Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
1189
INT J TUBERC LUNG DIS 5(3):272–277 2001 IUATLD Pulmonary resection in the treatment of patients with pulmonary multidrug-resistant tuberculosis in Taiwan C-Y. Chiang,* M-C. Yu,* K-J. Bai,* J. Suo,* T-P. Lin,* Y-C. Lee† * Chronic Disease Control Bureau, Department of Health, Shen-Keng Shiang, Taipei County, † Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan, Republic of China S E T T I N G : Chronic Disease Control Bureau, Depart- reserve, and 4) whose treatment regimen had been com- ment of Health, Taiwan. posed of at least two effective drugs to diminish the O B J E C T I V E : To evaluate the role of pulmonary resec- mycobacterial burden. tion in the treatment of pulmonary tuberculosis resistant R E S U L T S : There was no surgical mortality apart from to isoniazid and rifampin (MDR-TB). one peri-operative death (4%). Three patients (11%) D E S I G N : In a retrospective cohort study, 27 MDR-TB developed complications, and 24 (92%) patients dem- patients who underwent pulmonary resection between onstrated sputum conversion and/or remained negative December 1990 and March 1999 were reviewed. after surgery. Twenty-three patients have already com- Individually-tailored treatment regimens were selected pleted treatment, and during a mean of 42 Ϯ 18 follow- at a once-weekly staff conference following review of the up months (range 15–80 months), one patient relapsed. patient’s case history and drug susceptibility results. Sur- This patient was disease-free after another course of gery was performed for selected patients, essentially treatment. those: 1) whose medical treatment had failed, or for whom C O N C L U S I O N : For selected patients, pulmonary resec- treatment failure seemed highly likely, or for whom post- tion may improve the outcome of pulmonary MDR-TB. treatment relapse seemed likely, 2) with predominantly K E Y W O R D S : surgery; pulmonary resection; multidrug- localised disease, 3) with adequate cardiopulmonary
FOR PULMONARY tuberculosis (TB) patients with
vention for the treatment of pulmonary TB, having
drug-susceptible organisms, a 6-month regimen con-
been relegated to the distant background for decades,
sisting of isoniazid (INH), rifampin (RMP), and pyr-
may now play a role once again. For selected pulmo-
azinamide (PZA) given for the first 2 months fol-
nary MDR-TB patients with localised disease, the
lowed by INH and RMP for the remaining 4 months
combination of pulmonary resection and second-line
achieves a cure rate of more than 95%.1 When the
anti-tuberculosis agents has been previously reported
organism is resistant to INH and RMP (multidrug-
resistant tuberculosis: MDR-TB), however, even the
Tuberculosis remains a major public health prob-
best available treatment is often unsuccessful.2,3 To
lem in Taiwan. In 1997, 15 386 newly-diagnosed TB
evaluate the magnitude of the problem of resistance to
cases were reported, with an incidence rate of 71.1
anti-tuberculosis drugs worldwide, in 1994 the Global
per 100 000 population,6 and a tuberculosis mortality
Tuberculosis Programme of the World Health Organi-
of 7.48/100 000.7 According to a report from the
zation (WHO) and the International Union Against
Chronic Disease Control Bureau, Department of
Tuberculosis and Lung Disease (IUATLD) initiated
Health, in 1996, the incidence of primary MDR-TB
the Global Project on Anti-Tuberculosis Drug Resis-
was 1.6%, and the rate of acquired MDR-TB was as
tance Surveillance.4 MDR-TB was classified as pri-
high as 46%.8 The problem of drug resistance is
mary and acquired: primary MDR-TB was defined as
clearly challenging the Bureau’s TB programme.
a case without prior history of treatment for tubercu-
The prognosis for pulmonary MDR-TB patients
losis, while acquired MDR-TB was defined as a case
treated in Taiwan has been reviewed previously.
whose problem of resistance results from inadequate
Between January 1988 and December 1990, 87 pul-
treatment. The surveillance revealed that in certain
monary MDR-TB patients were treated by the
areas, the rate of MDR-TB was alarming.
