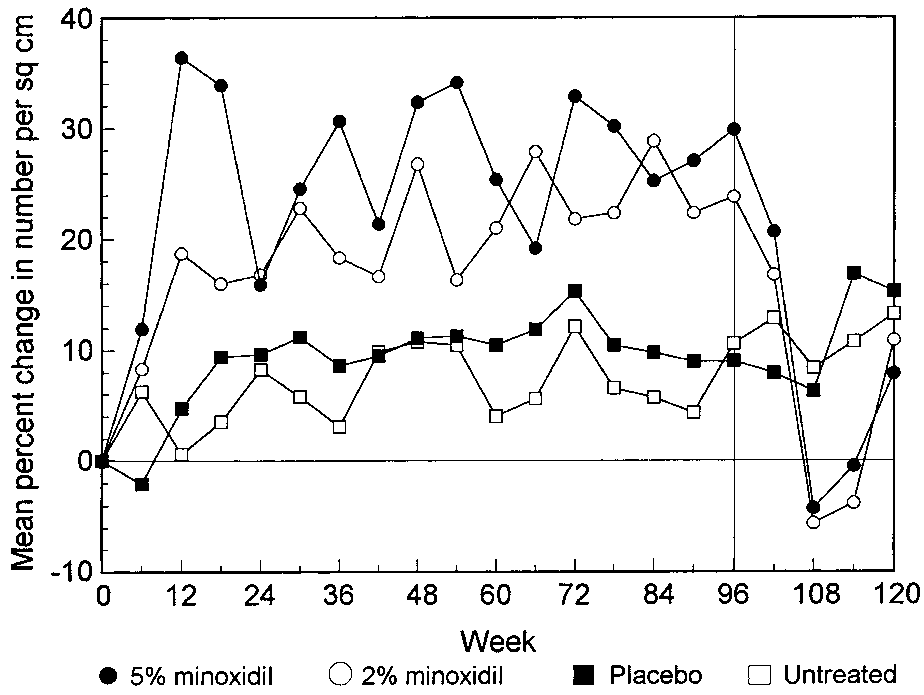
 Price, Menefee, and Strauss 719
Price, Menefee, and Strauss 719