Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Doi:10.1016/j.maturitas.2006.06.004
The effect of tibolone versus 17-estradiol on climacteric
symptoms in women with surgical menopause:
A. Somunkiran , C.T. Erel , F. Demirci , M.L. Senturk
a Abant Izzet Baysal University, Duzce Medical School, Department of Obstetrics and Gynecology,
b Istanbul University, Cerrahpasa Medical School, Department of Obstetrics and Gynecology,Division of Reproductive Endocrinology, Turkey
Received 19 December 2005; received in revised form 25 May 2006; accepted 4 June 2006
Abstract Objective: To compare the effectiveness of tibolone and 17-estradiol on climacteric symptoms, in a randomized, single-blind,cross-over study in surgically menopausal women. Material and methods: Forty surgically menopausal women were divided randomly into two groups. Group A received treatmentwith tibolone for 6 months, while group B received 17-estradiol. After 3 weeks washout period, treatment protocols wereexchanged for another 6 months. The climacteric symptoms were assessed with Greene Climacteric Scale at baseline, duringwashout and after the treatments. Statistical analysis was done with the Wilcoxon’s Sign Rank test. Results: Both treatments significantly improved the scores of all subscales with respect to baseline. However, the improvementin psychological, somatic and sexual subscales were significantly superior in the tibolone group compared with 17-estradiolgroup. Both treatments showed comparable improvements in the relief of vasomotor symptoms. Conclusion: Our findings suggest that tibolone may improve mood, libido and somatic symptoms in surgically menopausalwomen to a greater extent than estrogen therapy alone. 2006 Elsevier Ireland Ltd. All rights reserved. Keywords: Surgical menopause; Tibolone; 17-Estradiol; Greene Climacteric Scale
1. Introduction
flushes, sweating, changes in mood and libido are someimportant outcomes affecting the quality of life (QoL)
The decline in circulating estrogen levels in the
during climacterium in women. Quality of life covers
perimenopause results in climacteric symptoms. Hot
physical, functional, emotional, social and cognitivevariables menopause-associated symptoms can
impair these major aspects of QoL for many women.
Corresponding author. Tel.: +90 532 6346799;
After the results of The Women’s Health Initiative
E-mail address: (A. Somunkiran).
(WHI) study, to improve the quality of life in women
0378-5122/$ – see front matter 2006 Elsevier Ireland Ltd. All rights reserved. A. Somunkiran et al. / Maturitas 56 (2007) 61–68
during the menopausal transition period is the main
The climacteric scale constructed by Greene, is
indication for estrogen plus progestin based hormone
based on factor analysis studies This scale inde-
therapy (HT) Another issue is the quality of life
pendently measures psychological, somatic, vasomotor
in women undergoing surgical menopause. Since
and sexual symptoms and is used as a quality of life
the circulating sex steroids abruptly decrease, the
measurement in estrogen replacement trials
climacteric symptoms are more severe and disturb-
and in a population-based study to obtain normative
ing in women undergoing bilateral oophorectomy.
data for climacteric symptoms A recently pub-
Estrogen replacement therapy (ERT) improves the
lished study by Lam et al. investigated the effect of
complaints and in turn, quality of life. But ERT arm of
tibolone on menopause symptoms, psychological well-
the WHI study was terminated prior to the scheduled
being and dyadic relationships. In this randomized
close-out interval, because of increased risk of stroke,
placebo-controlled crossover study the menopausal
and the likelihood that neither cardioprotection nor
symptoms were assessed by Greene Climacteric Scale
breast cancer risk would be demonstrated in the
remaining intervention period s a result hormone
In the present study, we conducted a randomized
therapies, estrogen plus progestin or estrogen alone,
cross-over trial to compare the effects of tibolone and
are appropriate for the relief of vasomotor symptoms,
17-estradiol on climacteric symptoms, in women with
and primarily recommended for the prevention of
surgical menopause, with a standardized scale.
