Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Microsoft powerpoint - poster aptivus-hepatotox_a0_5,guhl 22.6.07.ppt
Hepatotoxicity during therapy with Tipranavir, Citalopram and Finasterid – a case report C. Guhl¹, W. J. Heinz¹, R. Winzer¹, P. Langmann², H. Klinker¹
¹ Department of Internal Medicine II, Division of Infectious Diseases, University of Würzburg, Germany
² Private practice, Am Tiefen Weg, 97753 Karlstadt, Germany
Background
Other causes of elevated liver enzymes like alcohol, viral hepatitis or opportunistic infections could be excluded. The patient mentioned
Tipranavir (TPV) is a new potent protease inhibitor. Side effects like
concomitant use of the antidepressant Citalopram and the hair restorer
hepatotoxicity have been described, whereas severe elevation of liver
Finasterid. Elevation of liver enzymes is considered to be a rare side effect
enzymes has been noticed in about 10% within 24 weeks of treatment.
of these drugs and has been little investigated. As both drugs are
Various interactions of co-medication with TPV can be found in literature.
metabolized via CYP3A4, inhibition of this cytochrome can increase their
They are hard to predict before and are even little investigated so far. In
plasma concentration. Due to this knowledge and the rather low TPV-levels
combination with Ritonavir (r), TPV itself inhibits cytochrome P450-CYP3A.
at that time (see below), the comedication has been stopped in July 2006
Combination of TPV/r with drugs metabolized via CYP3A can cause
whereas the ART has been retained unchanged. GOT and GPT decreased
interactions like elevated plasma levels of the co-medication and
during time (GOT 31 U/l, GPT 54 U/l at a six months-follow up), and GGT
consequently lead to side effects. We report one case of severe
decreased to 342 U/l six months later.
hepatotoxicity during therapy with TPV/r and a backbone of Tenofovir (TDF)
Due to resistance against TPV and intermediate susceptibility towards the
(FTC) and co-medication with the antidepressant
backbone with consequently increasing viral load and a decreasing CD4
Citalopram and the hair restorer Finasterid.
cell count, medication had to be modified again in March 2007 and an untilltoday successful combination of TMC-125 / Darunavir / Saquinavir / r has been started. After having stopped TDF/FTC/TPV/r, even GGT decreased
Case report
During the period when these severe elevated liver enzymes could be
A 38-years old male HIV-positive patient was planned to have a new
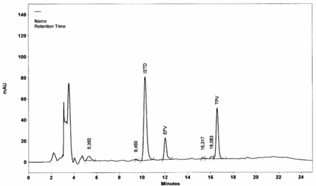
determined, therapeutic drug monitoring (TDM, an example of High
antiretroviral therapy (ART). He has already taken various HAART regimens
performance liquid chromatography (HPLC) results is shown in fig. 4)
during the past six years. Due to insufficient medical adherence, various
showed low plasma levels of TPV (8.1 to 18.5µg / ml, see fig. 5) and
resistances against all three ART classes and missing sufficient therapeutic
Ritonavir (57 to 303 ng / ml). On account of this, these antiretroviral agents
options, he was not taking any medication from April 2004 onwards. During
were not supposed to have caused the observed severe hepatotoxicitiy.
the next months, the lab results showed elevating viral load and a decreasing CD4 cell count (figure 1 and 2).
HIV1-RNA [copies/ml] Fig. 4: Example of Therapeutic Drug Monitoring of Tipranavir Fig. 1: HIV-1 RNA in copies/ml;
(TPV) with High performance liquid chromatography (HPLC);
measured plasma level of TPV: 17,3 µg/ml
CD4+ / µl Plasma levels [ng / ml] Fig.2: CD4+ count; *: start of TDF/FTC/TPV/r Fig. 5: Plasma trough levels of Tipranavir [µg/ml] in the mentioned
Therefore, treatment with Tenofovir (TDF), Emtricitabin (FTC) and the
patient; supposed effective level > 25 µg / ml
recently available Tipranavir (TPV) combined with Ritonavir (r) was started in January 2006, whereas TDF and FTC had already been prescribedbefore. In the course, blood results showed elevating liver enzymes with a peak (GOT 168U/l, GPT 654U/l, GGT 454U/l) approximately six months
Conclusion
The reported case shows that hepatotoxicity during therapy with Tipranavir
can be observed, but it also shows that not only the antiviral drug should be
considered as the causative drug. Drug interactions are very complex, but
should always be kept in mind when confronted with side effects like
hepatotoxicity. Thus, co-medication and especially free available or herbal
As GGT only decreased to its normal level after having stopped the TPV-
containing therapy, one might assume that TPV itself might partially have
caused the hepatotoxicity. However, normal or even low plasma levels of
TPV undermines that hypothesis. We therefore suggest that TDM helps to
Fig. 3: Liver enzymes after start of TDF/FTC/TPV/r (
find or exclude the causative drug, and cases like the reported one
stopping co-medication ( ) and stopping TDF/FTC/TPV/r
Anti-staphylococcal activity of ent-kaurane-type diterpenoids fromGiang P.M., Son P.T., Matsunami K., Otsuka H. Faculty of Chemistry, College of Natural Science, Vietnam National University, 19 Le Thanh Tong, Hanoi,Viet Nam; Graduate School of Biomedical Sciences, Hiroshima University, 1-2-3 Kasumi, Minami-ku,Abstract: Ent-kaurane-type diterpenpoids 1-11, isolated from the dried leaves of the
THE CONSULTANT GROUP, P.C. RHEUMATOLOGY NEW PATIENT QUESTIONNAIRE NAME:____________________________________________________BIRTHDATE: ___ RACE: __ ____SEX:M F___ RIGHT HANDED( )LEFT HANDED( ) NAME OF PHYSICIAN WHO REFERRED YOU:_______________________________________ ADDRESS:__________________________________________________________________________________________________________________


 Hepatotoxicity during therapy with Tipranavir, Citalopram
Hepatotoxicity during therapy with Tipranavir, Citalopram