Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Nichemedical.net.au
ARTICLE IN PRESS
The Journal of Emergency Medicine, Vol. xx, No. x, pp. xxx, 2009
Copyright 2009 Published by Elsevier Inc. doi:10.1016/j.jemermed.2008.06.029 Original Contributions EFFICACY AND COST COMPARISONS OF BRONCHODILATATOR ADMINISTRATION BETWEEN METERED DOSE INHALERS WITH DISPOSABLE SPACERS AND NEBULIZERS FOR ACUTE ASTHMA IN AN INNER-CITY ADULT POPULATION
Sunil Dhuper, MD,*†‡ Alpana Chandra, MD,*†‡ Aziz Ahmed, MD,*†‡ Sabin Bista, MD,†
Ajit Moghekar, MD,† Rajesh Verma, MD,*†‡ Cynthia Chong, MD,*†‡ Chang Shim, MD,†‡
Hillel Cohen, DRPH,‡ and Sonia Choksi, MD*†‡
*North Central Bronx Hospital, Bronx, New York, †Jacobi Medical Center, Bronx, New York, and ‡Albert Einstein College of Medicine,
Reprint Address: Sunil Dhuper, MD, Coney Island Hospital, 2601 Ocean Parkway, 2w6, Brooklyn, NY 11229
e Abstract—Background: demonstration nebulizer groups, respectively (p ؍ 0.56). The median im- equivalent efficacy of beta agonist delivery using a metered provement in the symptom score was 7 (5–9) vs. 7 (4 –9) in dose inhaler (MDI) with spacer vs. nebulizer in asthma the spacer and nebulizer groups, respectively (p ؍ 0.78). patients, use of a nebulizer remains standard practice. Ob- The median cost of treatment per patient was $10.11 jectives: We hypothesize that beta agonist delivery with a ($10.03–$10.28) vs. $18.26 ($9.88 –$22.45) in the spacer and MDI/disposable spacer combination is an effective and low- nebulizer groups, respectively (p < 0.001). Conclusion: cost alternative to nebulizer delivery for acute asthma in an There is no evidence of superiority of nebulizer to MDI/ inner-city population. Methods: This study was a prospec- spacer beta agonist delivery for emergency management of tive, randomized, double-blinded, placebo-controlled trial acute asthma in the inner-city adult population. MDI/ with 60 acute asthma adult patients in two inner-city emer- spacer may be a more economical alternative to nebulizer gency departments. Subjects (n ؍ 60) received albuterol delivery. 2009 Published by Elsevier Inc. with either a MDI/spacer combination or nebulizer. The spacer group (n ؍ 29) received albuterol by MDI/spacer
e Keywords—spacer; metered dose inhaler; MDI; asthma; followed by placebo nebulization. The nebulizer group (n ؍ nebulizer; emergency department; inner city 29) received placebo by MDI/spacer followed by albuterol nebulization. Peak flows, symptom scores, and need for rescue bronchodilatator were monitored. Median values INTRODUCTION were compared with the Kolmogorov-Smirnov test. Re- sults: Patients in the two randomized groups had similar
Asthma affects approximately 14 million adult Ameri-
baseline characteristics. The severity of asthma exacerba- tion, median peak flows, and symptom scores were not
cans and accounts for more than 450,000 hospitalizations
significantly different between the two groups. The median
annually. Approximately 1.8 million asthma patients re-
(interquartile range) improvement in peak flow was 120
quire emergency department (ED) visits each year. Rates
(75–180) L/min vs. 120 (80 –155) L/min in the spacer and
of hospitalizations and ED visits related to asthma aregreatest in the Northeast, especially in New York City.
This study was funded by a grant from Thayer Medical
Among New York City’s five boroughs, the two eco-
nomically depressed areas of the Bronx and Brooklyn
RECEIVED: 2 October 2007; FINAL SUBMISSION RECEIVED: 30 May 2008;ACCEPTED: 22 June 2008
ARTICLE IN PRESS
boroughs had the highest hospitalization rates of 75 and
tient settings. Although some have been done in the ED
52 per 10,000, respectively. Economically disadvantaged
setting, to our knowledge, none has focused on an inner-
inner-city adults, particularly the African-American and
city adult patient population who most frequently use the
Hispanic populations, are more susceptible The
ED as a primary source of asthma care.
ethnic differences in prevalence, morbidity, and mortal-
We hypothesized that albuterol delivered with a dis-
ity, along with frequent hospitalizations and ED visits,
posable spacer would be an efficient, cost-effective al-
are highly correlated with poverty and inadequate access
ternative to nebulized albuterol treatment for inner-city
to medical care. Other factors that may play a role
adult asthma patients presenting to the ED.
