Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Layout
Randomized Placebo-Controlled Crossover Trial ofTadalafil in Raynaud’s Phenomenon Secondary toSystemic Sclerosis
ELENA SCHIOPU, VIVIEN M. HSU, ANN J. IMPENS, JENNIFER A. ROTHMAN, DEBORAH A. McCLOSKEY,JULIANNE E. WILSON, KRISTINE PHILLIPS, and JAMES R. SEIBOLD
ABSTRACT. Objective. Raynaud’s phenomenon (RP) is an important clinical feature of systemic sclerosis (SSc)
for which consistently effective therapies are lacking. The study was designed to assess the safety, tolerability, and efficacy of tadalafil, a selective, long acting type V cyclic GMP phosphodiesterase (PDE-5) inhibitor, in this clinical syndrome. Methods. We performed a prospective, randomized, double-blind, placebo-controlled, crossover study comparing oral tadalafil at a fixed dose of 20 mg daily for a period of 4 weeks versus place- bo in women with RP secondary to SSc. Results. Thirty-nine subjects completed the study and were evaluable. There were no statistically significant differences in Raynaud Condition Score (RCS), frequency of RP episodes, or duration of RP episodes between treatment groups. Placebo response was a confounding factor. Tadalafil was well tolerated. Conclusion. Tadalafil appears to be safe and well tolerated but lacks efficacy in comparison to placebo as a treatment for RP secondary to SSc. (First Release Sept 15 2009; J Rheumatol 2009;36:2264–8; doi:10.3899/jrheum.090270) Key Indexing Terms: RAYNAUD PHENOMENON SYSTEMIC SCLEROSIS TADALAFIL PDE-5 INHIBITOR
Raynaud’s phenomenon (RP) is an important clinical issue
tor of smooth muscle tone. Nitric oxide, a crucial mediator
in patients with systemic sclerosis (SSc) and significantly
of smooth muscle relaxation is produced by nitric oxide syn-
affects both function and quality of life. The mechanism of
thase. NO signals the conversion of GTP into cGMP and
RP secondary to SSc is complex and includes contributions
furthers intracellular accumulation of cGMP6. cGMP is bro-
from dysfunctional endothelium, abnormal smooth muscle
ken down by PDE-5. Inhibition of PDE-5 results in
cell responses, fixed luminal obstruction, local platelet acti-
increased available intracellular cGMP, which leads to
vation, and extravascular neuroregulation1. Vasoactive ther-
vasodilatation. There are 3 PDE-5 inhibitor compounds
apy of RP secondary to SSc is not uniformly effective, and
available: sildenafil, vardenafil, and tadalafil. Although
interventional clinical trials report variable results2-4.
most of the literature addresses their use in male erectile
Endothelial injury is a hallmark of SSc and is associated
dysfunction, experience with use in RP has been reported.
with reduced production of nitric oxide (NO)5. A diverse
Benefit from sildenafil in severe RP and digital ischemia has
body of evidence suggests that type V cyclic GMP phos-
been suggested in both case reports and series7,8. A 40
phodiesterase (PDE-5) has an important central role in
patient open label trial of vardenafil in RP9 and a
smooth muscle tone regulation. The cyclic nucleotide
double-blind, placebo-controlled, crossover trial of silde-
monophosphate cGMP is an important intracellular regula-
nafil in 18 patients with RP10 also describe improvement.
Tadalafil has a chemical structure that differs significant-
From the University of Michigan Scleroderma Program, Ann Arbor,
ly from sildenafil and vardenafil and has little activity against
Michigan, and University of Medicine and Dentistry of New Jersey
most of the other PDE isoenzymes. Tadalafil has a prolonged
Scleroderma Program, New Brunswick, New Jersey, USA.
mean terminal elimination half life (17.5 h) and efficacy last-
Supported by an unrestricted grant from Lilly ICOS, LLC.
ing up to 36 h, thus making chronic daily dosing practicable. E. Schiopu, MD, University of Michigan Scleroderma Program; V.M. Hsu,
Steady-state plasma concentration is achieved within 5 days
MD, UMDNJ Scleroderma Program; A.J. Impens, PhD, University ofMichigan Scleroderma Program; J.A. Rothman, MD; D.A. McCloskey,
of once daily dosing11. Another distinctive feature of
BSN; J.E. Wilson, RN, UMDNJ Scleroderma Program; K. Phillips, MD,
tadalafil is the fact that its pharmacokinetics are not affected
PhD; J.R. Seibold, MD, University of Michigan Scleroderma Program.
