Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Slep.com.br
The Journal of Clinical Endocrinology & Metabolism 90(12):6553– 6555
Copyright 2005 by The Endocrine Society
BRIEF REPORT Serum Thyrotropin (TSH) Levels after Recombinant Human TSH Injections in Children and Teenagers with Papillary Thyroid Cancer
S. Iorcansky, V. Herzovich, R. R. Qualey, and R. M. Tuttle
Endocrinologia, Hospital de Pediatria (S.I., V.H.), 1245 Buenos Aires, Argentina; and Department of Endocrinology,Memorial Sloan Kettering Cancer Center (R.R.Q., R.M.T.), New York, New York 10021Context: In preparation for whole body radioactive iodine scanning, Results: The mean serum TSH at the time of RAI administration was
recombinant human TSH (rhTSH) is usually administered as 0.9-mg
similar in patients undergoing hypothyroid preparation (188 Ϯ 118
im injections on 2 consecutive days without regard to age, body size,
mIU/liter; range, 110 – 452 mIU/liter) and those treated with rhTSH
(134 Ϯ 75 mIU/liter; range, 32–290 mIU/liter; P ϭ 0.07). Serial de-terminations after rhTSH injections revealed a mean serum TSH of
Objective: Our objective was to determine whether the usual adult
268 Ϯ 76 mU/liter (range, 87– 628) at 6 h and 130 Ϯ 58 mU/liter
rhTSH dosing regimen would result in excessive elevations of serum
(range, 67–250) at 24 h after the initial injection, and 361 Ϯ 78
TSH in children and teenagers with thyroid cancer.
mU/liter (range 161–524) at 6 h and 134 Ϯ 44 mU/liter (range, 32–290)at 24 h after the second injection. Design/Setting/Patients/Interventions: A retrospective review identified 53 children and teenagers with thyroid cancer who under- Conclusions: The mean TSH levels achieved in children after rhTSH
went whole body radioactive iodine (RAI) scanning over a 12-yr period
injections are remarkably similar to values previously reported in
at two major medical centers (34 after thyroid hormone withdrawal
adults despite marked differences in clinical characteristics between
children and adults. These data suggest that dose adjustments are notgenerally required in children and teenagers undergoing rhTSH stim-
Main Outcome Measures: The dynamic time course of changes in
ulation for RAI scanning or serum-stimulated thyroglobulin
serum TSH after rhTSH administration and/or hypothyroid with-
determinations. (J Clin Endocrinol Metab 90: 6553– 6555, 2005)
drawal was examined. Peak TSH levels were correlated with age,weight, and body surface area.
IN NOVEMBER 1998, the U.S. Food and Drug Adminis- regardlessofage,gender,sizeofthepatient,orothercomorbid
tration issued approval for the use of recombinant hu-
conditions. A recent study by Vitale et al. (4) demonstrated a
man TSH (rhTSH; Thyrogen, Genzyme Corp., Cambridge,
significant influence of body surface area on peak serum TSH
MA) as an adjunctive diagnostic tool for serum thyroglobulin
levels after two consecutive daily injections of 0.9 mg rhTSH. In
testing with or without radioiodine imaging in the follow-up
multivariate analysis, body surface area (BSA) was negatively
of well-differentiated thyroid cancer.
correlated with peak TSH levels. The lowest peak TSH of 22
The standard dose of rhTSH can be administered either as
mIU/liter was documented in the patient with the highest BSA
two 0.9-mg injections 24 h apart or three 0.9-mg injections at
[120 kg, female, with a body mass index (BMI), 41.5 kg/m2;
72-h intervals (1). In healthy volunteers, pharmacokinetic
BSA, 2.44 m2], whereas the two highest peak TSH values (ϳ260
studies after a single im 0.9-mg injection of rhTSH demon-
and ϳ280 mIU/liter) were seen in two of the three children
strate a peak serum TSH of approximately 280 mIU/liter
included in this study (age, 10 and 11 yr; BMI, 22.3 and 22.5
within 6 – 8 h of injection, which then falls to approximately
kg/m2, respectively; BSA, 1.23 and 1.32 m2, respectively). These
140 mIU/liter at 24 h and 25 mIU/liter at 48 h after rhTSH
observations suggest that alterations in dosing may be neces-
administration (2). Serious adverse effects after rhTSH wereuncommon, but nausea and headache were seen more fre-
sary in patients with either a very low or a very high BSA.