include urban air quality, indoor allergens, scarcity ofpatient education programs that are culturally and lin-guistically appropriate, and lack of self-management
Because the inner-city patient population tends to
The study was approved by the Committee of Clinical
frequently use the ED rather than a primary physician as
Investigations. It was conducted as a prospective, ran-
the primary source of asthma care, management strate-
domized, double-blinded, placebo-controlled trial in
gies in the ED should be appropriately designed, with the
adult patients with acute asthma presenting to the EDs of
clinical effectiveness, efficiency, and economics being
two acute-care inner-city teaching hospitals (total ED
taken into consideration Patients with acute asthma
visits approximately 88,000/year) in the borough of the
are usually treated with nebulized albuterol in the ED
and in the inpatient setting after admission. An albuterolmetered dose inhaler (MDI) with a spacer can be usedalternatively, allowing the patient to inhale aerosol from
the MDI without the need to coordinate the actuation ofMDI and inhalation, a step many patients have difficulty
Patients who presented to the ED with acute exacerba-
tion of asthma as defined in the NAEPP (National
The MDI/spacer combination has been evaluated in
Asthma Education and Prevention Program) Expert
adults with mild, moderate, and severe acute asthma in
Panel Report II were eligible to participate in the study if
various settings, including the outpatient department,
they met the following criteria: 1) diagnosis of asthma, 2)
inpatient ward, ED, and intensive care settings
age 18 –70 years, and 3) ability to perform peak flow
Although greater bronchodilatator response might be ex-
maneuvers with good effort Patients were excluded
pected with a nebulizer due to the higher dose used for
for any of the following reasons: 1) requiring intubation
nebulization compared with standard measured-dose in-
and mechanical ventilation, 2) smoking history Ͼ 20
halers, studies comparing delivery of beta agonist with
pack years, and 3) the presence of coexistent systemic
MDI plus a spacer vs. a nebulizer show no difference
diseases such as congestive heart failure, pulmonary
with respect to clinical response in acute severe asthma
disease other than asthma such as pneumonia, tubercu-
and stable chronic asthma In addition, extra-
losis, bronchiectasis, interstitial lung disease, sarcoid-
pulmonary sympathetic effects such as tremor, anxiety,
osis, pleural diseases, kyphoscoliosis, chronic obstruc-
and dysrhythmias were found in one study to be more
tive pulmonary disease, renal failure, or cancer.
prevalent in patients receiving nebulized medication
All patients who met the eligibility criteria and signed
compared to MDI/spacer-delivered medication Al-
the informed written consent were enrolled.
buterol administered by a spacer and MDI, therefore, isan effective alternative to a nebulizer
Despite the demonstrated equivalency, rapid delivery,
and lesser use of personnel resources with the MDI/spacer combination, nebulized albuterol remains the
Patients were recruited for the study from August 2004
standard therapy for patients with acute asthma
to August 2005 and were randomly assigned to the study
Patients’ perception of the nebulizer being more effec-
group (MDI/disposable spacer combination) or control
tive, the lack of coordination between MDI actuation and
group (Nebulizer). Patients were enrolled 24 h a day by
inhalation when using an MDI/spacer during acute
either the investigators or housestaff specifically trained
asthma, especially for first time users, and the notion that
by the investigators, who were responsible for maintain-
delivery with non-disposable commercial spacers is
ing the study records. Randomization codes were se-
more expensive, has limited the use of spacers in the ED.
lected by a pharmacist who was not involved in the
Most studies comparing the two modes of delivery in
study, using a randomization table with a block size of
adults have been conducted in the ambulatory and inpa-
four. Codes for the study groups were known only to the
ARTICLE IN PRESS
pharmacist. All personnel involved in patient recruitment
decreasing score indicated improvement. Both groups
and medication delivery were blinded to the randomiza-
were followed for their expiratory peak flow, symptom
tion. A disposable and collapsible, dual-valve holding
severity, and the number of rescue bronchodilatator treat-
chamber for use with MDI LiteAire (Thayer Medical,
ments every hour for a maximum of 6 h. The triage
Tucson, AZ) was utilized for the study. Placebo MDIs
decision to admit or discharge a patient from the ED was
were prepared by a pharmacist who was not involved in
made within 6 h of enrollment into the study, and the
the study or in the assignment of randomization codes.
