Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
073 ao
Review Article Pleurodesis: technique and indications* MARCELO COSTA VAZ1, EVALDO MARCHI2, FRANCISCO SUSO VARGAS3 ABSTRACT Recurrent pleural effusion, which is commonly seen in clinical practice, compromises patient quality of life, especially in patients with advanced malignant disease. The therapeutic approach to the pleural space involves a wide range of techniques, including aggressive procedures such as pleurectomy. Among such techniques, pleurodesis is the most frequently used. Pleurodesis can be induced through the insertion of pleural catheters, as well as through major surgical procedures (such as thoracotomy). There are various recommended sclerosing agents, including talc (which is the most widely used), silver nitrate and, recently, proliferative cytokines. This article summarizes the principal approaches to the treatment of recurrent pleural effusion, pleurodesis in particular, addressing the indications for, as well as the advantages and disadvantages of, their application in daily pulmonology practice. Keywords: Pleural effusion, malignant/prevention & control; Pleural neoplasms; Pleura/surgery; Pleurodesis/methods; Silver nitrate; Talc; Recurrence
* Study carried out by the Pleura Group of the Pulmonology Department, Instituto do Coração (InCor, Heart Institute),Universidade de São Paulo (USP, University of São Paulo) School of Medicine - São Paulo, Brazil. 1. Ph.D. Professor in the Pulmonology Department of the Universidade de São Paulo (USP, University of São Paulo)School of Medicine - São Paulo, Brazil. Attending physician in the Pulmonology Department of the Instituto do Coração(InCor, Heart Institute) of the Universidade de São Paulo (USP, University of São Paulo) School of Medicine Hospital dasClínicas - São Paulo, Brazil2. Tenured Professor in the Pulmonology Department of the Universidade de São Paulo (USP, University of São Paulo)School of Medicine - São Paulo, Brazil. Associate Professor, Chief of the Department of Thoracic Surgery at theFaculdade de Medicina Jundiaí (FMJ, Jundiaí School of Medicine) - Jundiaí, Brazil3. Full Professor in the Pulmonology Department of the Universidade de São Paulo (USP, University of São Paulo) Schoolof Medicine - São Paulo. Brazil. Director of the Pulmonology Department of the Instituto do Coração (InCor, HeartInstitute) of the Universidade de São Paulo (USP, University of São Paulo) School of Medicine Hospital das Clínicas - SãoPaulo, BrazilCorrespondence to: Francisco Suso Vargas. R. Itapeva, 500, 4C, Bela Vista - CEP: 01332-000, São Paulo, SP, Brazil. E-mail: pnevargas@incor.usp.br; vargasfs@terra.com.brSubmitted: 3 January 2006. Accepted, after review: 12 January 2006. INTRODUCTION
hemodynamic alterations that can ultimately resultin respiratory distress syndrome or hemodynamic
Recurrent pleural effusion is commonly seen in
shock. The pleural fluid removal, performed with all
clinical practice, and results from the anatomic or
the necessary precautions, is well tolerated and
functional impairment of the pleural surfaces by
significantly improves the dyspnea caused by the
benign or malignant processes. Among the wide
effusion. Nevertheless, since the fluid can rapidly re-
range of clinical entities responsible for the
accumulate, performing multiple thoracenteses
production of these effusions are the transudates
becomes a temporary alternative in the control of
(resulting, in particular, from heart, liver or kidney
recurrent pleural effusion. The need for multiple
failure), and the exudates (principally generated by
punctures is physically and emotionally invasive,
nonspecific infections, tuberculosis or neoplasms).
resulting in evident protein and electrolyte depletion.
