Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Untitled
Annals of Oncology Advance Access published February 13, 2013
Multicentre phase II study of cisplatin–etoposidechemotherapy for advanced large-cell neuroendocrinelung carcinoma: the GFPC 0302 study
J. Le Treut1, M. C. Sault2, H. Lena3, P. J. Souquet4, A. Vergnenegre5, H. Le Caer6, H. Berard7,S. Boffa8, I. Monnet9, D. Damotte10 & C. Chouaid111Department of Pneumology, Aix en Provence; 2Department of anatomopathology, Aix en Provence; 3Department of Pneumology, Rennes; 4Department of Pneumology,Lyon; 5Department of Pneumology, Limoges; 6Department of Pneumology, Draguignan; 7Department of Pneumology, Toulon; 8Department of Pneumology, Rouen;9Department of Pneumology, Créteil; 10Department of anatomopathology, Hôtel Dieu; 11Department of Pneumology, Hôpital Saint Antoine, Paris, France
Received 28 October 2012; revised 18 December 2012; accepted 19 December 2012
Background: The optimal treatment of large-cell neuroendocrine carcinoma (LCNEC) of the lung remains unclear.
Here, our primary objective was to assess the efficacy of cisplatin–etoposide doublet chemotherapy in advancedLCNEC. Accuracy of the pathological diagnosis and treatment toxicity were assessed as secondary objectives. Patients and methods: Prospective, multicentre, single-arm, phase II study with a centralised review of treatment-
response and pathological data. Patients had untreated performance status (PS) 0/1 stage IV/IIIB LCNEC and received
cisplatin (80 mg/m22 d1) and etoposide (100 mg/m22 d1-3) every 21 days. Results: Eighteen centres included 42 patients (mean age, 59 ± 9 years; 69% men; median of four cycles/patient). At
least one grade-3/4 toxicity occurred in 59% of patients (neutropaenia, thrombocytopaenia, and anaemia in 32%, 17%,
and 12%, respectively). The median progression-free survival (PFS) and overall survival (OS) were 5.2 months (95%
confidence interval, CI, 3.1–6.6) and 7.7 months (95% CI, 6.0–9.6), respectively. The centralised pathologist reviewreclassified 11 of 40 (27.5%) patients: 9 as small-cell lung cancer, 1 as undifferentiated non-small-cell lung cancer, and
1 as atypical carcinoid. Survival data were not significantly changed by excluding the reclassified patients.
Conclusions: The pathological diagnosis of LCNEC is difficult. The outcomes of advanced LCNEC treated withcisplatin–etoposide doublets are poor, similar to those of patients with advanced small-cell lung carcinoma (SCLC). Key words: carcinoma, clinical trial phase II, large cell neuroendocrine tumours, small-cell lung cancer
extensive necrosis seen in LCNEC and SCLC are in contrast to
Large-cell neuroendocrine carcinoma (LCNEC) of the lung
the lower-grade neuroendocrine tumours, i.e. typical and
accounts for no more than 1% of all lung cancers. The typical
atypical carcinoids. LCNEC and SCLC also share clinical
histological features, first described in 1991 , ], include large
characteristics including a preponderance of males and
cells with abundant cytoplasm, a high mitotic rate, extensive
smokers and an aggressive clinical course [–]. The clinical
necrosis, and a neuroendocrine growth pattern. The World
outcome of LCNEC patients is poor, with overall 5-year
Health Organisation currently classifies LCNEC as a distinct
survival rates ranging from 15% to 57%. Studies have
subtype of pulmonary large-cell carcinoma [] and, therefore,
demonstrated significantly worse survival in LCNEC compared
as a subtype of non-small-cell lung carcinoma (NSCLC).
with other non-small-cell carcinomas but not compared with
However, LCNEC lacks the specific histologic features of
NSCLC such as glandular or squamous differentiation, but
In terms of treatment, several recent studies have shown that
instead displays evidence of neuroendocrine differentiation
LCNEC responds to cisplatin-based chemotherapeutic
reminiscent of small-cell lung carcinoma (SCLC), although the
regimens similar to those used for SCLC ]. However, these
malignant cells in SCLC are smaller, with scant cytoplasm, and
are retrospective studies in small numbers of patients
invade the tissues in sheets. LCNECLCNEC shares genetic
and consequently the sensitivity of LCNEC to the
alterations with SCLC [The higher mitotic rates and more
chemotherapeutic regimens commonly used for SCLC remainsunclear ].