Bureau. Of 78 patients with sufficient follow-up data,
Facing the challenge of MDR-TB, surgical inter-
41 (53%) responded to chemotherapy, becoming spu-
Correspondence to: Dr Yung-Chie Lee, Department of Surgery, National Taiwan University Hospital, 7 Chung San SouthRoad, Taipei, Taiwan, Republic of China. Tel: (ϩ886) 2-2664 5392. Fax: (ϩ886) 2-3393 3989. e-mail: jones1@ms7.hinet.netArticle submitted 6 June 2000. Final version accepted 9 November 2000.Pulmonary resection in the treatment of MDR-TB
tum culture negative, five of whom subsequently
wan,10 it was felt that the possibility of HIV infection
experienced a relapse. The overall favourable response
amongst these MDR-TB patients was very low.
rate was thus 46% over a mean period of 23 months.3
The clinical characteristics of these patients are
In that study, six (86%) of seven patients who under-
shown in Table 1. There were 15 men (54%), with a
went surgical intervention had a favourable response.
mean age of 44.3 Ϯ 11.6 years (range 24–67). All iso-
On the basis of these encouraging results, patients eli-
lates were resistant to a high concentration of RMP
gible for surgery were organised to undergo pulmo-
(5.0 ug/ml), and all except one were resistant to a high
nary resection as an adjunct in the treatment of pul-
concentration of INH (1.0 ug/ml). All of these
monary MDR-TB. We here report our experience
patients were classified as acquired MDR-TB. Before
surgery, the patients had had active TB for a meanperiod of 8 years (range 1–24), and had previouslyreceived a mean of six drugs (range 3–9). Seventeen
MATERIALS AND METHODS
patients (63%) had previously received second-line
We defined MDR-TB as pulmonary disease occurring
anti-tuberculosis agents as a retreatment regimen.
in patients with strains of Mycobacterium tuberculo-
Predisposing illness included diabetes mellitus in two
sis resistant in vitro to at least INH and RMP. Twenty-
and pneumoconiosis in one patient. All of the 27
seven patients who underwent pulmonary resection
patients were shedding organisms resistant to at least
in the treatment of pulmonary MDR-TB between
three drugs. As seen in Table 1, 11 strains demon-
December 1990 and March 1999 were included in this
strated resistance to one drug in addition to INH and
retrospective cohort study. These patients were treated
RMP (one to SM and 10 to EMB); nine strains were
by the Bureau, a centre responsible for the National
resistant to two additional drugs (three to SM and
TB Programme and a referral hospital with 100 beds
EMB, two to EMB and PAS, one to EMB and ETH,
available for treating TB patients. An average of 1300
one to PAS and KM, one to EMB and KM and one to
TB cases were treated by the Bureau each year, of
EMB and OFL); six were resistant to three additional
whom 6% were pulmonary MDR-TB patients. Some
drugs (three to SM/EMB/ETH, two to SM/EMB/PAS
of these patients had previously been treated at other
and one to SM/EMB/OFL); and one strain was resis-
hospitals and were subsequently referred to the
tant to four additional agents (EMB, KM, SM and
Bureau for further management. All drug susceptibil-
ity tests were performed in the Bureau’s mycobacteri-ology laboratory.
The absolute concentration method was used for
Characteristics of patients with multidrug-resistant
susceptibility testing on Middlebrook 7H10 agar
(1990–1993) or Middlebrook 7H11 agar (1994–
1999).9 The low and high drug concentrations in themedium were INH 0.2 g/ml, 1.0 g/ml; RMP 2.5
g/ml, 5.0 g/ml; streptomycin (SM) 5.0 g/ml, 1.0
g/ml; ethambutol (EMB) 7.5 g/ml, 15.0 g/ml;
kanamycin (KM) 6.0 g/ml, 12.0 g/ml, prothiona-
mide (ETH) 10.0 g/ml, 15.0 g/ml; para-aminosali-
cylic acid (PAS) 4.0 g/ml, 8.0 g/ml; enviomycin
(ENV) 2.5 g/ml, 5.0 g/ml; and ofloxacin (OFL) 1.0
g/ml, 2.0 g/ml. Surgery was performed at the
National Taiwan University Hospital, a medical cen-
tre in close liaison with the Bureau.