In this context, we must highlight the significant
The second option to be considered is prolonged
predominance of cancer, which accounts for
drainage to maintain the pleural cavity free of fluid.
approximately 50% of the total number of these
It should be noted that leaving a drain in place for
deposits.(1) It is estimated that there are approximately
long periods (a month or more) can, in itself, result
200,000 new cases of malignant pleural effusion per
in symphysis of the pleural surfaces, which is highly
year in the USA.(2) In Brazil, despite the lack of precise
positive. Nonetheless, prolonged drainage results in
epidemiological surveys, it is believed that, due to
great nutritional deprivation,(3) increases the risk of
the common characteristics of the two countries, the
pleural infections and can decrease survival.(3) Until
number of patients with malignant pleural effusion
recently, such drainage was performed with large-
caliber tubular thoracic drains (34 to 40 F), which
The treatment for recurrent pleural effusion is
have been currently replaced by small-caliber
complex and is aimed at arresting band preventing
catheters (maximum, 16 F). There are very effective
fluid collection, maintaining the pleural cavity free
pleural catheters in the market, such as the pig-tail
from new fluid accumulation. The first step is to
or pleurex, which are highly functional, although their
address the pathological process responsible for the
equally high cost can be an obstacle. Commercial
formation of the effusion. In the case of transudates,
production of these catheters has just recently begun
the treatment is aimed at treating the heart, kidney
in Brazil (Figure 1). This will certainly decrease costs,
or liver failure, whereas it is aimed at treating the
simplify the procedure and benefit our patients.
infection or cancer in the case of exudates. However,
The third option is using a pleuroperitoneal shunt,
when the systemic treatment of the condition
which is nothing more than a thin catheter with a
responsible for the formation of the effusion does
receptacle (a unidirectional valve) at its midpoint. The
not control the fluid accumulation and does not
extremities of the shunt are placed in the pleural and
prevent its recurrence, local treatment should be
peritoneal cavities, and the catheter, including the
recommended, allowing the free expansion of the
receptacle, follows a subcutaneous trajectory (Figure
lung with subsequent functional improvement. The
2). When the patient presents worsening of symptoms
methods in reference include initial thoracentesis,
(basically dyspnea), the receptacle is repeatedly
pleural drainage, pleuroperitoneal shunt,
compressed, removing fluid from the pleural cavity
and, by virtue of its unidirectionality, sending it to the
The objective of the initial thoracentesis is the
peritoneal cavity. The inconvenience of this system
removal of fluid from the pleural cavity in order to
lies in the small volume of the valve chamber (+ 2 ml),
achieve lung expansion and subsequent functional
which can require an exhaustive number of
improvement. However, due to the potential risks of
compressions of this compartment. For the removal
this procedure, caution is called for regarding the
of 400 ml pleural fluid, more than 200 compressions
volume to be removed from the pleural cavity.
are necessary. Other negative aspects of the system
Therefore, it is recommended that, even in large
are the high valve obstruction rate, the risk of neoplastic
effusions, fluid removal should not exceed 1200 ml
implantation in the abdominal cavity(4) and the high
(maximum, 1500 ml), since the removal of larger
cost, which makes it practically unviable in Brazil.
volumes of fluid increases the risk of developing
pulmonary edema, in addition to respiratory or
undoubtedly the most effective procedure. Figure 1 - Catheter for pleurodesis (manufactured in Brazil); A) drainage/pleurodesis kit and components; B) introduction of the guidewire into the catheter; C) catheter ready to be introduced into the pleural cavity and D) simulation of the assembled kit draining the pleural fluid
However, it has been contraindicated due to the
fluid. This has been the procedure most often used
in the case of complete pulmonary expansion and
mortality.(5) In fact, the high risk of complications
the general condition of the patient is good. It is
is justifiable since it is major surgery and the
currently the best option for the control of recurrent
candidates are patients with impaired general
health status. It represents highly aggressive
It is important to mention that pleurodesis only
treatment of a group of patients with limited
r e p r e s e n t s t h e l o c a l t h e r a p y o f a c l i n i c a l
manifestation, which is generally the treatment for
Finally, there is pleurodesis, that is, the
dyspnea. Therefore, the objective of this procedure
intentional collapse of the pleural surfaces (visceral
is not to change the progression of the cancer,
and parietal) resulting in the symphysis of the
and it is not aimed at prolonging patient survival.
pleural space, which hinders the accumulation of
In view of this, pleurodesis reduces the dyspnea
caused by fluid accumulation in the pleural spaceand consequently results in greater functionalcapacity and better quality of life. OBJECTIVE
Our intention is to discuss the strategies for
inducing pleurodesis in patients with recurrentpleural effusion, especially that of neoplastic origin. We endorse certain methods of execution cited inthe medical literature.