Here, our primary objective was to assess the efficacy of
*Correspondence to: Prof. C. Chouaid, Department of Pneumology, Centre Hospialier
de Creteil, 40 avenue de Verdun, 94010 Créteil, France. Tel: +33-157022070;
–etoposide doublet chemotherapy in patients with
Fax: +33-157022059; E-mail: christos.chouaid@chicreteil.fr
advanced LCNEC. Secondary objectives were to assess the
The Author 2013. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
accuracy of the pathologic diagnosis of LCNEC and to evaluate
toxicity was classified as treatment failure. We also computed the objective
the toxic effects of cisplatin–etoposide doublet chemotherapy.
response rate as the number of responders over the number of patients whocould be evaluated at the sixth cycle. Finally, we computed the objectiveresponse rate based on the best radiological response observed during the
six cycles. For all response rates, the 95% confidence intervals (95% CIs)
This prospective, multicentre, single-arm, phase II trial was approved by
the appropriate ethics committee (Marseille 2, Number 03/71). A written
Progression-free survival (PFS) and overall survival (OS) were estimated
informed consent was obtained from each patient before study inclusion.
using the Kaplan–Meier method from baseline to the date of radiological
The study patients were recruited at 18 study centres in France between
progression or death for PFS, date for death for OS. For patients alive at
May 2004 and December 2009. Patients were eligible if they had
last follow-up, the data were censored at the last follow-up visit. The
histologically documented LCNEC meeting criteria for stage IV disease or
median follow-up was estimated using the inverse Kaplan–Meier method.
for stage IIIB disease with pleural involvement. Pathological definition of
The analysis was based on a data cut-off date of April 2012.
LCNEC was as previously described [] cohesive sheet of large tumouralcells with an endocrine pattern, often one or several nucleoli andexpression of at least two out of the three neuroendocrine markers; CD56,
synaptophysin and chromogranin.The other inclusion criteria were as
The 18 study centres enrolled 42 patients during the study
follows: performance status (PS) 0/1; age 18–75 years; no previous
period. The mean age was 59 ± 9 years (range 33–73 years) and
chemotherapy; measurable target in a non-irradiated region; absence of
29 (69%) patients were men (Table The mean time from
peripheral neuropathy grade 2 or higher; life expectancy more than
diagnosis to study inclusion was 0.9 ± 1.2 months.
3 months, and biological status compatible with chemotherapy (bilirubin<1.25 ULN, transaminase activity <3 ULN, alkaline phosphatase
Tumour stage was IV in 88% of patients (Table The
<2.5 ULN, polymorphonuclear neutrophil count >1.5 G/l, and platelet
centralised pathology review was possible for 40 (95%) patients
count >100 G/l). Patients with a history of palliative radiation therapy
and led to the reclassification of 11 (27.5%) patients into the
could be included. We did not include patients with mixed histological
following diagnostic categories: SCLC, n = 9; undifferentiated
features or a diagnosis of LCNEC established only by cytological
NSCLC, n = 1; and atypical carcinoid, n = 1.
