Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
1999; 84-
scientific correspondence
Diminished A␥T fetal globin levels in Sardinian haplo-type II 0-thalassaemia patients are associated with afour base pair deletion in the A␥T promoter. Br JHaematol 1991; 78:105-7.
9. Pistidda P, Frogheri L, Oggiano L, et al. Fetal hemo-
globin expression in compound heterozygotes for -117(G→A) A␥ HPFH and 0 nonsense thalassemia. Am J
10. Pistidda P, Frogheri L, Guiso L, et al. Maximal ␥-glo-
bin expression in the compound heterozygous statefor -175 G␥ HPHF and 0 39 nonsense thalassaemia:a case study. Eur J Haematol 1997; 58:320-5. In vivo effect of chloroquine on platelet aggregation in anesthetized rats Sir,In vivo platelet aggregation was studied by a platelet
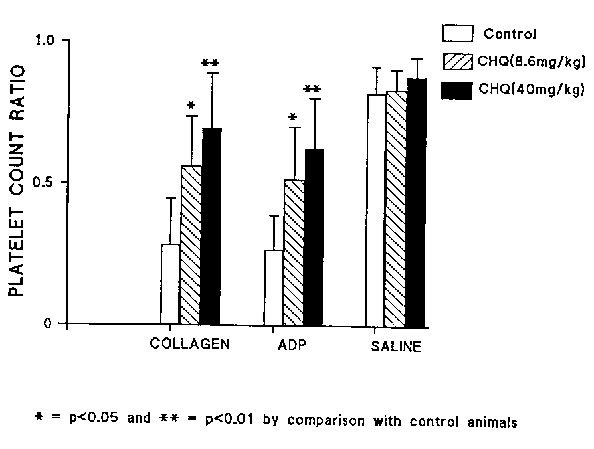
Figure 1. Platelet count ratio in rats administered collagen, adenosine diphosphate (ADP) or normal saline (iv) following
count ratio (PCR) technique. Following the intra-
ip administration of normal saline (1 mL/kg) to control rats
venous administration of collagen or ADP to rats the
(n=6) and chloroquine diphosphate to test rats at either
mean PCR was lower in controls than in two groups
8.6 mg/kg (n=6) or 40 mg/kg (n=6). Values are repre- sented as means±SD.
administered graded doses of chloroquine (p<0.05and 0.01 respectively). Chloroquine inhibits plateletaggregation in vivo in rats.
Previous reports on the effect of chloroquine on
control, first and second test groups respectively. The
platelet aggregation were based on in vitro and ex vivo
ratios for the two test groups were significantly higher
studies where aggregation inducers and chloroquine
(p<0.05 and 0.01) than that of the control group.
were added to isolated platelets, or aggregation
Results after ADP were similar. Platelet count ratios
inducers added to platelets withdrawn from chloro-
following the infusion of normal saline were 0.818±
quine-treated human volunteers.1-3 Since not all the
0.094; 0.830±0.073 and 0.876±0.070 for control, first
factors that affect aggregation in vivo may be avail-
and second test groups respectively. The ratios
able in vitro or ex vivo, the effect of chloroquine on
obtained with saline were not significantly different
platelet aggregation in vivo has been examined.
between the three groups (Figure 1).
Rats were randomly assigned into a control or two
Based on in vitro and ex vivo studies some investigators
test groups (n=6). The control group was adminis-
have concluded that therapeutic concentrations of
tered 0.9% NaCl (1 mL/kg, ip). The first test group
chloroquine have a negligible effect on platelet aggre-
was given ADP at a dose of 8.6 mg/kg, ip1 while the
gation and are not a significant risk to patients with
second test group was administered a higher dose of
compromized hemostasis.1 However, in vitro and ex vivo
chloroquine (40 mg/kg, ip). After one hour, collagen
studies may not reflect in vivo events since some endoge-
(1 mg/kg, iv) was administered under urethane anes-
nous aggregation inducers and inhibitors from non
thesia (1.5 g/kg, ip) to all groups to induce platelet
platelet sources may be reduced or unavailable.
We have shown that a therapeutic dose of chloro-
Blood (1 mL/rat) was taken by cardiac puncture for
quine inhibits platelet aggregation in vivo in rats and
estimation of platelet aggregation.This was measured
so, its use in patients with compromized hemostasis
by a PCR technique4 in which a lowering of the count
could be risky if the results are confirmed in humans.
ratio signifies an increase in platelet aggregation and
Conversely, chloroquine administration could be ben-
vice versa. These experiments were repeated using
eficial in the reduction of hyperaggregability of platelets
another aggregation inducer, ADP (90 µg/kg, iv) and
in malaria7,8 and in the prevention of thrombosis.
normal saline (1 mL/kg, iv). The doses of ADP and col-lagen were slightly higher than those reported for rab-
bits5 since preliminary studies showed that lower dos-
Cephas T. Musabayane, Alison Coutts*
es were ineffective. Serum chloroquine concentration
Departments of Physiology and *Hematology, Faculty of Medicine,
was estimated by the method of Prauty and Kuroda.6
University of Zimbabwe, Harare, Zimbabwe
Mean serum chloroquine concentrations one hour
after administration were 5.06±1.29 mg/L and 10.98±3.75mg/L (mean±SD; p<0.01) in rats administered
Funding
chloroquine at doses of 8.6 mg and 40 mg/kg respec-
This work was supported by grants from the University ofZimbabwe research board (Grant 3YYH103861). The
In the rats given i.v. collagen, the PCR were
authors are deeply indebted to S. Chikosi, N. Bendulo, C.