menopausal symptoms for the shortest possibletime. The effects of alternatives to HRT, such astibolone, phytoestrogens or SERMs, need to be
2. Material and methods
Tibolone is a tissue specific compound, struc-
A randomized, controlled, cross-over trial was con-
turally related to 19-nortestosterone derivatives, which
ducted at Department of Obstetrics and Gynecology,
exhibits weak estrogenic, progestagenic and andro-
Duzce School of Medicine to compare the effects of
genic activities In a number of studies, it has
tibolone and 17-estradiol in climacteric symptoms
been shown that tibolone provided relief of vasomotor
in women with surgical menopause. The study pro-
symptoms without stimulating endometrium and breast
tocol was approved by the Medical Ethics Committee
tissue The success of this relatively new com-
of Duzce Medical School and conformed to the ethical
pound, tibolone, in treating climacteric symptoms after
guidelines of the 1975 Helsinki Declaration. Informed
natural/surgical menopause, has not been addressed
written consent was obtained from each woman before
by well-designed studies. Albertazzi et al. reviewed
the studies in which tibolone was used for climac-teric symptoms. According to them the problems with
study designs were; the randomized double blind stud-ies were not cross-over, in the cross-over studies there
Forty women who had been subjected to hysterec-
were no washout periods, and measurement of symp-
tomy and bilateral oophorectomy for benign gyneco-
logical conditions in our clinic were enrolled to the
The effect of tibolone versus estrogen on climac-
study. All of the patients were in the perimenopausal
teric symptoms in women with surgical menopause was
period before the operation and none of them had been
the subject of two previous studies but both of
treated with hormones for their climacteric complaints
them used the Blatt–Kupperman Indices to measure cli-
before the operation. The initial screening included
macteric symptoms/complaints. The Blatt–Kupperman
medical history, physical and gynecological exami-
Index has severe limitations such as; the symptoms are
nation, measurement of systolic and diastolic arterial
highly selected, the scales have no psychometric prop-
blood pressures, height and weight and a mammogra-
erties and they are derived from biased samples. It is
phy if not performed during the previous 12 months.
argued that this index should be replaced by standard-
Complete blood count, urine analysis and blood bio-
ized scales that have reported properties of reliability
chemistry were done. All analysis was found to be in
the normal range. Any women who had hypertensive
A. Somunkiran et al. / Maturitas 56 (2007) 61–68
disorders (systolic BP > 170 mmHg and/or diastolic
teric symptoms. GCS was performed at baseline, after
BP > 105 mmHg), active liver disease, cerebrovascular
the washout and after the treatments. A different author
or thromboembolic disorders, diabetes mellitus, thy-
(AS), blind to the type of treatment, was responsible for
roid disorders, any malignancies and chronic disease
which may affect the quality of life, were excludedfrom the study.
The Greene Climacteric Scale measures a total of
21 symptoms. Each symptom is rated by the woman
Cross-over study design was used to define whether
herself according to its severity using a four-point
the treatment with tibolone was effective, with respect
rating scale: (0, not-at-all; 1, a little; 2, quite a bit;