Patient records were reviewed for the following
information: age, sex, concomitant disease(s), prior
treatment history and medication received, date effec-
tive second-line anti-tuberculosis drugs started, dura-
tion of pre- and post-operative medication regimen,
results of acid-fast smear and culture of sputum, drug
susceptibility result, operation procedure and compli-
cations, and final outcome. Chest radiographies were
Number of anti-TB drugs previously not used
read by two of our group, and were reviewed by a
third member of the group when opinions differed.
Human immunodeficiency virus (HIV) infection was
not routinely tested for amongst these patients. Based
* Drug list: isoniazid, ethambutol, rifampin, pyrazinamide, streptomycin, kan-
on the follow-up history, and given the low preva-
amycin, prothionamide, para-aminosalicylic acid, enviomycin, cycloserine andofloxacin.
lence of HIV infection amongst TB patients in Tai-
The International Journal of Tuberculosis and Lung Disease
Persistent sputum culture-positive for M. tuberculosis
despite treatment with adequate second-lineanti-TB drugs for at least 12 months.
Surgery in the early stages of treatment for patients
whose resistance pattern and extent of lungdestruction, based on our previous experience,predicted a high probability of treatment failure.
Surgery in the late stages of treatment for patients
with sputum conversion, yet still demonstrating apossibility of relapse that was of concern to us.
* Converted to and remained negative. † Excludes 1 peri-operative death.
Individually-tailored treatment regimens for the
patients were decided upon at a once-weekly staff
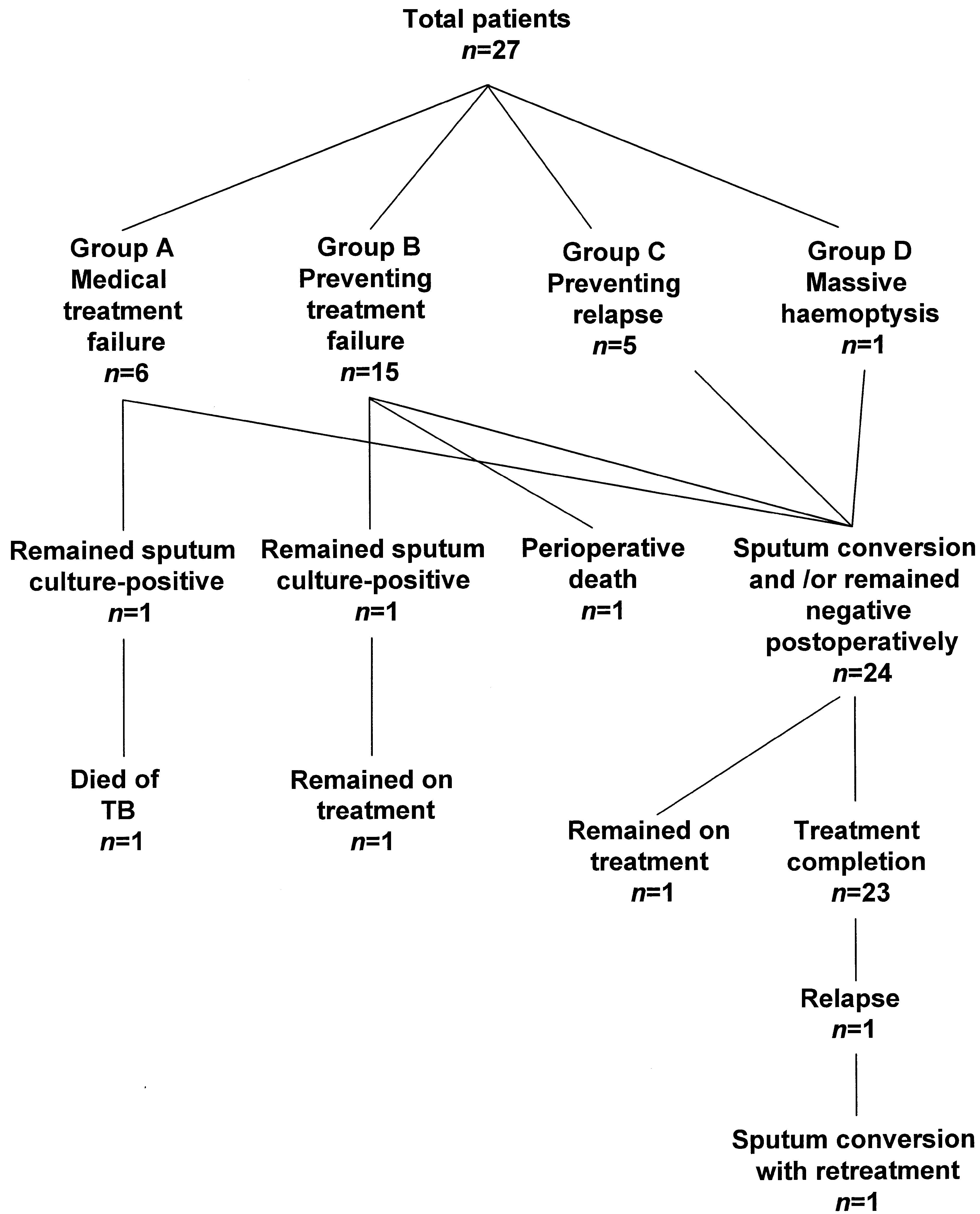
A flow-chart of the overall results of operation is
conference after review of the case history and drug
shown in the Figure, and the surgical procedures per-
susceptibility results. The drugs used and the dosages
formed and post-surgery outcomes are shown in
at which they were prescribed are as followed: EMB
Table 3. Whilst there was no direct surgical mortality,
800–1200 mg daily; PZA 1000–1500 mg daily; ETH
one patient (4%) died suddenly and unexpectedly
250 mg 2–3 times daily; PAS 150–200 mg/kg/day
after taking a hypnotic on the seventh post-operative
divided into 3–4 doses; cycloserine 250 mg 2–3 times
day. Three patients (11%) developed complications
daily; OFL 300–400 mg twice daily; SM/KM/ENV
post-operatively: one exhibited persistent wound
10–15 mg/kg/day daily for 2–3 months, then 3 times
infection with bronchopulmonary-pleural fistula for-
weekly for 2–3 months. An average of 3.8 chemother-
mation, one experienced bleeding into the pleural