study was terminated once the patient was discharged
All patients received treatment with the MDI/spacer
home or admitted to the hospital. Patients were dis-
combination and nebulizer. The MDI/spacer group re-
charged home after ED treatment based on the improve-
ceived 540 g of chloroflourocarbon (CFC) albuterol by
ment in the underlying disease severity as assessed by
MDI (six actuations of 90 g/actuation; Warwick Phar-
the peak flow. The discharge criterion was peak flow
maceutical Corporation, Reno, NV) with the spacer fol-
rates Ͼ 70% predicted Patients were discharged home
lowed by 3 mL of normal saline solution (0.9%) by
with specific therapy based on NAEPP guidelines
nebulizer every hour until disposition. The Nebulizergroup received six actuations of placebo MDI withspacer followed by 2.5 mg (3 cc) albuterol (Dey, Napa,
CA) by nebulizer (Cardinal Health Edison, NJ) on asimilar schedule. MDI was shaken before each actuation
The primary outcomes measured were changes in pa-
and medication was administered one actuation at a time
tients’ symptoms and peak flow rates, and disposition
into the spacer. Each actuation was delivered just before
(i.e., admission to hospital or discharge to home from the
inhalation and the aerosol was inhaled from the spacer by
ED). Secondary outcome measures were length of stay in
six tidal breaths. All MDI/spacer treatments were self
the ED, cost of therapy, and the number of rescue treat-
administered by the patient after a one-time demonstra-
ments required. The length of stay was calculated from
tion of its use by a respiratory therapist (RT). All nebu-
the time of enrollment into the study until the time the
lizer treatments were administered by a RT in the asthma
decision was made regarding the patient’s disposition. In
treatment room in the ED. The RT documented in the
the case of patients whose stay in the ED was prolonged
electronic medical chart the vital signs, room air oxygen
for reasons other than medical, the time of disposition
saturation, lung examination, and a pre- and post-treat-
was taken as the time they met the criteria for admission
ment peak flow rate for every treatment administered.
to the medical ward or discharge home. Cost analysis for
The RT managing the patient care was supervised by the
each group included the cost of medication, equipment
emergency physician on duty. Patients also received
(spacer vs. nebulizer kit), and labor (time spent by the
rescue treatments with albuterol nebulization as required.
respiratory therapists, for the active medication only). The cost of placebo medication, the device to deliver
Oral or intravenous steroids were administered at the
placebo, and the labor to administer it were excluded
discretion of the emergency physician.
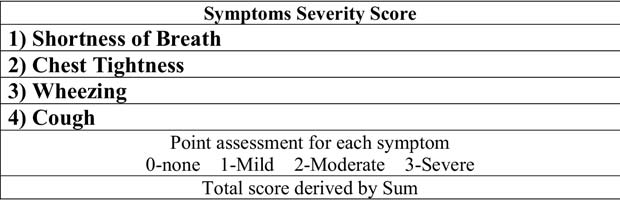
A baseline peak flow measured by a Wright peak flow
meter and a “symptom severity score” were recorded foreach patient at the start of the study, and every hour until
disposition. Based on each patient’s perception of sever-ity of symptoms, a score of 0 –3 was assigned, each for
Insofar as we did not have an a priori estimate of an
shortness of breath, chest tightness, wheezing, and cough
effect size difference with which to project a sample size,
(0 for none, 1 for mild, 2 for moderate, 3 for severe), and
we undertook to enroll as many eligible consecutive
a total score was calculated as the sum of each individual
participants as possible within the 1-year enrollment
period for the study. Entry characteristics between the
score reflected a greater severity of symptoms and a
two treatment groups were compared to assess whetherthe randomization achieved a reasonable balance. p Val-ues are provided as a guide to this assessment with theunderstanding that the formal interpretation of p is notapplicable to random assignment. Categorical variablesare presented as percentages and compared with chi-squared. Continuous variables within each of the studygroups did not meet normality assumptions. Values arepresented as median (interquartile range [IQR]) and
Figure 1. Symptom severity score.
between-group comparisons made with the non-parametric
ARTICLE IN PRESS Table 1. Baseline Characteristics
* Analysis of continuous variables (presented as median and interquartile range) by the non-parametric Kolmogorov-Smirnov test andcategorical variables (presented as % by chi-square). Treatment group was by random allocation, so that both groups came from thesame population. Thus, p values have been given only as a convenient gauge of the effectiveness of the randomization and should notto be given a formal interpretation.
Kolmogorov-Smirnov test. Normality assumptions were
the Nebulizer group (97% vs. 93%, respectively) were
met sufficiently for the sample as a whole to allow linear
discharged home at the completion of the study
regression models to assess potential confounding. All
Medians (IQR) for increase in peak flow from entry to
tests used a two-tailed alpha of 0.05 for statistical sig-
disposition were similar for the two groups, with 120
nificance, and analyses were performed with SPSS for
(75–180) L/min for the MDI/spacer group and 120 (80 –
Windows software (version 13; SPSS Inc., Chicago, IL).