to estrogen for each woman. Patients were randomly
3, extremely). Symptoms 1–11 address psychological
allocated into two groups, group A or group B, accord-
symptoms divided in a measure of anxiety (a sum of
ing to a computer-generated list of random num-
symptoms 1–6) and of depression (a sum of symptoms
ber groups, and were followed for 1 year
7–11). Somatic aspects are addressed in symptoms
The time interval between the surgery and the study
12–18 and vasomotor symptoms in symptom 19 and
was 3 weeks. Patients assigned to group A received
20. Symptom 21 is a probe for sexual dysfunction.
tibolone 2.5 mg/day (Livial®, NV Organon, Holland)
The total Greene climacteric score is the sum of all
for the first 6 months of study, and for the remain-
ing 6 months they received 17-estradiol (Estrofem®,Novo-Nordisk, Denmark) 2 mg/day. Patients allocated
to group B received 17-estradiol 2 mg/day for the firsthalf of the study, and tibolone 2.5 mg/day for latter
The mean score of each symptom is calculated by
half of the study. There was a 3-week washout period
the sum of all individual scores divided by the number
between treatments. One author (FD) was responsible
of subjects. The score of the clusters are given as the
for the randomization and the same author also assessed
sum of the mean scores of the symptoms within that
the subjects’ compliance to the study medication by
checking the empty boxes, and counting the unused
For comparisons between baseline, tibolone and
drugs. A patient was considered non-compliant if, on
17-estradiol the non-parametric Wilcoxon Sign Rank
at least 4 days within a period (28 days) no tablets were
Test was used. Results were analyzed using the SPSS
for Windows statistical package (SPSS/PC software,
The Greene Climacteric Scale (GCS) questionnaire
Chicago, IL). p-Value of <0.05 was accepted as statis-
was used to detect the efficacy of treatments on climac-
3. Results
After randomization 20 patients were assigned to
group A and 20 to group B. There were no significantdifferences in the baseline demographic and clinicalcharacteristics between the two groups (
ws the mean scores of the 21 items of the
Greene Climacteric Scale at baseline, and the changesof the scores from baseline according to the treatment,and the efficacy of tibolone and 17-estradiol. Dataindicate that, both 17-estradiol and tibolone signif-icantly improved palpitations, nervousness, sleeping
Fig. 1. Design of the study; GCS: Greene Climacteric Scale.
disorders, excitability, concentration, tiredness, loss of
A. Somunkiran et al. / Maturitas 56 (2007) 61–68
Table 1Basal characteristics of the patients
a Data are presented as mean and S.D.
b NS, Non-statistically significant.
interest in most things, feeling unhappy or distressed,
The scores of the several subscales (psychological,
crying spells, irritability, parts of body feel numb or
somatic, vasomotor and sexual) at baseline and after
tingling, muscle and joint pains, hot flushes, night
sweats and libido with respect to baseline. Neverthe-
baseline, all subscores improved in both groups during
less, with regard to the improvement of nervousness,
treatment. Tibolone treatment, however, produced sig-
sleeping disorders, concentration, tiredness, loss of
nificantly greater improvements in all subscores, except
interest in most things, feeling unhappy or distressed,
for vasomotor subscore, which were similar in both
crying spells and libido a significant between group
differences was observed. A significant better improve-
In order to investigate the carryover effect Wilcoxon
ment was observed in the above parameters during
Sign Rank Test was performed between the baseline
tibolone usage with respect to 17-estradiol. More-
GCS and after the washout GCS. None of the parame-
over, headaches significantly improved during the use
ters were statistically significant between baseline and
of tibolone in comparison to 17-estradiol.
Table 2Mean score of the 21 items of the Greene Climacteric Scale during the treatment with tibolone and 17-estradiol
A. Somunkiran et al. / Maturitas 56 (2007) 61–68
Table 3Mean score ± S.D. of the symptoms clusters of the Greene Climacteric Scale during the treatment with tibolone and 17-estradiol
* Number of items of the cluster in parentheses.
Two women in the tibolone/estrogen group (group
Tibolone also significantly lowers SHBG and
A) withdrew because of a change in employment, while
increases circulating free testosterone, further adding
they were taking estrogen pills. Their last GCS was
performed by phone calls. Other than these two, all
Tibolone has been shown to improve vasomotor
subjects were compliant and completed the study.