In this review, due to the current tendency
toward simplification of the pleurodesis procedure,we discuss the integration of the skills of clinicalpulmonologists, thoracic surgeons and oncologistsin a joint analysis of the patients, in order to promoteeffective and minimally invasive pleurodesis.
This review is consistent with the line of research
pursued by the Pleura Group of the PulmonologyDepartment of the University of São Paulo Schoolof Medicine, and our objective is quite clear: thecomprehensive evaluation of patients suffering from
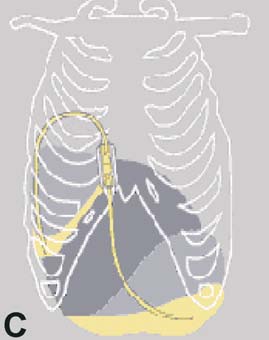
Figure 2 - "Pleuroperitoneal shunt": A) catheter with interposed
pulmonary diseases. We believe that patients with
receptacle (unidirectional valve); B) insertion of one of the extremities
lung cancer should be submitted to holistic treatment
into the pleural cavity; and C) shunt in position, draining fluid from
by the pulmonologist, rather than being referred to
the pleural cavity and directing it toward the abdominal cavity
the oncologist immediately after confirmation of thediagnosis. Therefore, we disagree with those whorecommend referring such patients to a surgeon
Register; and the Evidence-Based Medicine
for the induction of pleurodesis immediately after
Cochrane Database of Systematic Reviews. The
recurrent pleural effusion has been confirmed.
search terms used were 'pleurodesis' and 'pleural
Thanks to recent technological advances and
effusion'. We limited our search to articles that
simplification of procedures, the physician should
focused on efficacy and safety, ruling out case
develop the necessary skills to create continuity in
descriptions, letters to the editor and editorials.
the treatment of these patients, as well as tocoordinate clinical-surgical-oncological integration,
INDICATIONS
in order to offer the best treatment options topatients with neoplasms. (See our proposal regarding
Recurrent benign pleural effusions
minimally invasive outpatient pleurodesis performed
The performance of pleurodesis in recurrent
benign (transudative) pleural effusion is controversial
Therefore, the aim of this discussion is to answer
and should be regarded as a procedure reserved
the following questions: What are the indications
for pleurodesis? What is the best agent for
pleurodesis? What is the best method for the
comparative studies evaluating the efficacy and
safety of pleurodesis in benign processes. Thefindings of observational studies suggest that, in
these situations, pleurodesis is efficacious and safe. However, there is the theoretical fear that, after
pleurodesis of the transudates, the pleural fluid will
bibliographic searches of the following electronic
begin to accumulate in other tissues, such as those
databases: Medline; the Cochrane Controlled Trials
Therefore, the performance of pleurodesis in
effusion (radiological regression of the effusion
recurrent benign pleural effusion is only acceptable
and decreased number of thoracenteses to promote
in those rare situations in which there is absolute
dyspnea relief) is preceded by the performance of
failure of the clinical treatment of the underlying
one or two cycles of chemotherapy (after two to
three months or even at the end of the chemotherapy
Among the causes of recurrent benign pleural
treatment). Although there are factors in favor of and
effusion, we should mention liver, kidney and heart
against these approaches, both indications are
failure, as well as hypoproteinemia and myocardial
decided, other factors that, despite not enjoying a
Recurrent malignant pleural effusions
consensus, can modify the indication criteria
The main indication for pleurodesis resides in
should be considered, since they can interfere with
this group of patients. However, not all the patients
the result expected. Therefore, acid pH (< 7.3),(10)
with malignant pleural effusion benefit from the
low glucose level (< 60 mg/dl) and incidence of
procedure. In some situations, there is a consensus
chylothorax have been related to worse prognosis
regarding the induction of pleurodesis (Chart 1);
and worse efficacy of pleurodesis, independently
in others, it is absolutely controversial.
of the technique and of the drug used (5) (Chart 3).