apeutic agents to which the organism was fully orpartially susceptible were employed in the treatmentof these patients. The duration range of pre-operativetreatment extended from 2 to 33 months, with a meanof 10 months.
Indications for surgery are shown in Table 2. The
criteria for surgery are as follows: 1) patients with pre-dominantly localised disease, 2) patients with adequatecardiopulmonary reserve, and 3) patients whose treat-ment regimen had been composed of at least two effec-tive drugs to diminish the mycobacterial burden.
Group A patients (n ϭ 6) were operated upon due
to medical treatment failure; surgery was regarded as alast resort to treat their disease. Group B patients (n ϭ15) were prepared for surgical intervention in the earlystages of second-line anti-tuberculosis chemotherapy;eight patients in this group (53.3%) failed to dem-onstrate sputum conversion prior to surgery. Group Cpatients (n ϭ 5) were operated upon in the late stagesof their treatment; they exhibited sputum conversionprior to surgery, and were operated upon particularlyto remove lung cavities in order to prevent futurerelapse. The single patient in Group D was operatedupon due to life-threatening massive haemoptysis.
The extent of lung resection was determined by con-
ventional chest radiography and computed tomogra-phy. A pulmonary function test was performed if post-
Results of 27 patients undergoing pulmonary resec-
operative pulmonary reserve was of concern.
tion for pulmonary multidrug-resistant tuberculosis. Pulmonary resection in the treatment of MDR-TB
another course of anti-TB treatment subsequent to
relapse, and again completed treatment. The group Dpatient operated on for haemoptysis has subsequently
In summary, 24 of 26 patients (92%) (excluding
one peri-operative death) underwent sputum conver-
sion after surgery. One patient died of TB, two were
still on treatment (one had sputum conversion, one
remained sputum-positive), and 23 completed treat-
ment with a mean post-operative treatment duration
of 15 months (range 8–24). Amongst the 23 patients
who completed treatment, with a mean of 42 months
of follow-up (range 15–80), one patient relapsed. DISCUSSION
Using a combination of pulmonary resection and
appropriate medical treatment, we have achieved a
92% response rate among patients with chronic
MDR-TB, with strains resistant to a mean of 3.9
drugs (range 3–6). The contribution of surgery in the
Bacteriological response (n ϭ 26)*
treatment of MDR-TB is most impressive amongst
patients in group A, who had received extendedcourses of second-line anti-TB treatment but failed to
* Excludes 1 peri-operative death. RUL ϭ right upper lobe; RUL plus ϭ RUL lobectomy plus segmentectomy
demonstrate sputum conversion. Surgery was thus per-
and/or wedge resection; LUL ϭ left upper lobe; LLL ϭ left lower lobe.