symptoms, emotional reactions, sleep disturbances
During the use of tibolone, two women experi-
enced hirsutism, both in the estrogen/tibolone sequence
(group B) of assumption and there were no other
This study was focused on the effects of two differ-
ent forms of hormone replacement therapy on climac-teric symptoms in surgically menopausal women. Bothtibolone and 17-estradiol showed improvements in
4. Discussion
the relief of climacteric symptoms. Tibolone treatment,however, produced significantly greater improvements
After menopause, a progressive decline in both
in psychological, somatic and sexual symptoms com-
ovarian and adrenal androgen production occurs. This
effect is most dramatic in women undergoing bilat-
The findings of the studies examining the effects
eral oophorectomy. In women who undergo surgical
of tibolone on mood are not consistent. Meeuwsen
menopause, serum testosterone and androstenedione
et al. found an improvement in emotional reactions
levels fall acutely, by approximately 50% Surgi-
and sleep disturbances with 12 months of tibolone
cal menopause is associated with a more acute onset
therapy. But in that placebo-controlled trial, in the
of menopausal symptoms and deterioration in sexual
placebo group, an unexpected significant better score
life than natural menopause Furthermore, use
was observed in the physical mobility parameter, with
of estrogen replacement further decreases the amount
regard to tibolone In a double blind placebo-
of bioavailable androgens by increasing the levels of
controlled crossover study by Lam et al., tibolone
sex hormone binding globulin (SHBG), thereby fur-
treatment and placebo showed the same improvements
ther lowering the amount of bioavailable testosterone
on the psychological well-being in GCS In a
Thus, even adequately estrogenized, surgically
double-blind, cross-over placebo-controlled study of
menopausal women are at risk for androgen deficiency.
20 oophorectomized women, Crona et al. found that
Tibolone is a synthetic steroid that has estrogenic,
tibolone and estradiol valerate reduced hot flushes and
androgenic, and progestagenic properties. Tibolone
improved mood to a similar degree and both com-
itself has no biological activity; its effects are the results
pounds were effective than placebo. But the study
of the activity of its metabolites on various tissues. Its
period was too short (6 weeks for each preparation) and
4-isomer has androgenic effects on brain and liver
there was no washout period in the above mentioned
A. Somunkiran et al. / Maturitas 56 (2007) 61–68
study Albertazzi et al., in a very small sample
Although there are studies favoring estrogen in the
sized study, found no effect of tibolone and continuous
relief of vasomotor symptoms our finding is in
combined estradiol–norethisterone acetate therapy on
agreement with other studies that found tibolone to be
mood et al. compared the effects of tibolone
as clinically effective in controlling vasomotor symp-
and CEE-MPA on QoL in 501 naturally menopausal
women, and in that double blind, randomized trial they
Four of the items in the somatic subscale were absent
found no difference in total GCS score and psycho-
at the baseline and they remained unchanged during the
logical subscore between the tibolone and CEE-MPA
treatment period. Of the three items present at baseline,
two (parts of body feel numb or tingling, and muscle
As mood improvement can be induced by andro-
and joint pains) were improved by both treatments.
gens, the significantly greater improvement in psy-
Alleviation in headache was achieved with tibolone
chological symptoms in the tibolone group compared
only. Improvement in headache with tibolone was also
with 17-estradiol group, in the present study, may be
cantly improvement in somatic subscale with tibolone
formed in the brain. Genazzani et al. found that tibolone
compared with estrogen is the result of the improve-
increased -endorphin levels in the plasma and pitu-
ment in headache only. The present study gives further
itary, and proposed that this might contribute to the
support to the study of Lam et al., which showed that
improved mood in postmenopausal women. However,
tibolone treatment as compared with placebo treatment
mood was not directly assessed in their trial
had a significant beneficial effect on the somatic symp-
better improvement of tibolone in well-being in the
present study may also be attributed to the effects of
One limitation of this prospective randomized cross-
over study was that the treatment packages of tibolone
Although both medications improved libido,
and estrogen were not identical, so the patients were
