Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
801645 1095.1099
International Journal of Obesity (2001) 25, 1095±1099
ß 2001 Nature Publishing Group All rights reserved 0307±0565/01 $15.00www.nature.com/ijo
PAPERGastrointestinal side effects of orlistat may be
prevented by concomitant prescription of natural
®bers (psyllium mucilloid)H Cavaliere1, I Floriano1 and G Medeiros-Neto1*
1Department of Clinical Medicine, University of SaÄo Paulo Medical School, SaÄo Paulo, Brazil
OBJECTIVES: This placebo-controlled open study was designed to test the hypothesis that most of the gastrointestinal (GI) side
events induced by treatment of obese patients with orlistat (a gastrointestinal lipase inhibitor) could be prevented or
ameliorated by concomitant use of natural ®bers (psyllium mucilloid).
DESIGN: Two groups of obese women (BMI b 27 kgam2) were treated with orlistat 120 mg three times a day. One group
(A, n 30) was randomized to receive orlistat and, approximately 6.0 g of orange-¯avored psyllium mucilloid dissolved in water
and the other group (B, n 30) received orlistat and orange-¯avored placebo. At the end of 30 days and 2 weeks of washout,
group A switched to placebo and group B received psyllium while continuing orlistat three times a day.
SUBJECTS: Sixty professional women, more than 21-y-old with a body mass index (BMI) between 27.3 and 48.0 kgam2, who
were not receiving any other medication.
MEASUREMENTS: Assessments included weekly visits to attending physician, ®lling a form in which GI events were recorded,
monthly measurements of body weight, blood pressure and serum lipids. The frequency and severity of GI events were
evaluated by a score system, based on information provided by the patients.
RESULTS: Both groups A and B signi®cantly lost (P ` 0.01) weight after 60 days of orlistat (A 96.8 to 94.9 kg and B 98.7 to
96.5 kg). Similarly, BMI values declined signi®cantly in both groups. While in the psyllium plus orlistat group (group A) the mean
Æ s.e.m. of the scores re¯ecting GI events was 13.0Æ 1.8, the placebo plus orlistat group (B) had a value of 35.9Æ 2.7 (P ` 0.01).
When the reverse situation was instituted the placebo and orlistat group presented a mean score of 36.1Æ 3.6 and the psyllium
plus orlistat a mean score of 8.9Æ 1.5 (P ` 0.01).
CONCLUSIONS: Psyllium hydrophilic mucilloid concomitantly prescribed to obese patients receiving 120 mg of orlistat three
times a day is an effective and safe adjunct therapy that is helpful in controlling the GI side effects of this pancreatic lipase
International Journal of Obesity (2001) 25, 1095 ± 1099
Keywords: obesity; lipase-inhibitor; orlistat; gastrointestinal effects; natural ®bers; psyllium
excreta. In volunteers and obese subjects the maximal fecal
Orlistat, a hydrogenated derivative of lipstatin is a potent
fat loss, depending on the dose of orlistat and the amount of
inhibitor of gastric and pancreatic lipase.1±6 By inhibiting
fat in the diet, was about one-third (30%) of the ingested fat,
the intestinal lipase the therapeutic use of orlistat leads to a
reaching a plateau with doses around 360 mgaday.
decreased fat absorption and subsequent excretion of the
The side effects with orlistat are to be expected from its
unabsorbed triglycerides, cholesterol and fat in the fecal
mechanism of action on pancreatic lipase. These includeintestinal ¯atulence, borborygmi and abdominal cramps.5The most troubling were fecal incontinence, oily spotting
*Correspondence: G Medeiros-Neto, Division of Endocrinology,
Department of Clinical Medicine, Hospital das Clinicas, University of SaÄo
and ¯atus with discharge. In a large European Multicentre
Paulo Medical School Av. Eneas C. Aguiar 255-8A-bl. 3, 05403-900 SaÄo
Orlistat study group2 adverse gastrointestinal (GI) events
were a common reason for premature withdrawals in the
orlistat treated group. In another randomized controlled trial
Received 13 July 2000; revised 29 November 2000;
of obese subjects treated for 2 y with orlistat (Multicentre
Table 1 Age, weight-loss and BMI variation
American Study) at least one GI event was experienced by
obesity, were not under treatment for other conditions, were
79% of the subjects in the orlistat group.4 Gastrointestinal
willing to cooperate and had no gastrointestinal signs or
adverse events seem to increase with large doses of orlistat3
symptoms. Other exclusion criteria were weight loss of
and have a tendency to be less frequent in the second year of
more than 4 kg in the 3 months before screening, bulimia
and laxative abuse, use of any drug that might have in¯u-
Psyllium is a water-soluble, gel-forming ®ber derived from
enced bodyweight, alcohol abuse, history of prior chole-
the husks of blonde psyllium seeds (Plantago ovata, English
cystectomy or intestinal surgery, and inability to follow
plantain, commonly referred as `ispaghula'). Psyllium
instructions or to accurately report symptoms. After a single
belongs to a group of soluble ®bers that show cholesterol-
lead-in period of 4 weeks during which the patients received
lowering effects when added to patients' diets.7±11 Moreover,
nutritional advice and were instructed to exercise according
dietary ®ber, such as psyllium, may increase the fractional
to their possibilities and capacities, the patients were ran-
turnover of bile acids, probably by increasing their fecal
domly assigned to two groups of 30 subjects (Table 1).