155) L/min for the Nebulizer group (p ϭ 0.56) Symptom severity scores were also similar (p ϭ 0.78). At least one rescue bronchodilatator treatment was nec-
essary for 24% of the MDI/spacer group, compared to21% of the Nebulizer group (p ϭ 0.75). The median
We screened 75 patients who presented to our adult ED
length of ED stay was 2 h for both groups, with an IQR
for an asthma exacerbation. Of 75 patients screened, 5
of 1.5–3.0 h for the MDI/spacer group and an IQR of
did not satisfy eligibility criteria and 10 did not giveconsent for participation in the research. The remaining60 patients were randomized into two study groups, 30 in
Table 2. Outcomes by Treatment Group
each group. One patient from each group was not in-cluded in the outcome analysis because one withdrew
consent and the other signed out against medical advice,leaving 29 per group for the study sample. Entry char-
acteristics for the two randomized treatment groups were
similar in terms of race, intubation history, asthma du-
ration Ͼ 10 years, steroid administration, peak flow rate,
and symptom severity score Of the patients
enrolled, 48% were Hispanic and 49% were African-
American. Smoking history was not significantly differ-
ent between the two groups. The MDI/spacer group had
a higher percentage of female patients and was at a
Disposition (discharged home or admitted to hospital)
* Peak flow rate increase, symptom severity decrease, and
was similar between the groups (p ϭ 0.55). One patient
length of stay in ED are presented as median (interquartile range)
in the MDI/spacer group and 2 in the Nebulizer group
and compared with the non-parametric Kolmogorov-Smirnovtest. Disposition and receiving rescue treatments are presented
were admitted to the hospital (3% vs. 7%, respectively),
whereas 28 patients in the MDI/spacer group and 27 in
ARTICLE IN PRESS Table 3. Costs by Treatment Group
* Median (interquartile range). p Values calculated with the non-parametric Kolmogorov-Smirnov test except for delivery system, whichwas constant for both groups, and thus a p value is not applicable.
1–2.5 h for the Nebulizer group (p ϭ 0.78). Adjusting for
MDI/spacer combination compared to those treated us-
age and gender did not meaningfully change the results.
ing a standard nebulizer delivery system. Although the
In post hoc power analysis, with 29 participants per
spacer group tended to be female and older, neither sex
group, there was 95% power to detect if the MDI/spacer
nor age was significantly associated with any of the
was Ͼ 50% less effective than the nebulizer for increas-
outcome measures. Our results are comparable to a num-
ing peak flow rate, and 43% power to detect if the
ber of prior studies that revealed equivalent performance
MDI/spacer was 25% less effective. Similarly, there was
Ͼ 99% and 59% power, respectively, with regard to
In 2005, the American College of Chest Physicians/
decrease in symptom severity scores.
American College of Asthma, Allergy, and Immunology
The cost analysis for the two groups is summarized in
published evidence-based guidelines regarding device
Our cost calculations were based only on treat-
selection and outcomes of aerosol therapy in various
ments with albuterol in each arm and did not include
clinical settings based on a meta-analysis of 59 random-
placebo administration. Payroll costs (including fringe
ized controlled trials (RCT) Of the 19 RCTs that
benefits) for a respiratory therapist in our institutions is
compared aerosol delivery devices in the ED, the nine
on average $40.94 per hour. The RT needed about 10
studies that compared  -agonist delivery by nebulizer to
min to instruct and demonstrate the use of an MDI/spacer
that by an MDI with a spacer/holding chamber in adult
to a patient, just once for the entire ED stay. For the
patients with acute asthma did not report a significant
Nebulizer group, it required an average of approximately12 min per treatment. Thus, the cost for the RT time
difference in pulmonary function response to the two
represents the biggest difference in costs between the
methods of delivery. Only two of the nine studies re-
two groups, with a constant $6.82 per patient in the
ported any significant differences between the two
MDI/spacer group and a median of $16.38 (IQR 8.19 –
groups for time spent in the ED, hospital admission rate,
20.48) for the Nebulizer group (p Ͻ 0.001). There was a
and frequency of ED discharge at 6 h.
one-time cost per patient for the delivery system of $2.95
A Cochrane Database meta-analysis updated in 2006
for the LiteAire Spacer and $1.50 for the nebulizer.
by Cates et al. assessed the effects of spacers compared
Per-treatment costs of the medication were $0.17 and
to nebulizers for the delivery of beta agonists for acute
$0.19 for MDI/spacer and nebulizer, respectively. Total
asthma The updated review now includes data from
costs were significantly lower (p Ͻ .001) for the MDI/
614 adults randomized in 25 trials from the ED and
spacer group, with a median of $10.11 (IQR 10.03–
community settings in addition to the inpatient trials. The
10.28) compared to $18.26 (IQR 9.88 –22.45) for the
outcomes measured in the trials include hospital admis-
sion rates, length of stay in the ED, respiratory and pulserates, blood gases, and lung function. In this meta-analysis,the delivery of beta agonists using a spacer did not seem
DISCUSSION
to affect hospital admission rates for adults when com-pared to beta agonist delivery using a nebulizer, with the
In this study, we demonstrated that beta-agonist delivery
relative risk of admission for spacer vs. nebulizer being
with MDI/spacer and nebulizer have equivalent efficacy
0.97 (95% confidence interval 0.63–1.49). The length of
for adult patients with mild to moderate asthma exacer-
stay in the ED, peak flow rate, and forced expiratory
bation in two inner-city EDs. We found no meaningful
volume were also similar for the two delivery methods.