Once these conditions have been considered,
The presence of lymphangitis and a performance
status index lower than 70 have been associated with
procedure should be analyzed. Some authors
worse clinical evolution of the patient after the
defend the idea that pleurodesis should be
induction of pleurodesis.(5) Finally, lung entrapment,
performed as soon as possible after the diagnosis
either due to pleural loculations or to a lack of
has been confirmed.(9) Others recommend its
pulmonary expansion, reduces the efficacy of
performance only if chemotherapy fails to control
pleurodesis, as well as increasing the risk of infections
the pleural effusion. However, there is no evidence
in the pleural space.(3) Therefore, pleurodesis is not
to support the use of the latter strategy. In this
situation, the analysis of the control of the pleural
PERFORMANCE OF PLEURODESIS - Chart 1 - Indications for pleurodesis METHODOLOGY Types of procedures Indications
Pleurodesis can be achieved through the use of
Failure of oncological treatment to control pleural
various stimuli: direct physical lesion (abrasion);
instillation of caustic or irritating chemical substances
Dyspnea relief after drainage of the pleural cavityFull pulmonary expansion (chest X-ray)
(talc, doxycycline, silver nitrate or bleomycin) into
Karnofsky performance status index > 70
the pleural space; or immunological induction with
Corynebacterium parvum, transforming growth factor-beta (TGF-ß) or interferon-alpha 2 (IFN-a 2). Chart 2 - Ideal moment for the performance of pleurodesis Indication
Makes oncological treatment more difficult
Greater risk of empyemaPoorer performance status
Chart 3 - Prognostic factors of the efficacy of
the ideal sclerosing agent (Chart 4).
Chemical stimulation has the advantage of
allowing various routes of access to be combined. Worse prognostic and least efficacy
The most important aspect, in this particular case,
is that pleurodesis can be achieved surgically or
Presence of chylothorax Presence of lymphangitis
efficacious sclerosant. When compared with other
agents, it presents a relative risk of 1.34 fortherapeutic success (95% confidence interval: 1.16to 1.55) and a success rate of over 90% in moststudies.(11) However, in a recent multicenter study
Mechanical stimuli
conducted in Europe, talc was found to be
Among the mechanical stimuli, abrasion is the
efficacious in 71% to 78% of the patients submitted
principal method. Abrasion is carried out during a
to pleurodesis, all of whom survived for more than
surgical intervention, whether conventional or
30 days after the procedure.(12) Talc has been
video-assisted, in which the surgeon exfoliates the
considered the agent of choice, since it presents
pleural mesothelium, creating friction with a rough-
many of the characteristics cited in the definition
surfaced material (gauze, for example). This
of an ideal agent (low cost, wide distribution, easy
irritation results in the desquamation of the
administration, high efficacy and low rate of side
mesothelium and activation of the inflammation
effects). It can be administered, either by
and coagulation pathways, with subsequent
insufflation during thoracotomy or through drains
proliferation of fibroblasts and collagen deposition,
of various calibers, in the form of so-called talc
slurry (talc suspension in saline solution). Despite
Pleural abrasion is not currently used in the
its low rate of complications, its use has been
control of recurrent neoplastic pleural effusions
associated with acute respiratory distress syndrome,
due to its lesser efficacy, as well as to the high risk
which affects 1.2%(7) to 9% of patients(13) and can
of bleeding in the regions involved and to the
be fatal. It is believed that this complication is
possibility of tumor dissemination. These two risks
related to the size of the talc particles. The smaller
are related to the direct manipulation of the tumor
ones would be more easily absorbed from the
w i t h l e s i o n o f n e w l y f o r m e d v e s s e l s a n d
pleural cavity and distributed throughout the
embolization of tumor cells that are released
circulation, resulting in a greater risk of remote
during the manipulation of the tumor mass.
complications.(14) Due to the severity of this type
Another inconvenience of pleural abrasion is that
of complication, other drugs again began to be
it requires surgical intervention. Its indication has
been currently recommended only for selectedcases of recurrent pneumothorax. Chart 4 - Characteristics of the ideal sclerosant agent Chemical stimuli Characteristics
Pleurodesis induced by chemical stimuli was
first carried out at the beginning of the last century.