by food or alcohol intake, age, presence of diabetes, or mild
Address correspondence to Dr. J.R. Seibold, Professor & Director,
to moderate hepatic insufficiency6,12-16. University of Michigan Scleroderma Program, 24 Frank Lloyd WrightDrive, P. O. Box 481, Lobby M, Suite 2500, Ann Arbor, MI 48106-5753.
Our pilot trial was designed to test the efficacy and toler-
ability of once daily tadalafil in the treatment of RP second-
Accepted for publication May 26, 2009.
Personal non-commercial use only. The Journal of Rheumatology Copyright 2009. All rights reserved. The Journal of Rheumatology 2009; 36:10; doi:10.3899/jrheum.090270MATERIALS AND METHODS
monary hypertension, primary RP or RP secondary to a condition other
Study design. The primary objective of our study was to evaluate efficacy
than SSc, surgical sympathectomy involving the upper limb performed
and tolerability of tadalafil in women with RP secondary to SSc. The study
within the previous 12 months, participation in another study with an inves-
was a prospective, randomized, double-blind, placebo-controlled,
tigational drug or device during the 30 days prior to study entry, or during
crossover study evaluating oral tadalafil at a fixed dose of 20 mg daily for
the study, use of HIV protease inhibitors, ketoconazole or rifampin. Also,
a period of 4 weeks versus placebo in women with RP secondary to SSc.
the study excluded subjects who were pregnant or attempting to become
The sponsor of this pilot trial was primarily committed to investigation
pregnant before or during the study and subjects who were lactating or were
of the potential benefits of tadalafil in sexual dysfunction. Accordingly, this
< 6 months postpartum. All subjects of childbearing potential had to have
single center trial incorporated a co-primary outcome measure of possible
a negative pregnancy test result prior to enrollment. A woman of child-
effects on quality of female sexual function, which is reported separately17.
bearing potential was defined as a female who is biologically capable of
All the participants in our trial were hence women and were sufficiently
becoming pregnant. All women of childbearing potential in a heterosexual
healthy to agree to attempt sexual activity at least once weekly. The 20 mg
relationship had to agree to practice a medically acceptable form of contra-
daily dose of tadalafil was chosen based on sponsor data from other trials
All study patients were required to discontinue certain prespecified
Enrollment began in October to permit study during cold weather
concomitant medications before starting the 2-week pretreatment period.
months; however, the last enrolled subject exited in June of the following
These medications included drugs used in the treatment of RP [e.g., calci-
year. The potential for influence of variable weather was examined by com-
um channel blockers (CCB), other PDE-5 inhibitors, sympatholytic drugs,
paring results for patients starting the study in October-November with
arginine, papaverine, nitrates, nitrites and other vasodilators]. CCB and
those enrolling during the months of February-March.
angiotensin converting enzyme inhibitors (ACEI) being used for the treat-
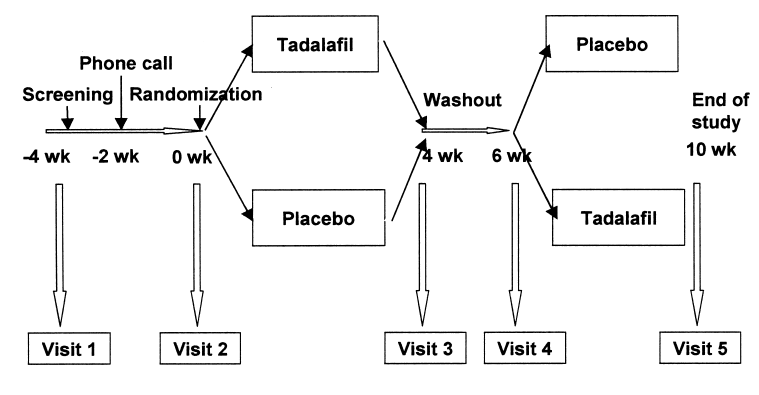
There were a total of 5 study visits: 1 screening visit (Visit 1), 3 inter-
ment of conditions other than RP could be continued at the same dose if the
mediate visits (Visits 2, 3 and 4), and an exit visit (Visit 5) (Figure 1).