examination. The other no inclusion criteria were histological status
In the intention-to-treat analysis of the overall population,
(small-cell lung cancer, bronchioloalveolar carcinoma), prior
stabilisation occurred in 26% of patients, a partial response in
chemotherapy, symptomatic brain metastases, unstable heart disease,
38%; the study meet is the primary end point with a 64%
uncontrolled infection, grade >2 neuropathy and a history of metastatic
disease control rate. When we confined the analysis to the 29
patients in whom the diagnosis of LCNEC was confirmed by
Chemotherapy consisted of cisplatin, 80 mg/m2, as a 30-min intravenous
the centralised pathology review, the rates of stabilisation,
infusion on day 1 (D1) and etoposide, 100 mg/m2 on D1, D2, and D3. This
partial response, and disease progression were 31%, 34%, and
combination was given at 21-day intervals, up to six times. Growth-factor
35%, respectively; these proportions were not significantly
therapy was at the discretion of the investigator in charge of patient care. A
different from those in the overall population (P = 0.18).
clinical evaluation and laboratory tests were carried out at the beginning of
The median follow-up was 37.2 months. The median PFS in
the overall population was 5.2 months (95% CI, 3.1–6.6
The primary end point was the objective response rate. Responses were
months) and the median OS was 7.7 months (95% CI, 6.0–9.6
evaluated based on Response Evaluation Criteria in Solid Tumours (version
months) as shown by Figure . After 1 year, the PFS rate was
1.0), after three and six treatment cycles. Computed tomography or
14.3% (95% CI, 6.7–27.8) and the OS rate was 26.8% (95% CI,
magnetic resonance imaging was used for radiologically measurable
15.7–41.9). In the analysis confined to the patients with
tumours. All imaging studies and TNM classifications were subjected to a
confirmed LCNEC, the median PFS was 5.0 months (95% CI,
centralised review. A panel of six pathologists carried out a centralisedreview of all histological specimens; they worked, independently withdifferences resolved by consensus; patients who were reclassified as havingtumours other than LCNEC continued their participation in the study.
Table 1. Main characteristics of the 42 study patients
Toxic effects were recorded and graded according to the National CancerInstitute Common Toxicity Criteria (AE version 3.0).
In this exploratory open phase II study, the hypothesis was to reject platin
doublet if the disease control rate (RR) was lower than 30% and retain this
doublet for an RR higher than 50% (risk alpha 5%, statistical power 80%);
two analysis were planned after 20 and after 35 inclusions and the protocol
had to be stopped for futility if there were respectively less than three and
less than six patients with disease control; the planned number of patients
Quantitative data were described as median and range and qualitative
Cisplatin–etoposide chemotherapy given, n
data as percentage. Groups were compared using the chi-square test.
Efficacy was assessed per patient. The objective response rate was
computed in the intention-to-treat population as the number of responders
over the total number of study patients. Treatment discontinuation due to
Table 2. Toxicity rates seen in over 10% of the patients and rates of grade-3/4 toxic effects
Figure 1. Progression-free survival (PFS) and overall survival (OS) in the
In this prospective, multicentre study of patients with advancedLCNEC, cisplatin–etoposide doublet chemotherapy provided
median PFS and OS durations of 5.2 and 7.7 months,respectively. The centralised pathology review showed that thehistological diagnosis of LCNEC was difficult, as it led toreclassification of one-fourth of the patients. To ourknowledge, our study is among the largest prospective studiesof advanced LCNEC. No studies have established the optimaltreatment for patients with LCNEC. More specifically, whetherchemotherapy protocols designed for NSCLC or SCLC maybenefit patients with LCNEC remains unknown.
A recent retrospective review of 45 consecutive patients with
advanced LCNEC assessed the outcomes depending on
Figure 2. Progression-free survival (PFS) according to the histological
whether first-line chemotherapy used regimens designed for
diagnosis after a centralised pathology review of 40 (95%) patients; 11
SCLC (n = 11) or for NSCLC (n = 34) []. The response rates
patients were reclassified into the following diagnostic categories: SCLC,
in these two groups were 73% and 50%, respectively (P = 0.19),
n = 9; undifferentiated NSCLC, n = 1; and atypical carcinoid, n = 1).