differences in number of admissions, changes in median
Several methodological limitations, including the lack of
peak flow rate, median symptom score, number of rescue
standardized spacer device, beta-agonist dose, and re-
bronchodilatator treatments, or length of stay in the ED
porting of the data regarding lung function tests in many
between those treated with bronchodilatators using the
studies, may restrict the generalizability of these results
ARTICLE IN PRESS
to patients presenting to the ED with an exacerbation of
No adverse side effects were found in any of the
The cost analysis in our study that took into account
In our literature search, we did not find a validated
equipment, medication, and labor costs revealed that
asthma severity scoring system for adults. This was
there was a significant cost reduction utilizing LiteAire
exemplified by a small pilot study that revealed that the
Spacer vs. a nebulizer. The largest component of the
correlation between wheezing and peak flow was weak
savings was related to the difference in the labor costs
However, in a prior study, when we studied mul-
associated with the two delivery systems. Other studies
tiple subjective symptoms, giving each symptom a se-
have demonstrated similar differences in the labor costs
verity rating, we found a reliable correlation between the
between the two modes of treatment. However, when
cumulative severity symptom score and peak flow
analyzing the labor cost, there is a large variability in the
Hence, we chose to utilize the same symptom scoring
studies with respect to duration of time spent by the RT
system in this study. It is our belief that the scoring system
during nebulizer delivery. The reported time ranges from
utilized in our study can be used when conducting other
4 to 20 min in different studies In our study,
outcome studies, although validation of the scoring system
the median time spent by the RT was 12 min. To see the
in a larger clinical trial would be desirable.
general applicability of this study from a cost perspec-
For patients who have poor coordination between
tive, we looked at the cost of other currently commer-
actuation of MDI and inhalation, spacer use is particu-
cially available spacers. The hospital price range for
larly valuable because it usually requires only a brief
other spacers is between $5.23 and $12.00, a two- to
demonstration of the proper use of a MDI/spacer device
four-fold difference from the spacer device utilized in
to improve user skills In our study, patients
this study. The cost of other commercially available
found it easy to learn to use the spacer device regardless
spacer devices, therefore, would seem to counterbalance
of educational background and socioeconomic status.
the savings derived from the labor economics. Because
The compact spacer we utilized is made of collapsible
the spacer cost in our study is not markedly different
cardboard that can be used for up to 1 week. Drug
from the thrifty nebulizer cost, the difference between
delivery using the LiteAire device has been shown to be
the two groups remains significant. An additional factor
equivalent to other valved holding chambers like the
of economic significance could be the use of CFC albu-
Aerochamber Plus® (Forest Pharmaceuticals Inc., St.
terol MDI in our study as opposed to the hydroflouroal-
kane (HFA) albuterol. Effective December 2008, the USFood and Drug Administration (FDA) has mandated theuse of HFA albuterol only. Of note is that, unlike a
significant difference in the cost of HFA albuterol vs. CFC albuterol in ambulatory and inpatient settings, the
A major limitation to our study was the relatively small
current hospital cost for HFA albuterol MDI for patients
sample size. Although we had adequate statistical power
in the ED is similar to the CFC albuterol. Hence, the new
to be confident that the MDI/spacer was not Ͼ 50% less
FDA mandate to use HFA albuterol has no significant
effective than the nebulizer to increase peak flow rate or
cost implications. Our findings are parallel to other stud-
decrease symptom severity score, the statistical power
ies that have compared MDI/spacers to nebulizer therapy
was not sufficient to have similar confidence with regard
and demonstrated a cost benefit to MDI/spacers
to smaller differences. Nonetheless, the point estimates
of the median values for peak flow rate increase, severity
There is a wide variation in the bronchodilatator dose
of symptoms score, and length of stay in the ED were
(1:1 to 1:12.5) reported in the literature in studies com-
exactly the same for both groups. Furthermore, one pa-
paring the two modes of delivery in the ED setting
tient in the MDI/spacer group needed hospitalization,
Also, potential dose-related adverse effects of beta ago-
compared to 2 patients in the Nebulizer group.