0.283±0.165, 0.560± 0.175 and 0.694±0.193 in the
Dakwa and B. Nhandara for their skilful technical assistance.scientific correspondence Dakwa and B. Nhandara for their skilful technical assistance.
removal of fibrils as assessed by liver biopsy.
The patient was a 37-year-old male whose com-
Key words
plaints were fatigue and significant maleolar edema. Chloroquine, platelets, in vivo aggregation.
An abdominal ultrasound showed enlarged retro-
Correspondence
peritoneal lymph nodes and after biopsy, a diagno-
Professor E.E. Osim, University of Zimbabwe, Faculty of
sis of Hodgkin’s disease was made. From the blood
Medicine, Department of Physiology, P.O. Box MP 167,
analysis severe hypoproteinemia (4.2 g/dL), hypoal-
Mount Pleasant, Harare, Zimbabwe. Fax/Phone: interna-
buminemia (1.1 g/dL) and increased alkaline phos-
tional +263-4-333678 • E-mail: osim@physiol.uz.zw
phatase (1163 U/L) were found as well as protein-uria (12 g/L). During pathologic staging, amyloid
References
deposition was found in hepatic sinusoids (Figure 1). Immunohistochemical staining confirmed amyloid
1. Cummins D, Faint R, Yardumian D, Dawling S, Mack-
AA deposition. After complete staging the definitive
ie I, Machin SJ. The in vitro and ex vivo effects of chloro-
diagnosis was mixed cellularity Hodgkin’s disease
quine sulphate on platelet function: implications formalaria prophylaxis in patients with impaired hemo-
stage II A with secondary amyloidosis. A renal biop-
stasis. J Trop Med Hyg 1990; 93:112-5.
sy was not performed due to an increased risk of
2. Bertrand E, Cloitre B, Ticolat R, et al. Antiaggregation
bleeding; the nephrotic syndrome was attributed to
action of chloroquine (French). Méd Trop 1990; 50:
After six cycles of COPP/ABV chemotherapy, a
3. Jancinova V, Majekova M, Nosal R, Petrikova M. Inhi-
bition of blood platelet function by cationic amphilic
complete remission was achieved, assessed by com-
drugs in relation to their physico-chemical properties.
puterized tomography. Nevertheless, proteinuria,
Blood Coagul Fibrinol 1996; 7:191-3.
hypoalbuminemia and edema persisted, probably
4. Wu KK, Hoak JC. A new method for the quantitative
due to renal deposition of amyloid. A repeat liver
detection of platelet aggregation in patients with arte-
biopsy showed similar findings to those at diagnosis,
rial insufficiency. Lancet 1974; 19:924-6.
5. Thiemermann C, May GR, Page CP, Vane JR. Endothe-
with the same amount of amyloid deposition. Four
lin inhibits platelet aggregation in vivo: a study with
months after complete remission, biochemical para-
111indium-labelled platelets. Br J Pharmacol 1990; 99:
meters and edema remained at similar levels.
6. Prauty R, Kuroda K. Spectrophotometric determina-
tion and distribution of chloroquine in human tissue. J Lab Clin Med 1958; 52:477-80.
7. Osim EE, Adegunloye BJ, Emeribe AO. In vivo platelet
aggregation in acute malaria. Acta Trop 1991; 49:227-32.
8. Essien EM, Ebhota M. Platelet hypersensitivity in acute
malaria (P. falciparum) infection in man. ThrombHaemostas 1981; 46:547-9. Successful treatment of AA amyloidosis secondary to Hodgkin’s disease with 4’-iodo-4’-deoxydoxorubicin Sir, A case of AA amyloidosis secondary to Hodgkin’s
disease is reported. After complete remission of thelymphoma, treatment with the drug 4’-iodo-4’-de-oxydoxorubicin resulted in an improvement of thenephrotic syndrome and removal of amyloid from liv-er tissue. The drug could be a therapeutic option forsecondary amyloidosis.