the median PFS durations were 6.1 and 4.9 months (P = 0.41),and the median OS durations were 16.5 and 9.2 months(P = 0.10). The type and efficacy of salvage chemotherapeutic
4.0–7.9) and the median OS was 8.0 months (95% CI, 3.7–7.9);
regimens differed considerably between the two groups: salvage
the corresponding figures in the 11 patients with diagnoses
regimens including irinotecan, platinum, or taxanes,
other than LCNEC were 3.1 months (95% CI, 2.8–8.5) and 7.0
commonly used in the SCLC-regimen group, provided
months (95% CI, 3.0–9.0), respectively, with no significant
relatively high objective response rates; whereas the frequently
differences compared with the LCNEC group (P = 0.55), as
used salvage agents in the NSCLC-regimen group, such as
pemetrexed, gefitinib, and erlotinib, failed to induce objective
At least one chemotherapy cycle was given to 41 (98%)
responses. A small retrospective review of 12 patients with
patients, and the median number of cycles was four per
LCNEC provided support for the therapeutic approach
patient (Table At least one chemotherapy cycle was
used in SCLC, i.e. cisplatin–etoposide chemotherapy with or
postponed because of leukopaenia/neutropaenia in 23 (56%)
without radiotherapy, which produced partial or complete
patients and at least one dosage reduction was required in 9
responses. Another retrospective study [] enrolled 22
(22%) patients. At least one grade-3/4 toxicity occurred in
patients with measurable LCNEC, including 15 with stage IV
59% of patients; the main grade-3/4 toxic effects were
disease. Chemotherapy consisted of cisplatin and irinotecan
neutropaenia, thrombocytopaenia, and anaemia (32%, 17%,
(n = 9), a platinum agent and paclitaxel (Taxol, n = 6),
and 12% of patients, respectively, Table Reasons for
paclitaxel alone (n = 1), cisplatin and vinorelbine (n = 1),
chemotherapy discontinuation were disease progression
cisplatin and docetaxel (n = 1), or platinum and etoposide
(38%), completion of the six cycles (32%), toxicity (20%),
(n = 4). The objective response rate was 59.1% and the median
PFS and OS were 4.1 and 10.3 months, respectively. Finally, in
three retrospective reviews of, respectively, 14, 20 and 25
2. Abedallaa N, Tremblay L, Baey C et al. Effect of chemotherapy in patients with
patients with LCNEC, treated with various chemotherapy
resected small-cell or large-cell neuroendocrine carcinoma. J Thorac Oncol
regimens LCNEC (the response rate was comparable with that
seen in SCLC; however, the samples size of these studies were
3. Travis WD. Advances in neuroendocrine lung tumors. Ann Oncol 2010; 21:
small, the disease stage varied widely, and in some cases
4. Jones MH, Virtanen C, Honjoh D et al. Two prognostically significant subtypes of
patients had been treated previously [, ,
high-grade lung neuroendocrine tumours independent of small-cell and large-cell
The multicentre design and uniformity of the patient
neuroendocrine carcinomas identified by gene expression profiles. Lancet 2004;
population are major strengths of our study. Cisplatin–
etoposide doublet chemotherapy in our patients with LCNEC
5. Asamura H, Kameya T, Matsuno Y et al. Neuroendocrine neoplasms of the lung:
provided a similar efficacy to that reported in extensive SCLC
a prognostic spectrum. J Clin Oncol 2006; 24: 70–76.
(median PFS and OS values of 4.8 and 9.4 months in the
6. Battafarano RJ, Fernandez FG, Ritter J et al. Large cell neuroendocrine
phase III trial comparing cisplatin–etoposide with cisplatin–
carcinoma: an aggressive form of non-small cell lung cancer. J ThoracCardiovasc Surg 2005; 130: 166–172.