patient was stabilized on the drug. Hypertension developing during the
During the screening visit (Visit 1) subjects signed informed consent and
study could be treated with ACEI and/or diuretics. Drug therapies for the
were instructed on the use of paper diaries to record daily Raynaud
underlying disease, SSc (e.g., methotrexate), could be continued if the
Condition Score (RCS)18, duration and frequency of RP attacks. At 2 weeks
patient was already receiving them, but new treatment was not allowed dur-
prior to randomization subjects received a phone call to reinforce appropri-
ing the study. Medications specifically prescribed for psychoses, bipolar
ate use of RP diaries. The total duration of the run-in period (between
disorder, and depression were prohibited. Cyclosporine was specifically
screening and randomization) was 2 weeks. At Week 0, subjects who
prohibited. Palliative therapies (e.g., nonsteroidal antiinflammatory drugs,
recorded at least 6 RP attacks per week during the run-in period were ran-
proton pump inhibitors) were continued. If a patient had been receiving any
domized to a uniform dose of 20 mg of tadalafil or matching placebo and
other medication for some period of time prior to the commencement of the
entered the first 4-week treatment block. This was followed by a 2 week
study, as a matter of necessity for the treatment of a medical condition, then
washout period and then by 4 weeks of crossover therapy.
the medication was permitted for the duration of the study, based on the
Our study was approved by the UMDNJ-Robert Wood Johnson
judgment of the investigator. If a subject withdrew or was dismissed from
Medical School Institutional Board for Human Studies.
the study after any use of the study medication, the exit procedures of the
Subjects. All patients fulfilled the American College of Rheumatology
last visit (Visit 5) were implemented. Withdrawn or dismissed patients were
(ACR; formerly, the American Rheumatism Association) classification cri-
replaced as needed to assure full numbers of completed patients.
teria for SSc19. To be eligible, patients had to be at least 18 years old, be
Treatment regimen. Patients were assigned at random to receive either
able to sign informed consent, and have documented evidence of at least 6
active treatment with a fixed dose of 20 mg of tadalafil or matching place-
RP attacks per week during the 2-week pre-treatment period. Exclusion cri-
bo daily for 4 weeks, followed by a 2-week washout period, followed by
teria included the following: active smoking status, clinically significant
another 4 weeks of crossover therapy.
evidence of hepatobiliary disease, serum creatinine > 1.8 mg/dl, history of
Outcome measures. The primary measure of outcome was efficacy of
myocardial infarction within the previous 6 months, unstable angina, con-
tadalafil for RP. The chosen measures of efficacy were RCS18, duration and
gestive heart failure of any etiology, current chronic or intermittent use of
frequency of RP attacks as recorded in a paper diary by the patient. Patients
nitrates or nitrites for angina pectoris or any other condition, significant
were instructed to record every RP episode along with the time (min) that
central nervous system diseases within the last 6 months (stroke, spinal
the attack lasted. At the end of each day, patients completed the RCS, a
cord injury, etc.), World Health Organization (WHO) Class III or IV pul-
10-cm visual analog scale, which is a validated measure of the overall
Personal non-commercial use only. The Journal of Rheumatology Copyright 2009. All rights reserved.
effect of the RP (including frequency, severity, effect on activities of daily
Table 1. Baseline characteristics of the study patients.
living)18. These measures were obtained weekly during the 2-week pre-treatment block and during the 2 4-week treatment blocks. The diaries were
collected at each visit. Measures of efficacy were reported as mean changefrom the baseline. The average RCS was calculated as the arithmetic mean
of the daily scores for every given interval. The average daily duration of
RP attacks was calculated by dividing the total duration of the attacks dur-
ing a given interval by the number of diary days. Similarly, the average
daily number of attacks was calculated by dividing the total number of RP
attacks by the number of diary days for a certain interval. Digital tip
ischemic ulcerations were followed as a secondary outcome measure.