tibolone therapy was superior to 17-estradiol in the
aware that their treatment medication changed after the
current study. Several other studies of tibolone consis-
washout. But the women in the groups did not have any
previous knowledge about whether these drugs might
Although understanding of the role played by andro-
have any effect on sexual functions, psychological and
gens in female sexual function remains incomplete, it
somatic symptoms and we did not give any information
is widely accepted that androgens exert an important
about those either. We aimed to assess the effect of two
influence on sexual function trials in post-
different treatments on QoL in surgically menopausal
menopausal women have consistently demonstrated
women. Concern can arise that hysterectomy may
that addition of androgens to estrogen replacement
also affect the QoL. But, in the patients enrolled to
results in a significant improvement of sexual func-
the study, hysterectomy and bilateral oophorectomy
tion, particularly sexual desire In the end,
was performed for benign gynecological conditions, to
the effect of tibolone on libido may be the result of
enhance the quality of life. Research shows that in most
its androgenic activity, as well as its SHBG lowering
women suffering from gynecological disorders, quality
of life is improved within a month after hysterectomy;
An internet held study reported that vasomo-
the surgery does not produce any psychological distur-
tor symptoms were overwhelmed by psychosomatic
bances in otherwise psychologically healthy women
symptoms, like; feeling tired/worn out, feeling lack of
energy and muscle and joint aches the symp-
In conclusion tibolone as well as 17-estradiol
toms “hot flushes” and “sweating at night” were the
improves psychological, somatic, sexual and vaso-
highest scored symptoms in the present study. This data
motor symptoms in surgically menopausal women.
supports the results of Barentsen et al. who found that
However, overall in this study a trend favoring tibolone
the most prevalent symptoms were vasomotor symp-
was observed. In the tibolone group in relation to
the psychological, somatic and sexual symptoms, a
Similar reductions in the vasomotor symptoms were
significant better improvement was observed com-
found with both medications in the present study.
pared to the estrogen group. Our findings suggest
A. Somunkiran et al. / Maturitas 56 (2007) 61–68
that tibolone may improve the proposed symptoms
[15] Davis SR. Testosterone deficiency in women. J Reprod Med
of female androgen deficiency; fatigue, diminished
well-being and loss of libido; to a greater extent than
[16] Nathorst-Boos J, von Schoultz H. Psychological reactions and
sexual life after hysterectomy with and without oophorectomy.
estrogen therapy alone, in surgically menopausal
Gynecol Obstet Invest 1992;34:97–101.
[17] Mathur RS, Landgreve SC, Moody LO, Semmens JP,
Williamson HO. The effect of estrogen treatment on plasmaconcentrations of steroid hormones, gonadotropins, prolactin
References
and sex hormone binding globulin in post-menopausal women. Maturitas 1985;7:129–33.
[18] Kloosterboer HJ. Tibolone: a steroid with a tissue-specific mode
[1] Blumel JE, Castelo-Branco C, Binfa L, et al. Quality of life
of action. Steroid Biochem Mol Biol 2001;76:231–8.
after the menopause: a population study. Maturitas 2000;34:
[19] Doren M, Rubig A, Coelingh Bennink H, Holzgreve W. Dif-
ferential effects of the androgen status of postmenopausal
[2] Writing Group for the Women’s Health Initiative Investi-
women treated with tibolone and continuous combined estra-
gators. Risks and benefits of estrogen plus progestin in
diol and norethindrone acetate replacement therapy. Fertil Steril
healthy postmenopausal women. Principal results from the
Women’s Health Initiative randomized controlled trial. JAMA
[20] Meeuwsen IB, Samson MM, Duursma SA, Verhaar HJ. The
influence of tibolone on quality of life in postmenopausal
[3] The Women’s Health Initiative Steering Committee. Effects
of conjugated equine estrogen in postmenopausal women with
[21] Palacios S, Menendez C, Jurado R, Castano JC, Vargas JC.
hysterectomy. The Women’s Health Initiative randomized con-
Changes in sex behavior after menopause: effects of tibolone.
trolled trial. JAMA 2004;291(14):1701–12.
[4] Palacios S. Tibolone: what does tissue specific activity mean?
[22] Laan E, Van Lunsen RH, Everaerd W. The effects of tibolone
on vaginal blood flow, sexual desire and arousability in post-
[5] Moore RA. Livial: a review of clinical studies. Br J Obstet
menopausal women. Climacteric 2001;4:28–41.