formed somewhat as a last resort, as for these patientsthe possibility of overall disease control seemed verylow if surgical intervention had not taken place. Most
cavity, requiring re-exploration to stop the bleeding,
of these patients initially refused surgery or were hes-
and one demonstrated a prolonged pulmonary air-
itant to undergo the operation. Attainment of an
leak with associated hydropneumothorax and fever
83.3% sputum conversion rate among this group is
appearing 20 days after surgery, which subsided after
encouraging, and supports the use of surgery by prac-
the administration of further antibiotics.
titioners in the early stages of the disease in order to
Of the group A patients, one remained sputum
prevent the prolongation of the treatment course and
culture-positive for M. tuberculosis and died of TB 15
the progressive destruction of lung tissue which will
months post-operatively. The other five patients
render subsequent resection impossible.
(83.3%) underwent sputum conversion and remained
Based on previous experience with unfavourable
negative for a mean duration of 41 months post-
responses for similar patients, we were prompted to
operatively (range 5–61). In group B, one patient died
perform surgery for group B patients in the early
on the seventh day post-operatively; 13 of the remain-
stages of their treatment. Whilst we did not conduct a
ing 14 patients (92.8%) demonstrated sputum con-
randomised controlled trial for this group of patients,
version and/or remained negative for a mean duration
comparing our results with historical control,3 the
of 42.8 months (range 23–80) post-operatively, and one
high success rate suggests that surgical intervention in
patient remained sputum culture-positive and remained
early stages of treatment may constitute a good
on treatment. In group C, all five patients received
adjunct to the effective treatment of MDR-TB. Group
post-operative treatment for a mean of 13.2 months
C patients were prepared for surgical intervention in
(range 11–19), and all completed treatment. How-
the late stages of their treatment. The only patient
ever, over a mean of 22 follow-up months (range 15–
who experienced disease relapse was in group C, which
64), one patient relapsed (20%). This patient had
made the benefit of surgery for group C patients
received second-line anti-TB treatment regularly for a
appear less clear. In this study, the relative success of
period of 19 months pre-operatively, and had under-
treatment in each sub-group may remain uncertain
gone RUL and RML lobectomy and right B6 segmen-
tal resection, followed by 18 months post-operative
In a report by Goble et al.2 of the results of treating
treatment; however, she relapsed 40 months post-
171 pulmonary MDR-TB patients, in 134 patients
operatively, revealing sputum culture positivity for
with sufficient follow-up data the overall response
M. tuberculosis. The drug-resistant patterns of the
rate was 56% over a mean period of 51 months.
pre- and post-operative organisms were similar, and
Using univariate analysis, four factors were associ-
the cause of her relapse is obscure. She commenced
ated with the failure to sterilise sputum cultures: pre-
The International Journal of Tuberculosis and Lung Disease
vious administration of more anti-tuberculosis drugs,
resistant to more drugs (уfour), the potential utility
regimens including fewer previously unused drugs, in
of surgical intervention should be evaluated. By con-
vitro organism resistance to more anti-tuberculosis
trast, for patients exhibiting primary MDR-TB,16
without evidence of cavity upon CXR, with isolates
The positive contribution of surgery to the effec-
susceptible to more drugs, with more second-line
tive treatment of pulmonary MDR-TB has been
drugs not having been used previously, and demon-
reported previously. In the work of Iseman et al.,5 29
strating good tolerability and rapid clinical response
TB patients were selected for resection to supplement
to second-line drugs, surgery to treat this disease may
chemotherapy. There was no mortality associated with
surgery, but two unrelated deaths occurred subse-quently. Of the 27 survivors, 25 (92%) have remained
CONCLUSION
sputum culture negative for a mean duration of 36months. Recently, Leuven et al.11 reported the results
For selected patients who have predominantly loca-
of a group of 62 patients undergoing pulmonary
lised disease, pulmonary resection could improve the
resection as an adjunct to MDR-TB treatment. Treat-
outcome in the treatment of pulmonary MDR-TB.