elimination. Also psyllium has been used to absorb intestinal
Group A (n 30), meanÆ s.e.m. age, 40.8Æ 7.9-y-old, with
fat both in obese and diabetic patients.10 Thus it was
a meanÆ s.e.m. weight of 98.82Æ 17.8, a BMI of 38.09Æ
assumed that the constant use of psyllium hydrophilic
5.26 kgam2, were assigned to receive orlistat 120 mg three
mucilloid might be effective in diminishing the adverse
times daily, with the meals, for a period of 4 weeks. The
effects of unabsorbed fat caused by orlistat.
patients were instructed to ingest the orlistat capsules with
In this study we have decided to use the bene®cial
approximately 6.0 g of orange-¯avored psyllium hydrophillic
gastrointestinal effects of a psyllium hydrophilic mucilloid
mucilloid, with no added sugar, dissolved in a glass of water.
in patients treated with orlistat, in order to minimize the GI
Group B (n 30), meanÆ s.e.m. age 41.7Æ 8.9 y, with a
events that are relatively common in this therapy.
meanÆ s.e.m. weight of 98.78Æ 16.81 kg, BMI of 38.17Æ4.81 kgam2, were similarly assigned to receive orlistat120 mg three times daily with meals for 4 weeks. These
patients also received, approximately, 6.0 g of a soluble
orange-¯avored powder (placebo) to be dissolved in water
Eligible obese patients all women, with ages from 27 to 42-y-
and ingested with the orlistat capsules three times a day.
old (meanÆ s.d. 40.9Æ 8.9-y-old) with body mass index
Both the psyllium powder and the placebo orange powder
(BMI) b 27 kgam2, were recruited by advertisement in the
were packed in small identical sachets to be open at home.
university hospital weekly newsletter. All of them were
Both the patient and the attending physician were blind to
employed by the hospital as of®cials, nurses and laboratory
personnel. Women of childbearing potential were included if
After 15 days of a washout period, the patients from group
they were using adequate contraception. The study con-
A were assigned to receive orlistat plus placebo and those
formed to the Declaration of Helsinki and was approved by
from group B received the orlistat capsules plus psyllium
the Ethics Committee of the University Hospital. All partici-
pants gave written informed consent. The main reason for
All patients were seen by one of the authors (HC) on a
using the university hospital personnel was to have a uniform
weekly basis. At each visit the patients were asked to return a
group of obese patients that were not actually being treated
printed form in which each GI event occurring during the
for obesity, would have a predictable low drop-out rate, would
week was recorded, on a daily basis (Table 2). The attending
be able to report accurately signs and symptoms related to GI
physician, therefore, was able to assign the number of points
events during orlistat therapy and could be easily contacted,
to reach the GI events score for that week. At the end of 30
on a daily basis, during the period of the project.
days, the total number of points for each patient was
A total of 110 obese patients were initially eligible for the
recorded and tabulated for further statistical analysis.
study. Of these, 60 obese women were ®nally recruited by
After this ®rst part of the study was completed it was
personal interview. They were lacking major complications of
noticed that most patients complained that it was not
Figure 1 Schematic design of the research project.
agreeable to ingest the orlistat capsules with the psyllium
The data was analyzed with a GraphPad Prism software
orange-¯avored drink, at each meal, mainly in public places
(version 2.0, Graphpad Software Inc., San Diego, CA, USA).