quently with the highest rhTSH doses tested in the initial
Over the last several years, an extensive body of literature
phase I/II trial of healthy adult volunteers (3).
has documented the safety and clinical efficacy of rhTSH in
In general, this standard dosing regimen is routinely used
the follow-up of adults with thyroid cancer (5, 6). Because ofthis track record of safety in adults, we began to offer rhTSHpreparations for radioactive iodine (RAI) scanning and thy-
First Published Online September 20, 2005 Abbreviations: BMI, Body mass index; BSA, body surface area; RAI,
roglobulin stimulation initially to teenagers, and then to
radioactive iodine; rhTSH, recombinant human TSH.
younger children with thyroid cancer. As with our previous
JCEM is published monthly by The Endocrine Society (http://www.
studies (7, 8), rhTSH was used with the full consent of the
endo-society.org), the foremost professional society serving the en-
patients and their parents in a clinical setting, with the ex-
docrine community.
J Clin Endocrinol Metab, December 2005, 90(12):6553– 6555
Iorcansky et al. • rhTSH in Children
pectation of clinical benefit and to avoid the clinical symp-
TABLE 1. Clinical characteristics of patients
In this manuscript we retrospectively review our clinical
experience in children and teenagers undergoing diagnostic
RAI whole body scanning over the last several years, with
particular emphasis on serum TSH levels at the time of testing
after either hypothyroid withdrawal or rhTSH stimulation. Subjects and Methods
Clinical records were retrospectively reviewed to identify children
and teenagers less than or equal to 18 yr of age undergoing routine
diagnostic whole body RAI scanning at two medical centers between
BSA (square meters) was calculated using the following formula:
BSA ϭ 0.20247 ϫ height (m)0.725 ϫ weight (kg)0.425. BMI was calculated
mU/liter (range, 67–250) 24 h after the initial injection and 361 Ϯ
using the following formula: BMI ϭ weight (kg)/height (m)2.
78 mU/liter (range, 161–524) at 6 h, and 134 Ϯ 44 mU/liter
Patients pretreated with rhTSH (Thyrogen, Genzyme Corp.) received
(range, 32–290) 24 h after the second injection (see Fig. 1, left
0.9 mg, im, into the gluteus maximus on 2 consecutive days accordingto the standard adult regimen. panel). As shown in Fig. 1, the initial 24-h serum TSH values
In each patient prepared with traditional hypothyroid withdrawal
were very similar to values previously reported by Torres et al.
(discontinuation of levothyroxine for 3– 6 wk before diagnostic scan-
in a cohort of six normal adults (2).
ning), serum TSH was available at the time of administration of the
The mean serum TSH level at the time of RAI adminis-
diagnostic dose of RAI. Because most patients undergoing rhTSH sim-ulation were having full dosimetry studies, blood samples were avail-
tration appeared to be slightly higher in patients undergoing
able just before the initial 0.9-mg rhTSH injection and 6, 10, 24, 30, and
hypothyroid preparation (188 Ϯ 118 mIU/liter; range, 110 –
48 h after the initial rhTSH injection. Because this was a retrospective
452 mIU/liter) than in those prepared with rhTSH (134 Ϯ 75
study, not all patients had sampling performed at all time points.
mIU/liter; range, 32–290 mIU/liter), although this difference
The serum TSH levels were measured using a variety of assays over
did not reach statistical significance (P ϭ 0.07).
the last 10 yr, with normal reference ranges that have generally rangedfrom 0.5–5 mIU/liter. No attempt was made to correct for minor dif-
Because our cohort included a wide range of ages, rhTSH-
ferences in TSH assays either within institution or between institutions.