ment outcome revealed that 80% remained free of
However, even if we are aggressive with respect to our
decision to perform surgery with patients suffering
A recent report of a good outcome in the treatment
from MDR-TB, treating such patients remains a great
of MDR-TB may question the role of surgery in the
challenge. Most patients suffer from MDR-TB due to
treatment of MDR-TB. Telzak et al. investigated the
previous irregular medication, and have a history of
treatment response in 26 HIV-negative MDR-TB
long-term medical treatment for this condition. Years
patients in New York.12 The clinical response rate to
of treatment usually result in extensive lung destruc-
chemotherapy in this group of patients was 96%, and
tion and poor lung function, which renders subse-
the authors concluded that contrary to previous
quent surgery impossible. Surgery is thus not the pan-
reports from Denver, HIV-negative patients with
acea to the challenge of MDR-TB. One of the few
MDR-TB responded well to appropriate chemother-
currently available mechanisms for reversing the omi-
apy. However, Iseman and Goble responded by refer-
nous threat of MDR-TB is ensuring regular medica-
ring to differences between the Denver2 and New
tion, such as by way of directly observed therapy, so
York12 studies, namely, and most importantly, that
as to reduce the likelihood of the emergence of bacte-
the patients in the Denver study had developed more
extensive drug resistance13 and such considerable dif-ferences probably contributed to the different success
The authors would like to thank Professor Michael D Iseman for
In a Korean report of a good outcome of treating
MDR-TB, Park et al. reviewed the clinical course of107 Korean patients with pulmonary MDR-TB.15 Of
the 63 patients with sufficient follow-up, 52 (82.5%)
1 Combs D L, O’Brien R J, Geiter L J. USPHS Tuberculosis
responded to chemotherapy.15 This study and the
short-course chemotherapy trial 21: effectiveness, toxicity, and
results from the Denver study2 are helpful in describ-
acceptability. Ann Intern Med 1990; 112: 397–406.
2 Goble M, Iseman M D, Madsen L A, et al. Treatment of 171
ing the TB patient who may most benefit from sur-
patients with pulmonary tuberculosis resistant to isoniazid and
gery. In the Korean study, similarly to the Denver
rifampin. N Engl J Med 1993; 328: 527–532.
study, patients who failed a retreatment regimen
3 Yu M C, Chien H P, Suo J, Lin T P. Treatment of multidrug-
using second-line drugs and demonstrating the pres-
resistant tuberculosis. Thorac Med 1995; 10: 85–90.
ence of a cavity on CXR, as well as those with isolates
4 Pablos-Mendez A, Raviglione M C, Laszlo A, et al. Global sur-
resistant to more drugs, experienced a less favourable
veillance for antituberculosis-drug resistance, 1994–1997. NEngl J Med 1998; 338: 1641–1649.
response than patients who failed initial treatment
5 Iseman M D, Madsen L, Goble M, Pomerantz M. Surgical in-
who showed no evidence of cavity and whose isolates
tervention in the treatment of pulmonary disease caused by
drug-resistant Mycobacterium tuberculosis. Am Rev Respir
Surgery, a high-cost intervention with a moderate
risk of complication, is indicated for those patients
6 Bai K J, Yang S L, Yu M C, et al. Tuberculosis in Taiwan, 1997.
who would be likely to derive the most benefit, and is
7 Department of Health, the Executive Yuan, ROC: Health and
considered unnecessary for patients who may respond
vital statistics-1. General health statistics 1997, Republic of
to medical treatment alone. Until the results of a ran-
domised control trial of the surgical management of
8 Chiang I H, Yu M C, Bai K J, et al. Drug resistance patterns of
MDR-TB become available, we advise that for patients
tuberculosis in Taiwan. J Formos Med Assoc 1998; 97: 278–282.
demonstrating persistent cavitary lesions upon CXR, a
9 Yu M C, Suo J, Chiang C Y, Bai K J, Lin T P, Luh K T. Initial
previous history of multiple relapse, a retreatment
drug resistance of Mycobacterium tuberculosis in Taiwan. J
history using more second-line drugs, and/or isolates
Formos Med Assoc 1997; 96: 890–894. Pulmonary resection in the treatment of MDR-TB
10 Chiang C Y, Wu I H, Yu M C, et al. Screening of human immu-
13 Iseman M D, Goble M. Multidrug-resistant tuberculosis. N
nodeficiency virus infection in pulmonary tuberculosis patients
in Taiwan. J Formos Med Assoc 1998; 97: 66–68.