There are references to the fact that, in 1901,
Spengler injected silver nitrate into the pleural
cavity for the control of recurrent pneumothorax.(5)
Apparently, talc was first introduced into the
pleural cavity, with the objective of collapsing the
existing residual space after pulmonary resection,
by Bethune in 1935.(5) Since then, various
Minimal, easily controlled morbidity Near 100% efficacy
substances have been used to induce pleurodesis,although there is as yet no consensus regarding
Doxycycline has proven efficacious and safe
efficacy of this agent has not been reproduced in
for the induction of pleurodesis. However, it is not
Brazil, and there are currently difficulties in its
available in many countries (including Brazil). In
production, and there is no distribution network.
the past, some health facilities in Brazil utilized
oral tetracycline/doxycycline derivatives to induce
interleukin 2-alpha, staphylococcal superantigen
pleurodesis. Nevertheless, there are doubts as to
and TGF-β. In a comparative, randomized,
whether the sclerosing effect observed is due to
prospective, parallel study carried out in 2004, IFN-
the agent used or to the excipient (talc). In
a 2b was found to be less efficacious than
addition, we should also be concerned with the
bleomycin,(17) and its use was not indicated for
sterilization of the agent introduced in the pleural
pleurodesis induction. Staphylococcal superantigen
cavity, since the capsules are in fact commercially
seems to be a promising agent, despite having been
distributed for oral ingestion and their content is
little studied. In a study carried out in 2004,(18)
not sterile and are therefore not recommended for
staphylococcal superantigen was instilled in
fourteen patients with low performance status
Silver nitrate was the first substance utilized in
indices. It was successful in eleven patients (71%),
the induction of pleurodesis, being abandoned,
without any side effects. Its principal advantage is
for reasons that remain unclear, in the 1980s. Our
ease of administration, not requiring hospitalization
group recently posited that the adverse effects
or thoracic drainage. Since these results are still
observed in the past were secondary to the high
preliminary, further studies of efficacy and safety
concentrations of silver nitrate used (from 1% to
are required. Finally, TGF-β is a cytokine that
10%), and we therefore suggested that the use of
stimulates tissue proliferation and collagen
lower concentrations would be safer and more
formation, without inducing an inflammatory
efficacious.(15) In studies with laboratory animals
reaction or tissue lesion. The major concern
(rabbits), 0.5% silver nitrate proved highly efficacious
regarding its use is related to its systemic
and presented a low rate of complications.(16) The
absorption, with development of fibrosis in other
pathophysiological mechanism involved in the
organs, including the lung. It was successfully
induction of pleurodesis seems to be, to a certain
tested in experimental animals with low short-term
extent, different from that observed with the talc,
complication rates.(19) However, studies analyzing
since, in this rabbit model, the corticosteroid did
its efficacy and safety in humans have yet to be
not reduce the efficacy of the pleurodesis obtained
carried out. It is rather unlikely that TGF-β will
with silver nitrate, in contrast to what occurs with
prove to be the ideal sclerosing agent, since its
the talc. A recently published study involving
cost is higher than that of other agents.
human subjects with neoplastic pleural effusion
Therefore, we can conclude that, despite the
and utilizing 0.5% silver nitrate, demonstrated
lack of consensus, talc, in the dosage of five to
efficacy indices similar to those found for talc, with
ten grams, remains the most accepted agent.
low rates of side effects.(15) Naturally, furthercomparative studies of the safety and efficacy of
Route of access
silver nitrate in humans are required.
Route of access is defined as the method by
Bleomycin is an antineoplastic agent that was
which the sclerosing agent is given access to the
used to induce pleurodesis in past decades. However,
pleural space, either through classical thoracotomy,
its low efficacy and high cost have significantly
through video-assisted surgery, through thoracic
drainage with local anesthesia or through thoracicdrainage with thoracic puncture and a small-caliber
Immunological stimuli
Chief among the immunostimulants is C.