such as restaurants, cafeterias and social gatherings. There-
Analysis of variance was used to examine body weight, BMI
fore, we started a new study design in which orlistat capsules
and serum-lipids values. Paired t-tests were used to examine
(120 mg) were prescribed to be taken three times a day, with
differences between means. The w2 method was employed for
meals, as previously done but the psyllium or placebo were
differences between frequency of GI events in speci®c groups
given as a single drink with approximately 12 g of orange-
¯avored powder in water, at bedtime. Only 30 patients fromthe original group of 60 subjects volunteered for this secondpart of the project, being randomly assigned, as previously
described, 15 to each group of placebo and psyllium during
The weekly visit to the attending physician and the need to
During the 60 days of treatment periods, patients were
hand out the printed form where the GI events were
prescribed a standard mildly hypocaloric diet containingroughly 30% of energy as fat. The estimated energy intake
Table 2 The scoring system for quanti®cation of the GI adverse
was 1200 kcaladay. The same diet was prescribed in the
The score system. The scoring system was previously
designed by interviewing obese patients in orlistat treat-
ment. The major adverse and troubling events were oily
spotting (¯atus with discharge) and fecal incontinence.
Therefore it was decided to assign to these events, respec-
tively, a scoring of 4 and 5 (in a scale of 0 ± 5). Similarly, other
side effects such as increased defecation, soft stools, ¯atu-
lence, abdominal pain and fecal urgency received scores
between 1 and 3. When the adverse events were more
frequent (in a weekly basis) the scores would concomitantly
increase, as shown in Table 2. Previous to the start of this
study, the scoring system was tested in a group of obese
patients on orlistat treatment and we concluded that it
re¯ected the actual intensity of the adverse effects.
Table 3 GI side effects; meanÆ s.e.m. scores for group A and group B
placebo (group A vs group B). Similarly, when we comparedthe meanÆ s.e.m. of the scores of GI events between (1) psyl-
lium three times a day plus orlistat and (2) psyllium 12.0 g at
bedtime there was no statistical difference between them(10.8Æ 1.7 vs 6.11Æ 1.21), respectively.
In Table 4 we have listed the total number of GI events
occurring with 60 patients either while on orlistat pluspsyllium or orlistat plus placebo. Overall GI events were
2 ± 6-fold more common during orlistat plus placebo ascompared to orlistat plus psyllium. After analysis of thedata by the w2 statistical method, this difference was highly
recorded was considered to be an excellent way to prevent
withdrawals and to achieve compliance. All 60 patientscompleted the two periods of 30 days each. For the secondpart of the project we randomly assigned the 30 patients that
volunteered to continue the study for another 30 days to two
Orlistat belongs to a class of anti-obesity agents that act
groups of 15 patients, as previously mentioned.
directly and speci®cally at the site of fat breakdown in the
Demographic and anthropometric characteristics did not
lumen of the intestinal tract. The systemic absorption of
differ signi®cantly between treatment groups both at the
orlistat is negligible and the potential for systemic adverse
start of the lead-in period or at the beginning of the trial.
events has been indicated as practically non-existent. Due tothe pharmacological mode of action of orlistat5 there is an
increased likelihood of gastrointestinal events. As pointed
Both groups A and B similarly had a signi®cant weight loss
out by SjostroÈm et al.2 the GI events were more common in
(P ` 0.01) that was also documented by a signi®cant
the orlistat-treated patients during the ®rst year of their
(P ` 0.01) variation in the BMI (Table 1). Considering the
collaborative multicenter trial, the frequency being lower
two periods of 30 days each, approximately 36.7% of the
during year 2 among participants who continued on orlistat
patients lost more than 2 kg each and 46.7% lost between 0.1
treatment. This has been interpreted as related to the fact
and 1.9 kg. The remaining 16.6% did not change their initial
that most patients would learn that orlistat treatment has to
weight or gained weight during the trial.
be associated with a moderate fat intake. During orlistattreatment the GI events are relatively important because itmay be cause for early withdrawal from the trial or cause
social embarrassment to the individual patient.
In Table 3, the meanÆ s.e.m. of the score of GI events
In order to circumvent the GI events that occur during
obtained for each patient is shown for both groups A and
orlistat treatment we have used the concomitant prescription
B. There was a signi®cant (P ` 0.01) difference between the
of psyllium hydrophilic mucilloid. Previous reports suggest
low prevalence of GI events, as indicated by the low score
that this natural ®ber may be effective in lowering serum
of GI events, when the patients were using psyllium
cholesterol,8,9 increasing the fecal excretion of bile acids11
hydrophillic mucilloid as compared with placebo. The
and absorbing free fat in the intestinal lumen.10 In this study
same results were obtained when groups A and B were
we were able to demonstrate that the adjunct use of psyllium
submitted after the washout period, respectively to placebo
with orlistat effectively diminished the number and seventy of
and psyllium. Overall, 71% of patients while on orlistat
GI events during orlistat therapy, as compared with placebo.