Secondary (AA) amyloidosis is known to be asso-
ciated with a variety of diseases in which inflamma-tion is a common feature.1 Apart from control ofunderlying disease, currently there are no treatmentsable to remove amyloid from involved tissues. Pre-liminary reports on the use of the drug 4-iodo-4’-deoxydoxorubicin in primary (AL) amyloidosis seemencouraging.2 We report here a case of AA amyloi-dosis secondary to Hodgkin’s disease in which treat-ment with 4’-iodo-4-deoxydoxorubicin resulted in
Figure 1. Liver biopsy showing extracellular amyloid depo-
substantial improvement of clinical status and
sition (Congo red, ϫ600). Scientific correspondence
four cycles of therapy with 4-iodo-4’-deoxydoxoru-bicin. Thus, it is reasonable to think that the drug isresponsible for partial resolution of the disease. In ouropinion, use of this drug for the treatment of AA amy-loidoses, as well as AL amyloidosis, should also beinvestigated. Encarnación Pérez Equiza, José María Arguiñano, Department of Hematology, Hospital de Navarra, Irunlarrea s/n,Key words Amyloidosis AA, 4’-iodo-4’-deoxydoxorrubicin, Hodgkin’sCorrespondence Dra E. Pérez Equiza, M.D., Department of Hematology,Hospital de Navarra, Irunlarrea s/n, 31008 Pamplona. Spain. Fax: international +34-948-171511 – Phone: inter-national +34-948-422235.References
1. Falk RH, Comenzo RL, Skinner M. The systemic amy-
loidoses. N Engl J Med 1997; 337:898-909.
2. Gianni L, Bellotti V, Gianni AM, Merlini G. New drug
Figure 2. Liver biopsy; substantial removal of amyloid after
therapy of amyloidosis: resorption of AL-type deposits
treatment (PAS, ϫ600).
with 4’-iodo-4’-deoxydoxorubicin. Blood 1995; 86:855-61.
3. Merlini G, Ascari E, Amboldi N, et al. Interaction of
the anthracycline 4’-iodo-4’-deoxydoxorubicin withamyloid fibrils: inhibition of amyloidogenesis. Proc
At that point, we started treatment with 4-iodo-4’-
deoxydoxorubicin in an attempt to improve the patien-
4. Gillmore JD, Hawkins PN, Pepys MB. Amyloidosis: a
t’s situation. Two weeks later, after four cycles of week-
review of recent diagnostic and therapeutic develop-ments. Br J Haematol 1997; 99:245-56.
ly administration at a dose of 30 mg/m2, a new evalu-ation was performed. Increased albuminemia (2.5g/dL) and proteinemia (4.8 g/dL), decreased alkalinephosphatase (711 U/L) and decreased proteinuria (5
Hepatitis C virus infection and mixed cryoglobulinemia
g/L) were found. Fatigue and edema disappeared and
in patients with lymphoproliferative diseases
a new liver biopsy showed substantial decrease in amy-
loid deposits (Figure 2). After one year of follow-up,
the patient’s status is similar, with hypoalbuminemia
In the last few years hepatitis-C virus (HCV) has
and proteinuria at levels comparable to those achieved
been implicated in the pathogenesis of diverse
at the end of therapy and no drug-related toxicity.
processes originating from B-clonal lymphoid prolif-
Initial reports of in vitro binding to amyloid fibrils3 led
eration, such as mixed cryoglobulinemia (MC) and B-
to clinical studies2 that suggest that 4-iodo-4’-deoxy-
cell non-Hodgkin’s lymphomas (NHL).1,2 However,
doxorubicin might achieve not only blockage of amy-
other studies carried out in other geographic areas
loid deposition but also removal of fibrils from the
have not confimed these observations.3 We, there-
extracellular matrix. The drug has been successfully
fore, analyzed 95 patients affected by B-cell lympho-
used for the treatment of AL amyloidosis but to date,
proliferative diseases (B-LPD), seen from October
there are no reports of its use in AA amyloidosis.
1991 to December 1995 at the Hematology Depart-
The possibility of improvement after resolution of
ment of the University Hospital of Zaragoza, Spain.
underlying Hodgkin’s disease cannot be completely
B-LPD was diagnosed on the basis of morpholog-
ruled out,4 but the evolution of biological parameters
ic and immunologic evaluation of lymph nodes, bone
was not uniform. No improvement was achieved four
marrow or peripheral blood specimens. All the
months after complete remission of the lymphoma,
processes were classified according the REAL classi-
but proteinuria and edema dramatically changed after
fication.4 Detection and characterization of cryo-
A Neurobiological Approach to Foreign Policy Analysis: Identifying Individual Differences The Pennsylvania State University and the United States Studies Centre, Sydney Abstract: A great deal of foreign policy analyses relies on social and environmental factors, or anecdotal evidence. In seeking to address this problem in a more systematic manner, we move from an investigation centered around st
Veterinaria, Anno 14, n. 1, Aprile 2000 REGOLAZIONE DELLA PRESSIONE ARTERIOSA ED IPERTENSIONE NEL CANE E NEL GATTO: FISIOLOGIA, FISIOPATOLOGIA, CLINICA E TERAPIA MARCO POGGI Dr. Med. Vet., Centro Veterinario Imperiese, Imperia LUCIANA BERGAMASCO Dr. Med. Vet., Dip. Morfofisiologia Veterinaria, Facoltà di Medicina Veterinaria di Torino, Torino MICHELE BORGARELLI Dr.
 scientific correspondence
scientific correspondence scientific correspondence
scientific correspondence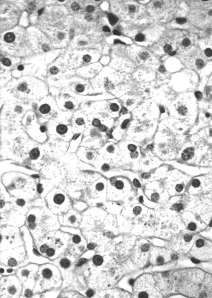 Scientific correspondence
Scientific correspondence