Quality of female sexual function was a co-primary outcome; hence, all
patients were sexually active women sufficiently well to attempt sexual
activity at least once per week. Safety and tolerability of tadalafil were
assessed by monitoring adverse events (AE) and severe adverse events
(SAE), changes in vital signs, clinical laboratory tests (complete blood
count, serum chemistry, urinalysis, and urine pregnancy test), electrocar-diogram, and examination at each study visit. The incidence of study-emer-
SSc: systemic sclerosis; RP: Raynaud's phenomenon; RCS: Raynaud
gent AE was tabulated by treatment group, event, and body system. Events
occurring between Visit 3 and 4 (washout period) were summarized withthe treatment received at Visit 2. Statistical analysis. The primary analysis was performed on all patients that
Table 2. Concomitant medications.
completed the study. Measures of efficacy are reported as mean changefrom the baseline. The paired sample t-test was used to compare the inter-
vention to the placebo group, using a significance level of 0.05. The infor-
mation about the sample size was based on data from a 2-group, parallel,placebo-controlled trial of oral iloprost for treatment of RP in patients with
SSc20. A sample size of 40 patients would provide 88% power to detect a
15% difference between placebo and tadalafil in the percent change from
baseline RCS at a 0.05 level of significance. It was envisaged that 40 sub-
jects would be enrolled in the study, but 45 patients signed consent to assure
the number of evaluable cases at study completion. All data management
and statistical analysis were performed with SPSS for Windows 16.0 (SPSS
Inc., Chicago, IL). The overall incidence rates of AE were comparedbetween treatments using Pearson’s chi-squared tests. There was no sub-
CCB: calcium channel blockers; ACEI: angiotensin converting enzyme
inhibitor; ARB: angiotensin receptor blocker; ERT: estrogen replacementtherapy; SSRI: selective serotonin reuptake inhibitor. RESULTS Characteristics of the study subjects. Of the 45 patients who
were the most frequently discontinued agents during the
signed consent, 39 completed the study. Three of the
patients who signed consent had fewer than 6 RP episodes
Study-specified measures of efficacy for RP are present-
per week during the 2 week run-in period between Visit 1
ed in Table 3. There were trends to improvement during this
and Visit 2 and were considered ineligible. Three other
trial in RCS, RP frequency, and RP duration which were
patients were discontinued during the first treatment period
unrelated to treatment. All differences were not significant.
due to noncompliance with the protocol (1 subject) and
We performed several post hoc analyses of potential con-
investigator’s discretion due to labile clinical circumstances
founding effects. There was no period effect — specifically
(2 subjects). Thus, 39 patients receiving tadalafil or placebo
no differences in change of RCS either in comparison to
were evaluated and fulfilled all visits required for full pro-
baseline or between treatment arms for patients randomized
to receive active drug first or to receive placebo first. There
The final study population consisted of 39 women with a
was no detectable relationship to environmental temperature
mean age of 52.9 [standard deviation (SD) 10.6; range
during the conduct of this study. This is not surprising.
40.3-63.3] (Table 1). Subjects were mostly Caucasian, and
Although our study enrolled between October and April, any
75% were classified as having limited SSc (Table 1). The
given subject completed participation within 10 weeks and
mean RP duration prior to enrolling in the study was 12
did not bridge between very cold and very warm weather.
years (SD 10 yrs). The frequency of RP attacks and the
There were no differences in RCS either in terms of absolute
mean RCS at baseline were comparable to previous large
values or in terms of change from baseline between subjects
randomized clinical trials in RP3,20,21.
studied in October through November versus February
Table 2 illustrates the use of concomitant medications
through March. In this patient population, there were too
before and after the initiation of the trial. Calcium channel
few digital ulcers to permit analysis of healing or preven-
blockers (CCB) and selective serotonin reuptake inhibitors
tion. Two subjects had a single digital ulcer at entry, which
Personal non-commercial use only. The Journal of Rheumatology Copyright 2009. All rights reserved. The Journal of Rheumatology 2009; 36:10; doi:10.3899/jrheum.090270Table 3. Results of the mean RCS, mean RP frequency, and mean RP duration in a crossover trial of tadalafil inRP secondary to SSc.