nists have been reported in studies comparing the use of
Another limitation is that the majority of patients had
nebulizers to MDIs in asthma patients. Extra-pulmonary
mild to moderate severity of asthma exacerbation be-
sympathetic effects such as tremor, anxiety, and tachy-
cause the study recruitment was mostly limited to pa-
cardia have been found to be more prevalent in patients
tients managed by a respiratory therapist, whereas those
receiving nebulized medication compared to MDI/spacer-
who were in status asthmaticus were managed by the
delivered medication The choice of the bron-
emergency physicians and excluded from this study. Our
chodilatator dose for our study was based on results of
study could have been more robust had we collected data
previous studies of children and adults demonstrating the
on the baseline use of albuterol or spacers, as well as
comparability of six actuations of albuterol MDI (540
patient returns to the ED after discharge. Because our
g) with spacer to 2.5 mg delivered by nebulizer
trial was limited to only 6 h in the ED, and we did not
ARTICLE IN PRESS
send the patient home with the spacer or conduct a
chamber is equivalent in effectiveness to nebulizer. Chest
follow-up post-disposition, we are unable to comment on
9. Jasper AC, Mohsenifar Z, Kahan S, et al. Cost-benefit comparison
these clinical outcomes. Future studies should include a
of aerosol bronchodilator delivery methods in hospitalized pa-
longer follow-up and collection of the aforementioned
10. Jenkins SC, Heaton RW, Fulton TJ, et al. Comparison of domicil-
iary nebulized salbutamol and salbutamol from a metered-dose
Although larger studies have reported the equivalence
inhaler in stable chronic airflow limitation. Chest 1987;91:804 –7.
of the MDI/spacer combination and nebulizer in adults
11. Manthous CA, Chatila W, Schmidt GA, et al. Treatment of bron-
with acute respiratory disease, our study has the strength
chospasm by metered-dose inhaler albuterol in mechanically ven-tilated patients. Chest 1995;107:210 –3.
of being one of the few conducted in a predominantly
12. Turner JR, Corkery KJ, Eckman D, et al. Equivalence of contin-
minority population in the inner city with a double-
uous flow nebulizer and metered-dose inhaler with reservoir bag
blinded, randomized protocol. Comparing spacer vs.
for treatment of acute airflow obstruction. Chest 1988;93:476 – 81.
nebulizer in the ED for the minority patient population is
13. Tenholder MF, Bryson MJ, Whitlock WL. A model for conversion
from small volume nebulizer to metered dose inhaler aerosol
most relevant because this group utilizes the ED most
frequently Most of the earlier comparison
14. Woodcock A. Use of spacers with metered dose inhalers. Lancet
15. Turner MO, Patel A, Ginsburg S, et al. Bronchodilator delivery in
. We could find only one prior study in an inner-city ED
acute airflow obstruction. A meta-analysis. Arch Intern Med 1997;
where 70% of the patients enrolled were African-American,
but there were few Hispanic patients Our findings
16. Batra V, Sethi GR, Sachdev HP. Comparative efficacy of jet
argue for a larger, multi-center trial to assess equivalence
nebulizer and metered dose inhaler with spacer device in thetreatment of acute asthma. Indian Pediatr 1997;34:497–503.
and cost benefit for an MDI/spacer combination.
17. Schuh S, Johnson DW, Stephens D, et al. Comparison of albuterol
delivered by a metered dose inhaler with spacer versus a nebulizerin children with mild acute asthma. J Pediatr 1999;135:22–7.
18. Williams JR, Bothner JP, Swanton RD. Delivery of albuterol in a
CONCLUSION
pediatric emergency department. Pediatr Emerg Care 1996;12:263–7.
We found no evidence that a conventional nebulizer was
19. Chou KJ, Cunningham SJ, Crain EF. Metered-dose inhalers with
spacers vs nebulizers for pediatric asthma. Arch Pediatr Adolesc
more efficacious than a spacer device for bronchodilata-
tor therapy in adults with acute exacerbation of asthma.
20. Kerem E, Levison H, Schuh S, et al. Efficacy of albuterol admin-
Additionally, using a spacer device may result in a
istered by nebulizer versus spacer device in children with acuteasthma. J Pediatr 1993;123:313–7.
marked reduction in time and effort invested by the
21. Maguire GP, Newman T, DeLorenzo LJ, et al. Comparison of a
respiratory therapist and, consequently, savings in the total
hand-held nebulizer with a metered dose inhaler-spacer combina-
cost for asthma treatment in an inner-city ED setting.
tion in acute obstructive pulmonary disease. Chest 1991;100:1300 –5.
22. O’Reilly JF, Buchanan DR, Sudlow MF. Pressurised aerosol with
conical spacer is an effective alternative to nebuliser in chronic
REFERENCES
stable asthma. Br Med J (Clin Res Ed) 1983;286:1548.
23. Gibson PG, Wlodarczyk JH, Borgas T. Drug delivery in asthma: a
comparison of spacers with a jet nebuliser. Aust N Z J Med
1. U.S. Dept. of Health and Human Services, National Center for
Health Statistics. National Health Interview Survey, 2002 [Com-
24. Prior JG, Nowell RV, Cochrane GM. High-dose inhaled terbutal-
puter file]. ICPSR04176-v2. Hyattsville, MD: U.S. Department of
ine in the management of chronic severe asthma: comparison of
Health and Human Services, National Center for Health Statistics
wet nebulisation and tube-spacer delivery. Thorax 1982;37:300 –3.
[producer]; 2002. Ann Arbor, MI. Inter-university Consortium for
25. Clay MM, Clarke SW. Wastage of drug from nebulisers: a review.
Political and Social Research [distributor]; 2006.