All of these techniques present advantages and
parvum. Its principal advantage is that it does not
disadvantages that can interfere with the final
require surgical intervention or pleural drainage
result of the procedure (Chart 5). Among the
and can be introduced into the pleural space
advantages, we can cite the complete drainage of
through a simple puncture. However, the described
distribution of the sclerosing agent in the pleural
and can be more easily introduced, being currently
space, less aggressiveness of the procedure and
recommended as an option for the initial approach
less need for hospitalization. These factors
to recurrent pleural effusion and for the induction
influence the choice of the technique that is most
Small-caliber drains have been successfully
In these past few years, the route of access for
used in the performance of rapid pleurodesis. In
pleurodesis has been thoroughly studied. There is
this new form of pleurodesis induction, the
a tendency to reduce the aggressiveness of the
pleural catheter is put in place, the sclerosant is
treatment, migrating from talc insufflation during
instilled, the drain (with a unidirectional valve
thoracotomy to video-assisted insufflation and
system that allows the outflow of the fluid but
eventually to the instillation of sclerosant through
does not allow the air to get in and prevents
a thoracic drain. Even when the thoracic drain is
backflow of the fluid into the pleural space) is
used as a route of access to the pleural cavity,
left open, and the drain is generally removed
there is a tendency toward reducing its complexity
within 48 h.(21) The combination of small-caliber
and morbidity (pain). Therefore, we have evolved
drains with a valve system, such as the Heimlich
from using large-caliber to using small-caliber
valve, which is a unidirectional valve system that
drains and ultimately to the use of pleural catheters.
allows the replacement of the water-seal (Figure
In parallel with the reduced aggressiveness, the
2), has facilitated pleurodesis induction, allowing
efficacy of the treatment must be maintained. The
greater patient mobility and comfort, as well as
ideal route of access for striking a balance between
a l l o w i n g p l e u r o d e s i s t o b e p e r f o r m e d i n
efficacy and safety in pleurodesis has yet to be
defined. Unfortunately, many studies comparingroutes of access have not employed the same
CONCLUSIONS AND RECOMMENDATIONS
sclerosing agent for each route, thereby making itdifficult to interpret the isolated effect of the route
of access to the pleural space. A meta-analysis
indicated in benign pleural effusions, with
carried out in 2004(11) by the Pain, Palliative Care
restrictions. The principal indication for pleurodesis
and Supportive Care Group of the Cochrane
is recurrent malignant pleural effusions, with full
Database of Systematic Reviews (112 patients),
pulmonary expansion, in patients with good
evaluated the efficacy of talc pleurodesis using
video-assisted surgery or using drainage/talc slurry
Pleurodesis via chemical stimulus, especially talc
(talc in suspension). The authors showed that the
pleurodesis, remains the first option for the
instillation through video-assisted surgery was
treatment of recurrent malignant pleural effusion.
more efficacious, with favorable relative risk of
Silver nitrate seems to be a reasonable option for
1.19 (95% confidence interval: 1.04 to 1.36) and
use in Brazil, although more studies of its safety
similar mortality in the two groups. Unfortunately,
in this meta-analysis, it was not possible to
The most efficacious route of access is video-
compare the adverse effects of the two treatments
assisted surgery. However, the use of small-caliber
due to the lack of pertinent data in the studies
thoracic drains (catheters) provides a good cost-
involved. Despite the fact that video-assisted
effectiveness/comfort ratio, especially for patients
surgery was found to be more efficacious than
in advanced stages of neoplastic disease.
slurry pleurodesis, the level of success for both
The most significant aspect to be considered
is that pleurodesis has become a procedure to can
be carried out in outpatient clinics by physicians.
The current evidence suggests there is no
This simplifies its execution considerably while
difference between the use of large-caliber thoracic
maintaining the indices of efficacy. Therefore, there
drains and small-caliber thoracic drains (catheters).
is no need for hospitalization, which would deprive
Although a consensus has yet to be reached, small-
patients, during this difficult phase of their life, of
caliber drains provides more comfort to the patient
Chart 5 - Techniques employed in the performance of pleurodesis Technique
Hospitalization requiredComplicates use of soluble drugs
Hospitalization requiredComplicates use of soluble drugs
Hospitalization requiredTalc slurry not possible
Feasible with lower performance statusSoluble drugs can be used
Chart 6 - Proposal/protocol for outpatient pleurodesis by a physician or surgeon
• Confirm the diagnosis of neoplastic pleural effusion through cytological or anatomopathological study. • Confirm lung expansion after initial thoracentesis (X-ray or tomography). • The better the general status of the patient (Karnofsky > 60), the better the result. • Introduce small-caliber catheter/drain, connect Heimlich valve draining into collection bag (or colostomybag).