plus placebo had GI events as compared with 29% of
This was con®rmed when the psyllium-treated group was
patients while using orlistat and psyllium mucilloid.
switched to placebo and vice-versa. Therefore, we concluded
There was no statistical difference between meansÆ s.e.m.
that psyllium mucilloid had a protective action in the produc-
when orlistat and psyllium groups was compared with group
tion of GI events, most probably by absorbing free fat (oil) anddecreasing intestinal ¯atulence. Interestingly, most patientsindicated that the number of bowel movements did not
Table 4 Oily spotting, fecal urgency and incontinence. Comparison
increase in number while on orlistat plus psyllium. The most
between orlistat with psyllium or placeboa
important GI event that was prevented by the use of orlistat
plus psyllium was the embarrassing oily spot, de®ned as yellowdischarge with ¯atus during daily activities. Although psyllium
Oily spotting Fecal urgency Fecal incontinence
was not totally effective in preventing this situation, oily
spotting was 6-fold less frequent in the psyllium-treated
Finally we concluded that the use of psyllium as a single
Number of episodes during a 60 day trial of orlistat and psyllium or orlistat
dose of 12.0 g in water, at bedtime, is as effective as using
psyllium three times a day, at meals time. Most patients
3 Drent ML, Larsson I, William-Olsson T, Quaade F, Czubayko F,
considered that intake of psyllium at bedtime was far more
von Bergmann K, Strobel W, SjoÈstroÈm L, van der Veen EA.
Orlistat, a lipase inhibitor, in the treatment of human obesity: a
convenient and comfortable as compared to the alternate
multiple dose study. Int J Obes Relat Metab Disord l995; 19: 221±
In conclusion, psyllium hydrophilic mucilloid is an effec-
4 Davidson MH, Hauptman JB, Digirolamo M, Focyt JP, Halsted CH,
tive, practical and easy method to circumvent the GI events
Heber D, Heimburger DC, Lucas CP, Robbins DC, Chung J,
Heyms®eld SB. Weight control and risk factor reduction in
during orlistat treatment of obese patients, provided that a
obese subjects treated for 2 years with orlistat. JAMA 1999; 281:
5 Bray GA, Greenway FL. Current and potential drugs for treatment
of obesity. Endocr Rev 1999; 20: 805±875.
6 Hauptman J, Lucas C, Boldrin MN, Collins H, Segall KR. Orlistat
We acknowledge the help of Creusa R Dal Bo in the statistical
in the long-term treatment of obesity in primary care settings.
analysis of the data. This study was supported by Roche
Pharmaceutical Co. and Procter & Gamble (Brazil). The
7 Everson GT, Daggy BP, McKimley C, Story JA. Effects of psyllium
hydrophillic mucilloid on LDL-cholesterol and bile acid syn-
expert secretarial work of Maria Suzette Pott is gratefully
thesis in hypercholesterolemic men. J Lipid Res 1992; 33: 1183±
acknowledged. Part of this work was reported at the 9th
European Congress on Obesity, Milan, Italy (1999).
8 Levin EG, Miller VT, Muesing RA, Stoy DB, Balm tK, LaRosa JC.
Comparison of psyllium hydrophillic mucilloid and cellulose as
adjuncts to a prudent diet in the treatment of mild to moderate
hypercholesterolemia. Arch Intern Med 1990; 150: 1822±1827.
9 Bell LP, Hectorme K, Reynolds H, Balm TK, Hunninghake DB.
1 James WPT, Avenell A, Broom J, Whitehead J. A one year trial to
Cholesterol-lowering effects of psyllium hydrophilic mucilloid.
assess the value of orlistat in the management of obesity. Int J
Obes Relat Metab Disord 1997; 21(Suppl 3): S24±S30.
10 Vahouny GV, Krutchevsky M (eds). Dietary ®ber: basic and clinical
2 SjoÈstroÈm L, Rissanem A, Andersen T, Boldrin M, Golay A,
aspects. Plenum Press: New York; 1986. pp 181±209.
Koppeschaar HPF, Krempf M. Randomised placebo-controlled
11 Kesaniemi YA, Tarpila S, Miettinem L. Low vs. high dietary ®ber
trial of orlistat for weight loss and prevention of weight regain
and serum, biliary and fecal lipids in middle-aged men. Am J Clin
in obese patients. Lancet 1998; 352: 167±173.