Gynaecol 1999;106(Suppl. 19):1–21.
[23] Crona N, Samsioe G, Lindberg U-B, Silfverstolpe G. Treat-
[6] Albertazzi P, Di Micco R, Zanardi E. Tibolone: a review. Matu-
ment of climacteric complaints with Org OD 14: a comparative
study with oestradiol valerate and placebo. Maturitas 1988;9:
[7] Castelo-Branco C, Vicente JJ, Figueras F, et al. Comparative
effects of estrogens plus androgens and tibolone on bone, lipid
[24] Albertazzi P, Natale V, Barbolini C, Teglio L, Di Micco R. The
pattern and sexuality in postmenopausal women. Maturitas
effect of tibolone versus continuous combined norethisterone
acetate and oestradiol on memory, libido and mood of post-
[8] Mendoza N, Suarez AM, Alamo F, Bartual E, Vergara F,
menopausal women: a pilot study. Maturitas 2000;36:223–9.
Herruzo A. Lipid effects, effectiveness and acceptability
[25] Huber J, Palacios S, Berglund L, et al. Effects of tibolone and
of tibolone versus transdermic 17-estradiol for hormonal
continuous combined hormone replacement therapy on bleed-
replacement therapy in women with surgical menopause. Matu-
ing rates, quality of life and tolerability in postmenopausal
[9] Alder E. The Blatt-Kupperman menopausal index: a critique.
[26] Genazzani AR, Petraglia F, Genazzani AD, Bergamaschi M,
Grasso A, Volpe A. Effects of Org OD 14 on pituitary and
[10] Greene JG. Constructing a standard climacteric scale. Maturitas
peripheral -endorphin in castrated rats and postmenopausal
[11] Derman RJ, Dawood MY, Stone S. Quality of life during
[27] Nathorst-Boos J, Hammar M. Effect on sexual life-a compari-
sequential hormone replacement therapy; a placebo controlled
son between tibolone and a continuous estradiol-norethisterone
acetate regimen. Maturitas 1997;26:15–20.
[12] Ulrich LG, Barlow DH, Sturdee DW, et al. Quality of life
[28] Davis SR. The effects of tibolone on mood and libido.
and patient preference for sequential versus continuous com-
bined HRT: the UK Kliofem multicenter study experience. Int
[29] Montgomery J, Brincat M, Tapp A, et al. The effect of estro-
gen and testosterone implants on psychological disorders of the
[13] Barentsen R, van de Weijer PHM, van Gend S, Foekema H.
Climacteric symptoms in a representative Dutch population
[30] Sherwin BB, Gelfand MM, Brender W. Androgen enhances sex-
sample as measured with the Greene Climacteric Scale. Matu-
ual motivation in females: a prospective, crossover study of sex
steroid administration in the surgical menopause. Psychosom
[14] Lam PM, Cheung GWY, Shek DTL, et al. A randomized,
placebo-controlled, crossover study of tibolone (Livial) on
[31] Davis SR, McCloud P, Strauss BJ, Burger HG. Testosterone
menopause symptoms, psychological well-being, and dyadic
enhances estradiol’s effects on postmenopausal bone density
relationship of postmenopausal Chinese women and their
and sexuality. Maturitas 1995;21:227–36.
spouses. Menopause 2004;11:416–22. A. Somunkiran et al. / Maturitas 56 (2007) 61–68
[32] Conboy L, Domar A, O’Connell E. Women at midlife: symp-
[34] Egarter C, Sator M, Berghammer P, Huber J. Efficacy, tolerabil-
toms, attitudes, and choices. An internet-based survey. Maturi-
ity, and rare side effects of tibolone treatment in postmenopausal
women. Int J Gynaecol Obstet 1999;64:281–6.