• The patient can go home after detailed explanation about special care and how to change the collectionbag. Provide guidance on access to medical treatment in case of emergency. Patient can return after sevendays.
• Induce pleurodesis. There are basically two options, injecting through the catheter: a) 5 g of talc insuspension with 100 mL of saline solution; or b) 20 ml of a solution of 0.5% silver nitrate.
• Confirm the diagnosis of neoplastic pleural effusion through cytological or anatomopathological study. • There is no need for analgesia. The procedure is well tolerated. However, it is convenient to have access toan opioid (morphine, meperidine or tramadol), since significant pain can be observed, which will be reducedby the medication, allowing the proposed procedure to continue.
• After the intrapleural introduction of the sclerosant agent, inject 20 ml of saline solution to wash thecatheter, clamp it for one hour, and then open it to allow the drainage of the fluid. Leave it open. There isno need to move (rotate) the patient while the catheter is clamped.
• The patient can be discharged after receiving guidance regarding necessary care. In general, commonpainkillers (dipyrone or equivalent) are sufficient. More potent drugs are rarely necessary, and we suggesttramadol or opioids. Avoid the use of nonsteroidal anti-inflammatory drugs or corticosteroids, since they canreduce the efficacy of the pleurodesis. Ask the patient to write down the volume drained daily, and schedulean appointment for the following week.
• If the drainage is inferior to 100 ml/day, and there is no sign of obstruction of the catheter or of pleuralloculation, remove the catheter. Conduct clinical follow-up evaluation and follow-up imaging studies (X-ray,ultrasound or tomography). REFERENCES
1. DiBonito L, Falconieri G, Colautti I, Bonifacio D, Dudine
Oncology Group. Phase III intergroup study of talc
S. The positive pleural effusion. A retrospective study of
poudrage vs talc slurry sclerosis for malignant pleural
cytopathologic diagnoses with autopsy confirmation.
effusion. Chest. 2005;127(3):909-15.
13. Rehse DH, Aye RW, Florence MG. Respiratory failure following
2. Light RW, editor. Pleural diseases. 3rd ed. Baltimore:
talc pleurodesis. Am J Surg. 1999;177(5):437-40.
14. Maskell NA, Lee YC, Gleeson FV, Hedley EL, Pengelly G,
3. Varga FS, Teixeira LR, Marchi E. Derrame pleural. 4a ed.
Davies RJ. Randomized trials describing lung inflammation
after pleurodesis with talc of varying particle size. Am J
4. Genc O, Petrou M, Ladas G, Goldstraw P. The long-
Respir Crit Care Med. 2004;170(4):377-82.
term morbidity of pleuroperitoneal shunts in the
1 5 . Paschoalini MS, Vargas FS, Marchi E, Pereira JR, Jatene
management of recurrent malignant effusions. Eur J
FB, Antonangelo L, et al. Prospective randomized trial
Cardiothorac Surg. 2000;18(2):143-6.
of silver nitrate vs talc slurry in pleurodesis for
5. Vargas FS, Teixeira LR. Pleural malignancies. Curr Opin
symptomatic malignant pleural effusions. Chest.
6. Dikensoy O, Light RW. Alternative widely available,
1 6 . Vargas FS, Antonangelo L, Capelozzi V, Vaz MA, Genofre
inexpensive agents for pleurodesis. Curr Opin Pulm Med.
EH, Marchi E, et al. Lung damage in experimental
pleurodesis induced by silver nitrate or talc: 1-year
7. de Campos JR, Vargas FS, de Campos Werebe E, Cardoso P,
follow-up. Chest. 2002;122(6):2122-6.
Teixeira LR, Jatene FB, et al. Thoracoscopy talc poudrage:
17. Sartori S, Tassinari D, Ceccotti P, Tombesi P, Nielsen I,
a 15-year experience. Chest. 2001;119(3):801-6.