RCS: Raynaud Condition Score; RP: Raynaud Phenomenon; NS: not significant.
was still present at the exit visit. No physiologic measures of
and idiopathic pulmonary arterial hypertension (PAH)24.
digital perfusion were included in this trial.
Tadalafil is highly selective for the pulmonary circulation
Safety and tolerability. No SAE were reported for the dura-
and has a longer lasting effect of all available PDE-5
tion of our study. The most frequently encountered AE dur-
inhibitors on lung and systemic hemodynamics in PAH25.
ing the treatment phase were headache, back pain, fluid
There are several limitations to our study. Our subjects
retention, and vasomotor changes (Table 4). The common
had a mean disease duration of 12 years which is longer than
AE were similar in the placebo and tadalafil group. Back
the average 8-9 years reported in other RP trials3,20. It has
pain was reported more frequently in the treatment group
been noted that severity of RP tends to increase with disease
but this is a well known, idiosyncratic side effect of PDE-5
duration which may be due to cumulative intimal damage
inhibitors. Overall, tadalafil at 20 mg daily was well tolerat-
over time. Our study sample might thus be less likely to note
ed among all the study subjects who received the active
a measurable difference when exposed to a drug in which
drug, with the majority of reported AE being mild to mod-
actions are largely dependent on endothelial integrity.
erate in intensity and with the exception of back pain,
However, all our subjects were sufficiently healthy to vol-
judged unrelated to the treatment. Measurements of vital
unteer as sexually active women and only 2 had active dig-
signs, physical findings, electrocardiograms, and laboratory
ital ischemic ulcers. If our study reflected a selection bias,
measures were not different between the treatment and the
we speculate that we were enriched for patients with gener-
With a sample size of 39 patients, our study has 88%
DISCUSSION
power to detect a 15% treatment effect. Placebo effect,
We were not able to demonstrate evidence of efficacy of
reported in previous large RP trials to be as high as 46%20,
tadalafil by any of our clinical measures of RP. These out-
remains a prominent issue in RP secondary to SSc trial
come measures included duration of daily attacks, frequen-
design. Previous studies in RP secondary to SSc have been
cy of RP recorded in a diary, and RP severity as measured
limited by lack of adequate assessment tools that are sensi-
by a patient-completed daily RCS. While all measures
tive to change over the time course of a short clinical trial.
showed improvement, there were no statistical differences
The RCS is the only measure that has been validated.
between placebo and tadalafil in any of these variables. At
Although uniformly used in RP trials, diary collection of RP
the dose used for the duration of this study (20 mg daily),
information is likely to introduce a recall bias and to be an
tadalafil was associated with no severe adverse events. The
inaccurate method of assessing the exact status and severity
of the peripheral circulation. In the large trial of oral iloprost
Tadalafil was reported to increase blood flow and reduce
(308 subjects), mean RCS at entry was 4.21–4.35 units
symptoms in a single case of secondary RP not responding
(comparable to that of our study population20. Drug and
to sildenafil22. Effects of tadalafil on the pulmonary circula-
placebo response were 1.32 and 1.00 units respectively —
tion are described in both high-altitude pulmonary edema23
again an effect comparable to our study (Table 3).
A similar crossover trial of tadalafil 20 mg every other
Table 4. Summary of adverse events in 39 subjects with SSc.
day versus placebo has been reported in abstract and showedsignificant improvement in the mean daily frequency and
duration of RP and in the mean daily RCS26. The mean ageof the subjects in this latter trial was lower than the mean
age in our subjects (36.71 vs 52.9), and the study design
allowed continuation of established therapies for RP (24 of
24 continued CCB; 18 of 24 participants also continued
ACE inhibitors and angiotensin receptor blockers). The
magnitude of change on active therapy of mean RCS, RP
duration and frequency between baseline and treatment was
Personal non-commercial use only. The Journal of Rheumatology Copyright 2009. All rights reserved.
similar to our study. However, placebo response was notably
9. Caglayan E, Huntgeburth M, Karasch T, Weihrauch J, Hunzelmann
absent — a surprising finding for which we offer no
N, Krieg T, et al. Phosphodiesterase type 5 inhibition is a noveltherapeutic option in Raynaud disease. Arch Intern Med
Our study did not permit inclusion of physiologic meas-
10. Fries R, Shariat K, von Wilmowsky H, Bohm M. Sildenafil in the
ures of the digital blood flow in response to tadalafil daily.