Einstiege in die Frage nach dem Sch¨onenThese der Vorlesung: Das Sch¨one hat eine wichtigeFunktion im menschlichen Leben. Nebenthese: Unser Zeitalter hat sich dagegen ziem-lich blind gemacht. – ”technisches“ Denken;derMensch als Produzent – Die Erfahrung des Sch¨onen kann das Bewußt- sein unseres Zeitalters aufbrechen und sein phi-losophisches Vorurteil korrigieren. Das Chris
Traveller’s Diarrhea This fact sheet provides basic information only. It must not take the place of medical advice, diagnosis or treatment. Always talk to a healthcare professional about any health concerns you have, and before you make any changes to your diet, lifestyle or treatment. What is traveller's diarrhea? Traveller's diarrhea is frequent, loose, or watery bowel movements resulti
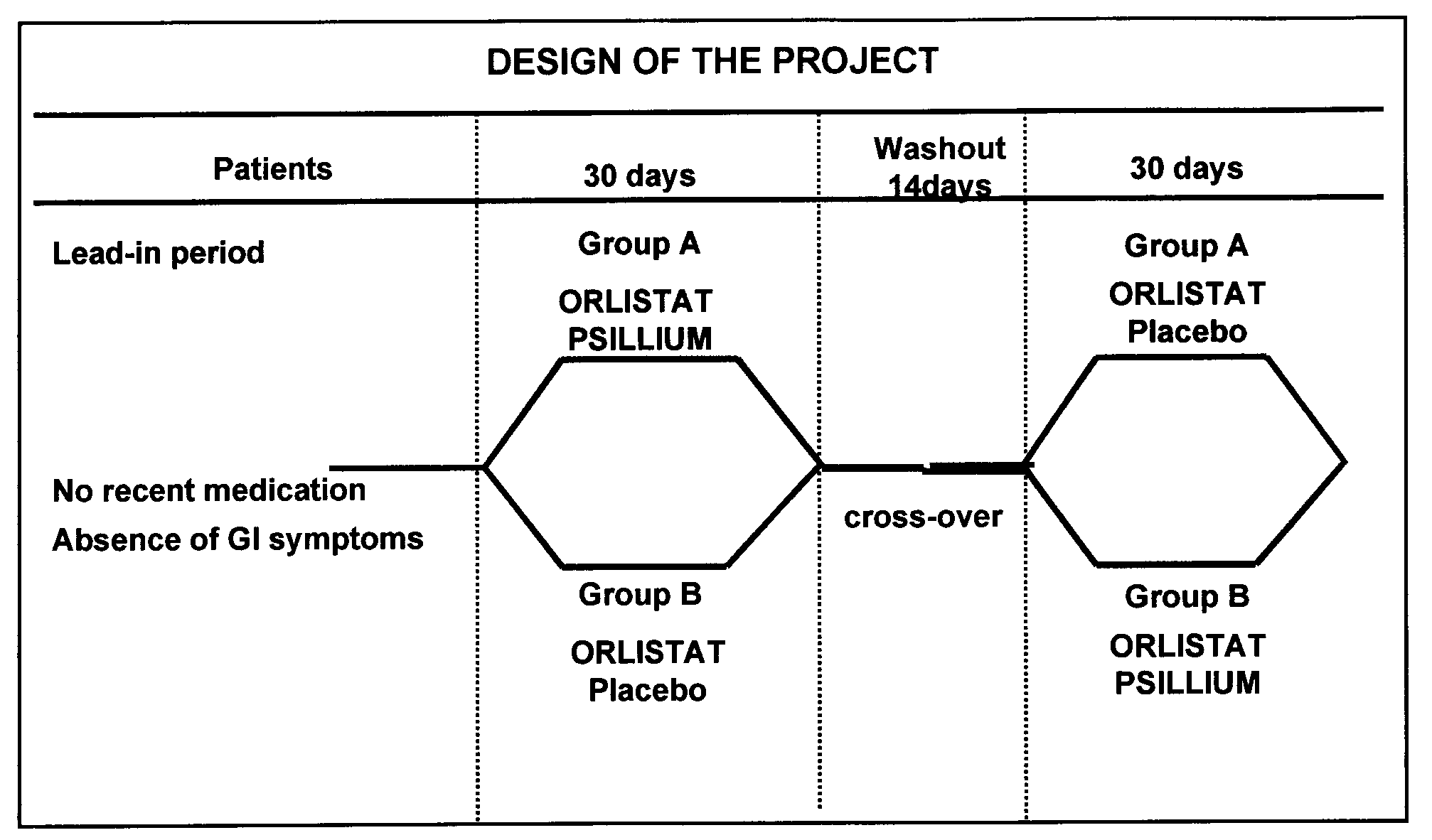 Figure 1 Schematic design of the research project.
Figure 1 Schematic design of the research project.