2. Steele LL, Ellemberg CM, Medvesky MG. Asthma among adults
26. Everard ML, Clark AR, Milner AD. Drug delivery from jet nebu-
in New York State 1996 –2002: prevalence and health behavior.
lisers. Arch Dis Child 1992;67:586 –91.
Behavioral Risk Factor Surveillance System 2004;11(1)
3. Alavy B, Chung V, Maggiore D, Shim C, Dhuper S. Emergency
27. Rodrigo C, Rodrigo G. Salbutamol treatment of acute severe
department as the main source of asthma care. J Asthma 2006;43:
asthma in the ED: MDI versus hand-held nebulizer. Am J Emerg
4. Demirkan K, Tolley E, Mastin T, et al. Salmeterol administration
28. Leversha AM, Campanella SG, Aickin RP, et al. Costs and effec-
by metered-dose inhaler alone vs metered-dose inhaler plus valved
tiveness of spacer versus nebulizer in young children with moder-
holding chamber. Chest 2000;117:1314 – 8.
ate and severe acute asthma. J Pediatr 2000;136:497–502.
5. Bowton DL, Goldsmith WM, Haponik EF. Substitution of metered-
29. Barry PW, O’Callaghan C. The effect of delay, multiple actuations
dose inhalers for hand-held nebulizers. Success and cost savings in a
and spacer static charge on the in vitro delivery of budesonide from
large, acute-care hospital. Chest 1992;101:305– 8.
the Nebuhaler. Br J Clin Pharmacol 1995;40:76 – 8.
6. Clausen JL. Self-administration of bronchodilators. Cost effective?
30. National Heart, Lung, and Blood Institute (NHLBI), National
Asthma Education and Prevention Program. Expert Panel Report 2.
7. Garner SS, Wiest DB, Bradley JW, et al. Albuterol delivery by
Guidelines for the diagnosis and management of asthma (NIH
metered-dose inhaler in a mechanically ventilated pediatric lung
publication #97-4051A). Bethesda, MD: NHLBI Health Informa-
model. Crit Care Med 1996;24:870 – 4.
8. Idris AH, McDermott MF, Raucci JC, et al. Emergency department
31. Brenner B, Kohn MS. The acute asthmatic patient in the ED: to
treatment of severe asthma. Metered-dose inhaler plus holding
admit or discharge. Am J Emerg Med 1998;16:69 –75. ARTICLE IN PRESS
32. Dolovich MB, Ahrens RC, Hess DR. Device selection and out-
inhalation technique with metered-dose inhaler plus spacer device.
comes of aerosol therapy: evidenced based guidelines. Chest 2005;
46. Chafin CC, Tolley E, Demirkan K, et al. Effect of a brief educa-
33. Cates CJ, Crilly JA, Rowe BH. Holding chambers (spacers) versus
tional intervention on medical students’ use of asthma devices. J
nebulisers for beta-agonist treatment of acute asthma. Cochrane
47. Okeson C, Loomis K, McGowen P. Metered dose inhaler output
34. Turner MO, Gafni A, Swan D, Fitzgerald JM. A review and
comparison between collapsible paperboard and two rigid plastic
economic evaluation of bronchodilator delivery methods in hospi-
holding chambers. Respir Care J 2006;51:1322.
talized patients. Arch Intern Med 1996;156:2113– 8.
48. Coyle YM, Aragaki CC, Hynan LS, Gruchalla RS, Khan DA.
35. Summer W, Elston R, Tharpe L, et al. Aerosol bronchodilator
Effectiveness of acute asthma care among inner-city adults. Arch
delivery methods. Relative impact on pulmonary function and cost
of respiratory care. Arch Intern Med 1989;149:618 –23.
49. Halm EA, Wisnivesky JP, Leventhal H. Quality and access to care
36. Orens DK, Kester L, Fergus LC, et al. Cost impact of metered dose
among a cohort of inner-city adults with asthma: who gets guide-
inhalers vs small volume nebulizers in hospitalized patients: the
line concordant care? Chest 2005;128:1943–50.
Cleveland Clinic experience. Respir Care 1991;36:1099 –114.
50. Morley TF, Marozsan E, Zappasodi SJ, Gordon R, Griesback R,
37. Camargo CA, Kenney PA. Assessing the costs of aerosol therapy.
Giudice JC. Comparison of beta-adrenergic agents delivered by
nebulizer vs metered dose inhaler with InspirEase in hospitalized
38. Everard ML, Hardy JG, Milner AD. Comparison of nebulised
asthmatic patients. Chest 1988;94:1205–10.
aerosol deposition in the lungs of healthy adults following oral and
51. Raimondi AC, Schottlender J, Lombardi D, Molfino NA. Treat-
nasal inhalation. Thorax 1993;48:1045– 6.
ment of acute severe asthma with inhaled albuterol delivered via jet
39. O’Callaghan C, Clark AR, Milner AD. Why nebulise for more than
five minutes? Arch Dis Child 1989;64:1270 –3.
nebulizer, metered dose inhaler with spacer, or dry powder. Chest
40. O’Callaghan C. How to get drugs into the respiratory tract. Arch
52. Rodriguez IS, Buitrago JR, Garcia RL. Nebulizer versus inhaler
41. Everard ML, Evans M, Milner AD. Is tapping jet nebulisers
plus holding chamber for acute asthma in adults. Data on file 1999
worthwhile? Arch Dis Child 1994;70:538 –9.