treatment of Raynaud’s phenomenon resistant to vasodilatory
Peripheral vascular response to PDE-5 inhibitors has been
therapy. Circulation 2005;119:2980-5.
assessed objectively. One study reported a 400% increase in
11. Porst H. Phosphodiesterase type-5 inhibitors: a critical comparative
analysis. EAU Update Series 2004;2:56-63.
capillary blood flow velocity assessed by laser Doppler
12. Rosen R, Kotsis J. Overview of phosphodiesterase 5 inhibition in
anemometry after 4 weeks of sildenafil10 and another report-
erectile dysfunction. Am J Cardiol 2003;92 Suppl:9M-18M.
ed an increase of 9.9% in blood flow using laser Doppler
13. Sung B, Hwang K, Jeon Y, Lee J, Heo Y, Kim J, et al. Structure of
flowmetry in an open label trial using vardenafil9. However,
the catalytic domain of human phosphodiesterase 5 with bound
a recent study of 20 patients with RP (including only 1 sub-
drug molecules. Nature 2003;425:98-102.
14. Boin F, Wigley F. Understanding, assessing and treating Raynaud’s
ject with RP secondary to SSc) who received a single dose
phenomenon. Curr Opin Rheumatol 2005;17(6):752-60.
of 10 mg of tadalafil had digital blood flow measured by
15. Wright P. Comparison of phosphodiesterase type 5 (PDE5)
laser Doppler flowmetry at rest and during 2 heat and cold
inhibitors. Int J Clin Pract 2006;60:967-75.
exposure cycles27. Tadalafil had no measurable effect on
16. Forgue S, Phillips D, Bedding A, Payne C, Jewell H, Patterson B,
digital blood flow at baseline, during heating or in response
et al. Effects of gender, age, diabetes mellitus and renal and hepaticimpairment on tadalafil pharmacokinetics. Brit J Clin Pharmacol
to cold exposure. The physiological response or lack there-
of to chronic daily use of tadalafil has not yet been studied
17. Impens AJ, Rothman J, Schiopu E, Cole JC, Dang J, Gendrano N,
et al. Sexual activity and functioning in female scleroderma
Other studies have suggested that treatment with
patients. Clin Exp Rheumatol 2009; Suppl 54: [in press].
vasodilators of RP secondary to SSc may not benefit all
18. Merkel PA, Herlyn K, Martin RW, Anderson JJ, Mayes MD, Bell P,
et al. Measuring disease activity and functional status in patients
patients, possibly due to the relative contribution of fixed
with scleroderma and Raynaud’s phenomenon. Arthritis Rheum
changes related to the underlying SSc vasculopathy.
Additional larger studies are needed to identify a subgroup
19. Subcommittee for Scleroderma Criteria of the American
for which PDE-5 inhibitors may be beneficial or to assess
Rheumatism Association Diagnostic and Therapeutic Criteria
whether or not there is therapeutic efficacy associated with
Committee. Preliminary criteria for the classification of systemicsclerosis (scleroderma). Arthritis Rheum 1980;23:581-90.
specific agents within this class. In conclusion, the results of
20. Wigley F, Korn J, Csuka M, Medsger TJ, Rothfield N, Ellman M, et
our study do not support the use of tadalafil as a therapy for
al. Oral iloprost treatment in patients with Raynaud’s phenomenon
RP secondary to SSc at a dose of 20 mg daily. Placebo
secondary to systemic sclerosis: a multicenter, placebo-controlled,
response continues to be a significant limitation in RP trials.
double-blind study. Arthritis Rheum 1998;41:670-7.
21. Gliddon A, Doré C, Black C, McHugh N, Moots R, Denton C, et al.
Prevention of vascular damage in scleroderma and autoimmune
REFERENCES
Raynaud’s phenomenon: a multicenter, randomized, double-blind,
1. Herrick A. Pathogenesis of Raynaud’s phenomenon. Rheumatology
placebo-controlled trial of the angiotensin-converting enzyme
inhibitor quinapril. Arthritis Rheum 2007;56:3837-46.