[33] Volpe A, Facchinetti F, Grasso A, Petraglia F, Campanini
[35] Rannestad T. Hysterectomy: effects on quality of life and
D, Genazzani AR. Benefits and risk of different hormonal
psychological aspects. Best Pract Res Clin Obstet Gynaecol
replacement therapies in postmenopausal women. Maturitas
Eiskalter Blick zum Urknall Quantenphysiker ebnen Weg zu neuen Materiezuständen in ultrakalten Atomgemischen Einen Meilenstein in der Erforschung von Quantengasmi- schungen haben Forscher des Instituts für Quantenoptik und Quanteninformation (IQOQI) in Innsbruck erreicht. Der Gruppe um Rudolf Grimm und Florian Schreck gelang es erstmals, in einem Quantengas zwischen zwei fermio- n
Detail-Document #211113 −This Detail-Document accompanies the related article published in− PHARMACIST’S LETTER / PRESCRIBER’S LETTER November 2005 ~ Volume 21 ~ Number 211113 Sulfa Drugs and the Sulfa-allergic Patient *Health Canada Product Labeling Listed by Exception* Sulfonamide-Containing Agents: Summary of Cross-Reactivity Information Drug FDA Comments1,2,
 The effect of tibolone versus 17-estradiol on climacteric
symptoms in women with surgical menopause:
A. Somunkiran , C.T. Erel , F. Demirci , M.L. Senturk
a Abant Izzet Baysal University, Duzce Medical School, Department of Obstetrics and Gynecology,
b Istanbul University, Cerrahpasa Medical School, Department of Obstetrics and Gynecology,
Division of Reproductive Endocrinology, Turkey
Received 19 December 2005; received in revised form 25 May 2006; accepted 4 June 2006
Abstract
The effect of tibolone versus 17-estradiol on climacteric
symptoms in women with surgical menopause:
A. Somunkiran , C.T. Erel , F. Demirci , M.L. Senturk
a Abant Izzet Baysal University, Duzce Medical School, Department of Obstetrics and Gynecology,
b Istanbul University, Cerrahpasa Medical School, Department of Obstetrics and Gynecology,
Division of Reproductive Endocrinology, Turkey
Received 19 December 2005; received in revised form 25 May 2006; accepted 4 June 2006
Abstract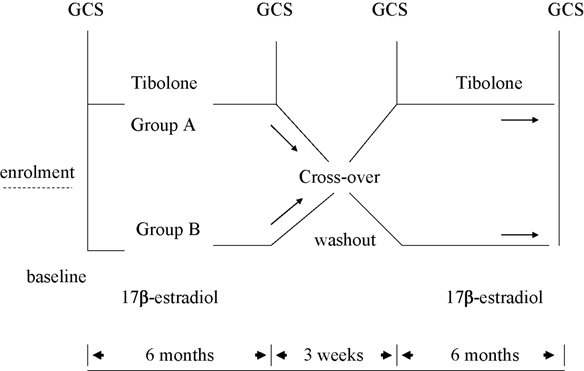 A. Somunkiran et al. / Maturitas 56 (2007) 61–68
disorders (systolic BP > 170 mmHg and/or diastolic
teric symptoms. GCS was performed at baseline, after
BP > 105 mmHg), active liver disease, cerebrovascular
the washout and after the treatments. A different author
or thromboembolic disorders, diabetes mellitus, thy-
(AS), blind to the type of treatment, was responsible for
roid disorders, any malignancies and chronic disease
which may affect the quality of life, were excludedfrom the study.
A. Somunkiran et al. / Maturitas 56 (2007) 61–68
disorders (systolic BP > 170 mmHg and/or diastolic
teric symptoms. GCS was performed at baseline, after
BP > 105 mmHg), active liver disease, cerebrovascular
the washout and after the treatments. A different author
or thromboembolic disorders, diabetes mellitus, thy-
(AS), blind to the type of treatment, was responsible for
roid disorders, any malignancies and chronic disease
which may affect the quality of life, were excludedfrom the study.