(Unpublished data obtained from Cochrane Database 2006; Re-
42. Hung JC, Hambleton G, Super M. Evaluation of two commercial
view of spacers versus nebulisers for beta-agonist treatment of
jet nebulisers and three compressors for the nebulisation of anti-
biotics. Arch Dis Child 1994;71:335– 8.
53. Rodrigo G, Rodrigo C. Comparison of salbutamol delivered by
43. Shim CS, Williams MH Jr. The relationship of wheezing to sever-
nebulizer or metered-dose inhaler with a pear-shaped spacer in
ity of airway obstruction in asthma. Arch Intern Med 1983;
acute asthma. Curr Ther Res Clin Exp 1993;54:797– 808.
54. Newman KB, Milne S, Hamilton C, et al. A comparison of albu-
44. Chandra A, Shim C, Cohen HW, et al. Regular vs ad-lib albuterol
terol administered by metered-dose inhaler and spacer with albu-
for patients hospitalized with acute asthma. Chest 2005;128:1115–20.
terol by nebulizer in adults presenting to an urban emergency
45. Self TH, Kelso TM, Arheart KL, et al. Nurses’ performance of
department with acute asthma. Chest 2002;121:1036 – 41. ARTICLE IN PRESS ARTICLE SUMMARY 1. Why is this topic important?
Asthma exacerbations are costly to manage. In addi-
tion to therapies that increase asthma control and reduce the frequency or severity of exacerbations, other efforts to decrease cost may bring economic benefits. Inner-city patients frequently use the emergency department (ED) for asthma exacerbations. This study presents data on the use of a metered dose inhaler with spacer as a cost- effective alternative to nebulizer therapy for use in acute exacerbation of asthma in an inner-city ED. Hence, an alternate mode of B- agonist delivery may reduce the number of ED visits. Although nebulizer use for bron- chodilatator delivery in asthma exacerbation requires longer delivery times and greater resource utilization, their use is the standard of care due to the expense of commercially available spacer devices, which would oth- erwise be a viable alternative. This study presents data on the use of MDI with spacer as an efficient, cost-effective alternative to nebulizer for use in acute exacerbation of asthma in the inner-city population. 2. What does this study attempt to show?
This study attempts to demonstrate that albuterol de-
livered with spacer is an efficient, cost-effective alterna- tive to nebulized albuterol treatment for asthma patients in the ED in an inner-city hospital. 3. What are the key findings?
Albuterol delivery using the nebulizer or spacer in
patients with acute asthma exacerbation resulted in equivalent improvements in peak expiratory flows and asthma symptoms in patients, in this randomized, double- blinded, placebo-controlled trial. The number of rescue treatments required in the two groups and the length of ED stay were also equivalent .The cost was significantly less for the spacer device. Most of the cost benefit was derived by the amount of time the respiratory therapist spent with the patient. 4. How is patient care impacted?
This study demonstrates that use of spacer devices may
decrease the economic burden of asthma managementwithout compromising the quality of care delivered in aninner-city patient population who frequently use the EDfor managing their asthma.
Determination of Steroids in A solution to these problems is to use an SFE instrument and method that simplifies the Animal Tissues by separation and recovery of trace level drug residues from an analyte/fat matrix. This Supercritical Fluid application describes a procedure for coupling SFE Extraction and Inline technology with an inline trapping technique to quickly and easily
William Vlach Assistant Lab/PSD Manager ADM Cocoa 12500 W. Carmen Ave. Milwaukee, WI 53225-6199 PH: 414-358-5886 William_vlach@admworld.com Bill graduated from Concordia University with a B.A. in Science. He has been a presenter for ten years at in-house seminars held by ADM Cocoa and has attended workshops and seminars including Penn State Chocolate Manufacturer

 ARTICLE IN PRESS
ARTICLE IN PRESS ARTICLE IN PRESS
ARTICLE IN PRESS
 ARTICLE IN PRESS
ARTICLE IN PRESS ARTICLE IN PRESS
ARTICLE IN PRESS ARTICLE IN PRESS
ARTICLE IN PRESS ARTICLE IN PRESS
ARTICLE IN PRESS ARTICLE IN PRESS
ARTICLE IN PRESS ARTICLE IN PRESS
ARTICLE IN PRESS ARTICLE IN PRESS
ARTICLE IN PRESS