stimulated patients were divided into three groups, based on
The data are presented as the TSH value clinically reported in the
age at the time of diagnostic scanning, to compare children
less than 13 yr of age with young teenagers (13–15 yr old,
Data are analyzed based on the TSH level at the time of RAI admin-
istration and on the peak TSH level achieved before RAI administration.
inclusive) and older teenagers (Ͼ15–18 yr old, inclusive). No
In the hypothyroid withdrawal group, the peak TSH was the TSH level
significant differences were seen in the mean serum TSH
at the time of RAI administration. All data are presented as the mean Ϯ
levels at the time of RAI administration after two consecutive
se, with medians and ranges given as appropriate. ANOVA was used
rhTSH injections in children (187 Ϯ 107 mIU/liter), young
to analyze mean values between multiple groups. P Ͻ 0.05 was con-sidered significant. Associations between individual BSA and peak TSH
teenagers (88 Ϯ 71 mIU/liter), and older teenagers (130 Ϯ 76
and TSH levels at the time of RAI administration were analyzed by
mIU/liter). Likewise the serum TSH values over time after
rhTSH injections were quite similar among the three groups,although the younger children tended to have higher peak
TSH values after each injection than the older teens, and this
A total of 53 children and teenagers underwent routine
difference did not reach statistical significance (see Fig. 1,
RAI diagnostic scanning as part of their follow-up for thyroid
cancer at our institutions over a 12-yr period (1990 –2002). All
A comparison of either peak serum TSH or TSH at the time
patients included in this analysis had previously undergone
of RAI administration with BSA, weight, or age failed to
total thyroidectomy and radioactive iodine remnant ablation
demonstrate any significant correlation in patients stimu-
The majority of the patients (n ϭ 34) underwent traditional
No significant adverse side effects were reported in the
thyroid hormone withdrawal; 19 patients received rhTSH
patients undergoing rhTSH stimulation. As would be ex-
injections in preparation for RAI scanning. With regard to the
pected, chart review did reveal mild nausea and headaches
patients seen at each institution, 23 of the patients were seen
in a few of the patients. In no case did the nausea or headache
at the Hospital de Pediatria, Buenos Aires (including 12
require treatment or admission to the hospital. Although
patients prepared with rhTSH with an age range of 9 –18 yr,
RAI-avid pulmonary metastasis were present in 25% of the
and 11 patients prepared with thyroid hormone withdrawal
patients, and one patient had an RAI-avid skull metastasis,
with an age range of 4.6 –15 yr). Thirty of the patients were
none experienced pain or swelling sufficient to result in
evaluated at Memorial Hospital, New York (including seven
pulmonary compromise or neurovascular compromise.
patients prepared with rhTSH with a mean age of 15–18 yr,and 23 patients prepared with thyroid hormone withdrawal
Discussion
with a mean age of 6 –18 yr). A summary of the clinical
Contrary to what we expected, the serum TSH profile after
characteristics of these patients is given in Table 1.