Trevisani L, et al. Prospective randomized trial of
8. Webb WR, Ozmen V, Moulder PV, Shabahang B, Breaux
intrapleural bleomycin versus interferon alfa-2b via
J. Iodized talc pleurodesis for the treatment of pleural
ultrasound-guided small-bore chest tube in the palliative
effusions. J Thorac Cardiovasc Surg. 1992;103(5):881-
treatment of malignant pleural effusions. J Clin Oncol.
9. Marrazzo A, Noto A, Casa L, Taormina P, Lo Gerfo D,
1 8 . Ren S, Terman DS, Bohach G, Silvers A, Hansen C, Colt
David M, et al. Video-thoracoscopic surgical pleurodesis
H, et al. Intrapleural staphylococcal superantigen
in the management of malignant pleural effusion: the
induces resolution of malignant pleural effusions and
importance of an early intervention. J Pain Symptom
a survival benefit in non-small cell lung cancer. Chest.
1 0 . Crnjac A, Sok M, Kamenik M. Impact of pleural effusion
1 9 . Gary Lee YC, Teixeira LR, Devin CJ, Vaz MA, Vargas FS,
pH on the efficacy of thoracoscopic mechanical
Thompson PJ, et al. Transforming growth factor-beta2
pleurodesis in patients with breast carcinoma. Eur J
induces pleurodesis significantly faster than talc. Am
Cardiothorac Surg. 2004;26(2):432-6.
J Respir Crit Care Med. 2001;163(3 Pt 1):640-4.
11. Shaw P, Agarwal R. Pleurodesis for malignant pleural
2 0 . Clemensten P, Evald T, Grode G, Hansen M, Krag
effusions. Cochrane Database Syst Rev. 2004;(1):CD002916.
Jacobsen G, Faurschou P. Treatment of malignant
Comment in: ACP J Club. 2004;141(2):43.
pleural effusion: pleurodesis using a small percutaneous
1 2 . Dresler CM, Olak J, Herndon JE 2nd, Richards WG,
catheter. A prospective randomised study. Respir Med.
Scalzetti E, Fleishman SB, Kernstine KH, Demmy T,
Jablons DM, Kohman L, Daniel TM, Haasler GB,
2 1 . Yildirim E, Dural K, Yazkan R, Zengin N, Yildirim D,
Sugarbaker DJ; Cooperative Groups Cancer and Leukemia
Gunal N, et al. Rapid pleurodesis in symptomatic
Group B; Eastern Cooperative Oncology Group; North
malignant pleural effusion. Eur J Cardiothorac Surg.
Central Cooperative Oncology Group; Radiation Therapy
Complementary Medicine: Handle with Care Ken Harvey Adjunct Senior Research Fellow, School of Public Health, La Trobe UniversitySome forms of complementary medicine are efficacious but many have unproven or nohealth benefits. Claims that cannot be substantiated by scientific research are common,In Australia, complementary medicines are equitable access and cost-effective use of necessar
MSE Policy Review in Nepal: Current Reform Process in Government Prof. Dinesh P. Chapagain 1. Conceptualization: MSE Value Chain for Development Poverty reduction has been the foremost development objective of Nepal since it embarked on planned development efforts almost half a century ago. Given the country’s geo-political condition and small economic scale, the micro a


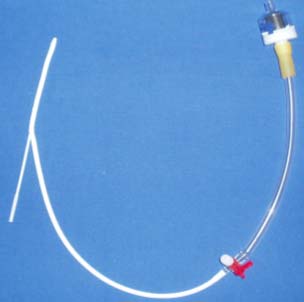
 Figure 1 - Catheter for pleurodesis (manufactured in Brazil); A) drainage/pleurodesis kit and components; B)
Figure 1 - Catheter for pleurodesis (manufactured in Brazil); A) drainage/pleurodesis kit and components; B)

 caused by fluid accumulation in the pleural spaceand consequently results in greater functionalcapacity and better quality of life.
caused by fluid accumulation in the pleural spaceand consequently results in greater functionalcapacity and better quality of life.