irinotecan and a median OS value of 8.4 months in the phase
7. Fernandez FG, Battafarano RJ. Large-cell neuroendocrine carcinoma of the lung:
III trial of cisplatin–etoposide versus cyclophosphamide–
an aggressive neuroendocrine lung cancer. Semin Thorac Cardiovasc Surg 2006;
epirubicin–vincristine triplet chemotherapy), The
behaviour of advanced LCNEC seems to be similar to that of
8. Gollard R, Jhatakia S, Elliott M et al. Large cell/neuroendocrine carcinoma. Lung
extensive SCLC, and none of the results from our study suggest
9. Sun JM, Ahn MJ, Ahn JS et al. Chemotherapy for pulmonary large cell
Another major strength of our study is the centralised review
neuroendocrine carcinoma: similar to that for small cell lung cancer or non-small
of the histology specimens by a panel of pathologists. LCNEC
cell lung cancer? Lung Cancer 2012; 77: 365–370.
is a poorly recognised and underdiagnosed entity that is
10. Yamazaki S, Sekine I, Matsuno Y et al. Clinical responses of large cell
frequently mistaken for poorly differentiated NSCLC, atypical
neuroendocrine carcinoma of the lung to cisplatin-based chemotherapy. LungCancer 2005; 49: 217–223.
carcinoid tumours, or intermediate cell-type SCLC. This
11. Mazieres J, Daste G, Molinier L et al. Large cell neuroendocrine carcinoma of the
centralised review led to the reclassification of 27.5% of the
lung: pathological study and clinical outcome of 18 resected cases. Lung Cancer
patients, usually as having SCLC. Similarly, in another study
[] only 53% (n = 44) patients were originally correctly
12. Rossi G, Mengoli MC, Cavazza A. Pulmonary large cell neuroendocrine
classified as having LCNEC, whereas 47% were misdiagnosed
carcinoma: a true high-grade neuroendocrine tumor needing prospective
as having NSCLC. These diagnostic errors are chiefly
therapeutic data. J Thorac Oncol 2011; 6: 1775.
ascribable to the difficulty in recognizing the neuroendocrine-
13. Kozuki T, Fujimoto N, Ueoka H et al. Complexity in the treatment of pulmonary
cell morphology by light microscopy, especially in cytology
large cell neuroendocrine carcinoma. J Cancer Res Clin Oncol 2005; 131:147–151.
14. Fujiwara Y, Sekine I, Tsuta K et al. Effect of platinum combined with irinotecan or
In conclusion, the pathological diagnosis of LCNEC is
paclitaxel against large cell neuroendocrine carcinoma of the lung. Jpn J Clin
difficult. The outcomes of advanced LCNEC treated with
cisplatin–etoposide doublets are poor, similar to those of
15. Igawa S, Watanabe R, Ito I et al. Comparison of chemotherapy for unresectable
patients with advanced SCLC. Further prospective studies on
pulmonary high-grade non-small cell neuroendocrine carcinoma and small-cell
LCNEC are needed to better delineate the prognosis and
lung cancer. Lung Cancer 2010; 68: 438–445.
sensitivity to chemotherapy regimens of this rare malignancy.
16. Shimada Y, Niho S, Ishii G et al. Clinical features of unresectable high-grade lung
neuroendocrine carcinoma diagnosed using biopsy specimens. Lung Cancer
17. Noda K, Nishiwaki Y, Kawahara M et al. Irinotecan plus cisplatin compared with
This work was funded by the Groupe Français de Pneumo
etoposide plus cisplatin for extensive small-cell lung cancer. N Engl J Med 2002;
Cancérologie (GFPC) [no grant number].
18. Hanna N, Bunn PA, Jr, Langer C et al. Randomized phase III trial comparing
irinotecan/cisplatin with etoposide/cisplatin in patients with previously untreated
extensive-stage disease small-cell lung cancer. J Clin Oncol 2006; 24:
The authors have declared no conflicts of interest.
19. Varlotto JM, Medford-Davis LN, Recht A et al. Should large cell neuroendocrine
lung carcinoma be classified and treated as a small cell lung cancer or withother large cell carcinomas? J Thorac Oncol 2011; 6: 1050–1058.