two consecutive daily doses of 0.9 mg in children and teen-
The mean serum TSH levels after two 0.9-mg rhTSH injec-
agers was very similar to that previously reported in studies
tions were 268 Ϯ 76 mU/liter (range, 87–628) 6 h and 130 Ϯ 58
of normal adults, as shown in Fig. 1 (2, 3). Furthermore, the
Iorcansky et al. • rhTSH in Children
J Clin Endocrinol Metab, December 2005, 90(12):6553– 6555
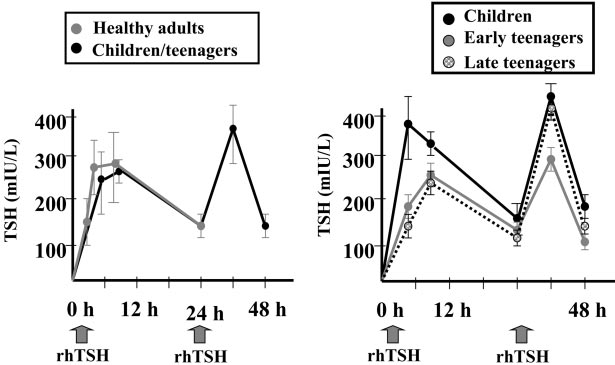
FIG. 1. In the left panel, serum TSH levels after 0.9-mgrhTSH im injections on 2 consecutive days in children andteenagers with thyroid cancer compared with serum TSHvalues measured after a single 0.9-mg im injection of rhTSHin six healthy adult volunteers in the study by Torres et al. (2). Despite significant differences in age and body sizebetween children and adults, the serum TSH curves showremarkable overlap in the first 24 h after rhTSH adminis-tration. In the right panel, serum TSH levels after rhTSHadministration (0.9 mg, im, on 2 consecutive days) analyzedby age of the patient at the time of injection. Children refersto patients less than 13 yr of age, early teenagers were13–15 yr old (inclusive), and late teenagers were more than15–18 yr old (inclusive). Although there is a trend towardhigher peak serum TSH levels in the youngest children,these differences did not reach statistical significance (byANOVA).
TSH level at the time of RAI administration in this cohort of
Received July 13, 2005. Accepted September 12, 2005.
children and teenagers (mean TSH, 134 Ϯ 75 mIU/liter) was
Address all correspondence and requests for reprints to: Dr. R. Mi-
very similar to that previously reported by Robbins et al. (9)
chael Tuttle, Department of Endocrinology, Schwartz Building, Room
in 45 adults with thyroid cancer (mean TSH, 105 Ϯ 43 mIU/
713 (Box 419), Memorial Sloan Kettering Cancer Center, 1275 YorkAvenue, New York, New York 10021. E-mail: tuttlem@mskcc.org.
liter), and by Haugen et al. (1) in 117 adults with thyroidcancer (mean TSH, 124 Ϯ 59 mIU/liter). These data wouldsuggest that dose alterations may not be necessary when
References
rhTSH is used in children and teenagers with thyroid cancer.
In our cohort of children and teenagers, no correlation was
1. Haugen BR, Pacini F, Reiners C, Schlumberger M, Ladenson PW, Sherman
detected among BSA, the age of the patient, and either the peak
SI, Cooper DS, Graham KE, Braverman LE, Skarulis MC, Davis TF, DeGroot
TSH or the TSH level at the time of RAI administration. As in
LJ, Mazzeferri EL, Daniels GH, Ross DS, Luster M, Samuels MH, Becker DV, Maxon III HR, Cavalieri RR, Spencer CA, McEllin K, Weintraub BD, Ridg-
the study of Vitale et al. (4), the peak TSH levels in children in
way EC 1999, A comparison of recombinant human thyrotropin and thyroid
our cohort also was in the 250–260 mIU/liter range. The BSA
hormone withdrawal for the detection of thyroid remnant or cancer. J Clin
values for most patients in our cohort were normal to low,
2. Torres MS, Ramirez L, Simkin PH, Braverman LE, Emerson CH 2001, Effect
making it impossible to directly compare peak TSH values with
of various doses of recombinant human thyrotropin on the thyroid radioactive
those seen in the largest patients in the Vitale study (4).
iodine uptake and serum levels of thyroid hormones and thyroglobulin in
Fortunately, rhTSH was very well tolerated by all of the
normal subjects. J Clin Endocrinol Metab 86:1660 –1664
patients, with only minimal nausea and occasional head-
3. Meier CA, Braverman LE, Ebner SA, Veronikis I, Daniels GH, Ross DS, Deraska DJ, Davies TF, Valentine M, DeGroot LJ 1994 Diagnostic use of
aches as would be expected in a typical adult thyroid cancer
recombinant human thyrotropin in patients with thyroid carcinoma (phase I/II
cohort. There were no serious or unexpected side effects.