2. Thompson A, Shea B, Welch V, Fenlon D, Pope J. Calcium-channel
22. Baumhaekel M, Scheffler P, Boehm M. Use of tadalafil in a patient
blockers for Raynaud’s phenomenon in systemic sclerosis. Arthritis
with a secondary Raynaud’s phenomenon not responding to
sildenafil. Microvascular Res 2005;69:178-9.
3. Dziadzio M, Denton C, Smith R, Howell K, Blann A, Bowers E, et
23. Maggiorini M, Brunner-La Roca H, Peth S, Fischler M, Bohm T,
al. Losartan therapy for Raynaud’s phenomenon and scleroderma:
Bernheim A, et al. Both tadalafil and dexamethasone may reduce
clinical and biochemical findings in a fifteen-week, randomized,
the incidence of high-altitude pulmonary edema: a randomized trial.
parallel-group, controlled trial. Arthritis Rheum 1999;42:2646-55.
4. Pope J, Fenlon D, Thompson A, Shea B, Furst D, Wells G, et al.
24. Affuso F, Palmieri E, Di Conza P, Guardasole V, Fazio S. Tadalafil
Iloprost and cisaprost for Raynaud’s phenomenon in progressive
improves quality of life and exercise tolerance in idiopathic
systemic sclerosis. Cochrane Database Syst Rev
pulmonary arterial hypertension. Int J Cardiol 2006;108:429-31.
25. Ghofrani H, Voswinckel R, Reichenberger F, Olschewski H,
5. Kahaleh B. Vascular disease in scleroderma: mechanisms of
Haredza P, Karadas B, et al. Differences in hemodynamic and
vascular injury. Rheum Dis Clin North Am 2008;34:57-71.
oxygenation responses to three different phosphodiesterase-5
6. Uckert S, Hedlund P, Andersson K, Truss M, Jonas U, Stief C.
inhibitors in patients with pulmonary arterial hypertension: a
Update on phosphodiesterase (PDE) isoenzymes as pharmacologic
randomized prospective study. J Am Coll Cardiol 2004;44:1488-96.
targets in urology: present and future. Eur Urol 2006;50:1194-207.
26. Shenoy P, Agarwal V, Kumar S, Choudhary SK, Jha LK, Singh U,
7. Colglazier C, Sutej P, O’Rourke K. Severe refractory fingertip
Misra R. Efficacy of tadalafil in secondary Raynaud’s phenomenon
ulcerations in a patient with scleroderma: successful treatment with
resistant to vasodilator therapy: a double blind randomized cross
sildenafil. J Rheumatol 2005;32:2440-2.
over trial [abstract]. Arthritis Rheum 2008;58 Suppl:s402.
8. Gore J, Silver R. Oral sildenafil for the treatment of Raynaud’s
27. Friedman EA, Harris PA, Wood AJJ, Stein CM, Kurnik D. The
phenomenon and digital ulcers secondary to systemic sclerosis. Ann
effects of tadalafil on cold-induced vasoconstriction in patients with
Raynaud’s phenomenon. Clin Pharmacol Ther 2007;81:503-9.
Personal non-commercial use only. The Journal of Rheumatology Copyright 2009. All rights reserved. The Journal of Rheumatology 2009; 36:10; doi:10.3899/jrheum.090270
Procedure # : 032 Effective : Hiring Process Section : Page : 1 of 4 Review Operating Guidelines Statement Student Transportation Services Brant Haldimand Norfolk (STSBHN) endeavours to hire the most qualified candidates for positions that become available within the organization. STSBHN is an equal opportunity employer. Hiring for all unionized employees, if any e
INTRODUCTION . 274 I. THE EXISTENCE OF INEQUALS . 276 II. INTRODUCING A PATENT REGIME IN INDIA. 278 A. The Background . 278 B. Towards an Indian Patent Policy . 281 1. Patents and Underdeveloped Nations . 282 2. Inventions Relating to Chemicals, Food, and Pharmaceuticals. 283 3. Industrialization. 286 III. ESTABLISHING AN INDIAN PATENT REGIME . 289 A. Indian Patent Legislation . 289 1.
 MATERIALS AND METHODS
MATERIALS AND METHODS