1. Travis WD, Linnoila RI, Tsokos MG et al. Neuroendocrine tumors of the lung with
20. Rossi G, Cavazza A, Marchioni A et al. Role of chemotherapy and the
proposed criteria for large-cell neuroendocrine carcinoma: an ultrastructural,
receptor tyrosine kinases KIT, PDGFR alpha. PDGFR-beta, and Met in
immunohistochemical, and flow cytometric study of 35 cases. Am J Surg Pathol
large-cell neuroendocrine carcinoma of the lung. J Clin Oncol 2005; 23:
Veiligheidsinformatieblad volgens (EG) nr. 1907/2006 RUBRIEK 1: Identificatie van de stof of het mengsel en van de vennootschap/onderneming Productidentificatie: Relevant geïdentificeerd gebruik van de stof of het mengsel en ontraden gebruik: Details betreffende de verstrekker van het veiligheidsinformatieblad: Henkel AG & Co. KGaA Henkelstr. 67 40589 Düsseldorf
Commonwealth of MassachusettsMassHealth Drug Utilization Review ProgramP.O. Box 2586 Worcester, MA 01613-2586Fax: 1-877-208-7428 Phone: 1-800-745-7318Anticonvulsant Prior Authorization Request MassHealth reviews requests for prior authorization (PA) on the basis of medical necessity only. If MassHealth approves the request, payment is still subject to all general conditions of MassHealth, inclu
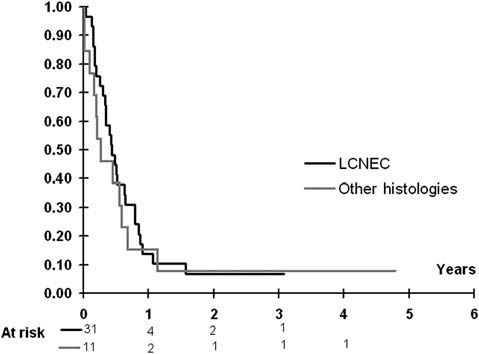
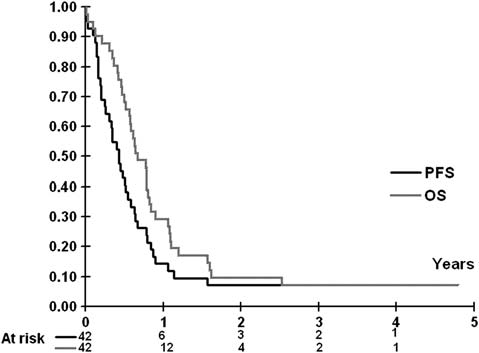 Table 2. Toxicity rates seen in over 10% of the patients and rates of grade-3/4 toxic effects
Figure 1. Progression-free survival (PFS) and overall survival (OS) in the
In this prospective, multicentre study of patients with advancedLCNEC, cisplatin–etoposide doublet chemotherapy provided
median PFS and OS durations of 5.2 and 7.7 months,respectively. The centralised pathology review showed that thehistological diagnosis of LCNEC was difficult, as it led toreclassification of one-fourth of the patients. To ourknowledge, our study is among the largest prospective studiesof advanced LCNEC. No studies have established the optimaltreatment for patients with LCNEC. More specifically, whetherchemotherapy protocols designed for NSCLC or SCLC maybenefit patients with LCNEC remains unknown.
Table 2. Toxicity rates seen in over 10% of the patients and rates of grade-3/4 toxic effects
Figure 1. Progression-free survival (PFS) and overall survival (OS) in the
In this prospective, multicentre study of patients with advancedLCNEC, cisplatin–etoposide doublet chemotherapy provided
median PFS and OS durations of 5.2 and 7.7 months,respectively. The centralised pathology review showed that thehistological diagnosis of LCNEC was difficult, as it led toreclassification of one-fourth of the patients. To ourknowledge, our study is among the largest prospective studiesof advanced LCNEC. No studies have established the optimaltreatment for patients with LCNEC. More specifically, whetherchemotherapy protocols designed for NSCLC or SCLC maybenefit patients with LCNEC remains unknown.