study). J Clin Endocrinol Metab 78:188 –196
It should be noted that this manuscript does not address
4. Vitale G, Lupoli GA, Ciccarelli A, Lucariello A, Fittpaldi MR, Fonderico F, Panico A, Lupoli G 2003 Influence of body surface area on serum peak
the sensitivity or specificity for disease detection in these
thyrotropin (TSH) levels after recombinant human TSH administration. J Clin
children. Although there is no reason to suspect that rhTSH
would not be a useful adjunct to disease detection in children
5. Robbins RJ, Robbins AK 2003 Clinical review 156: recombinant human thy-
rotropin and thyroid cancer management. J Clin Endocrinol Metab 88:1933–
with thyroid cancer, additional studies are needed to verify
the clinical utility of rhTSH for the detection of recurrent
6. Mazzaferri EL, Massoll N 2002 Management of papillary and follicular (dif-
disease in children with thyroid cancer.
ferentiated) thyroid cancer: new paradigms using recombinant human thy-
In summary, our data demonstrate that rhTSH can be safely
rotropin. Endocr Relat Cancer 9:227–247
7. Robbins RJ, Tuttle RM, Sharaf RN, Larson SM, Robbins HK, Ghossein RA,
administered to children and teenagers without significant un-
Smith A, Drucker WD 2001, Preparation by recombinant human thyrotropin
expected side effects. Furthermore, the serum TSH pharmaco-
or thyroid hormone withdrawal are comparable for the detection of residual
kinetic profiles after two consecutive daily doses of 0.9 mg
differentiated thyroid carcinoma. J Clin Endocrinol Metab 86:619 – 625
8. Robbins RJ, Chon JT, Fleisher M, Larson SM, Tuttle RM 2002 Is the serum
rhTSH are very similar in adults and children, making dose
thyroglobulin response to recombinant human thyrotropin sufficient, by itself,
adjustments unnecessary in all but the very youngest children.
to monitor for residual thyroid carcinoma? J Clin Endocrinol Metab 87:3242–3247
Acknowledgments
9. Robbins RJ, Larson SM, Sinha N, Shaha A, Divgi C, Pentlow KS, Ghossein R, Tuttle RM 2002 A retrospective review of the effectiveness of recombinant
The authors thank Lucı´a Santiago for her help with the manuscript
human TSH as a preparation for radioiodine thyroid remnant ablation. J Nucl
and graphics and Dr. Lucrecia Miravalle for her clinical assistance. JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.
Long-Term Treatment of Transsexuals with Cross-Sex Hormones: Extensive Personal Experience Louis J. Gooren, Erik J. Giltay, and Mathijs C. BunckDepartment of Endocrinology (L.J.G., M.C.B.), Vrije Universiteit University Medical Center, 1081 HV Amsterdam, The Netherlands; andLeiden University Medical Center (E.J.G.), Department of Psychiatry, 2333 ZA Leiden, The Netherlands Context: Transsexu
Faculté des sciences de l’administrationQuébec (Québec) Canada G1K 7P4Tél. Ph. Tel. :Vice-décanat à la recherche et au développementFaculté des sciences de l’administration DOCUMENT DE TRAVAIL 2000-019 Chantal Gravel Martine Lécuyer Lise Lamothe One-line publication updated :Seria electrónica, puesta al dia Le marché canadien du médicament Document préparé par :
 Iorcansky et al. • rhTSH in Children
J Clin Endocrinol Metab, December 2005, 90(12):6553– 6555
FIG. 1. In the left panel, serum TSH levels after 0.9-mgrhTSH im injections on 2 consecutive days in children andteenagers with thyroid cancer compared with serum TSHvalues measured after a single 0.9-mg im injection of rhTSHin six healthy adult volunteers in the study by Torres et al.
Iorcansky et al. • rhTSH in Children
J Clin Endocrinol Metab, December 2005, 90(12):6553– 6555
FIG. 1. In the left panel, serum TSH levels after 0.9-mgrhTSH im injections on 2 consecutive days in children andteenagers with thyroid cancer compared with serum TSHvalues measured after a single 0.9-mg im injection of rhTSHin six healthy adult volunteers in the study by Torres et al.