14 Telzak E E, Sepkowitz K. Turett G. Multidrug-resistant tuber-
11 Leuven M V, Groot M D, Shean K P, Oppell U O V, Willcox
culosis. N Engl J Med 1996; 334: 269.
P A. Pulmonary resection as an adjunct in the treatment of
15 Park S K, Kim C T, Song S D. Outcome of chemotherapy in
multiple drug-resistant tuberculosis. Ann Thorac Surg 1997;
107 patients with pulmonary tuberculosis resistance to iso-
niazid and rifampin. Int J Tuberc Lung Dis 1998; 2: 877–884.
12 Telzak E E, Sepkowitz K, Alpert P, et al. Multidrug-resistant
16 Bai K J, Yu M C, Chiang C Y, Hsu C J, Wu M P, Lin T P. Treat-
tuberculosis in patients without HIV infection. N Engl J Med
ment of pulmonary multidrug-resistant tuberculosis. Thorac
R É S U M É C A D R E : Le Bureau de Lutte contre les Maladies Chro- localisée ; 3) réserve cardio-pulmonaire adéquate ; 4) niques, Département de la Santé, T’ai-wan. réduction préalable de la charge mycobactérienne grâce O B J E C T I F : Evaluer le rôle de la résection pulmonaire à un régime de traitement comportant au moins deux dans le traitement des tuberculoses pulmonaires à produits efficaces. germes résistant à la fois à l’isoniazide et à la rifampicine R É S U L T A T S : La mortalité chirurgicale se limite à un (TB-MR). décès péri-opératoire (4%). Des complications sont sur- S C H É M A : Cette étude rétrospective de cohorte a passé venues chez trois patients (11%) et la négativation de en revue 27 patients TB-MR qui avaient subi une résec- l’expectoration ou la persistance de la négativité ont été tion pulmonaire entre décembre 1990 et mars 1999. Les observées après l’intervention chez 24 patients (92%). régimes de traitement individualisés ont été sélectionnés Le traitement est déjà terminé chez 23 patients et, au lors de réunions hebdomadaires du personnel, après cours d’un suivi moyen de 42 Ϯ 18 mois (extrêmes 15– revue de l’histoire du cas et des résultats de la sensibilité 80 mois), il n’y a eu qu’une seule rechute. Ce patient a aux médicaments. On a pratiqué la chirurgie chez des été stabilisé après une nouvelle cure. patients sélectionnés, essentiellement pour les raisons C O N C L U S I O N : Chez les patients sélectionnés, la résec- suivantes : 1) échec du traitement médical ou haute tion pulmonaire peut améliorer les résultats dans les probabilité d’échec du traitement ou rechute paraissant tuberculoses pulmonaires à germes multirésistants. probable après traitement ; 2) maladie à prédominance M A R C O D E R E F E R E N C I A : Oficina de Control de Enfer- predominio de enfermedad localizada ; 3) con reservas medades Crónicas, Departamento de Salud, Taiwan. cardiopulmonares adecuadas ; 4) cuando el esquema te- O B J E T I V O : Evaluar el papel de la resección pulmonar en rapéutico contenía por lo menos dos drogas eficaces el tratamiento de la tuberculosis pulmonar resistente a la para disminuir la carga micobacteriana. isoniacida y a la rifampicina (TB-MR). R E S U L T A D O S : No hubo mortalidad quirúrgica, excepto M É T O D O : Un estudio retrospectivo de una cohorte de una muerte peri-operatoria (4%). Tres pacientes (11%) 27 pacientes con TB-MR que fueron sometidos a una tuvieron complicaciones y 24 (92%) mostraron conver- resección pulmonar entre diciembre de 1990 y marzo de sión del esputo y/o permanecieron negativos después de 1999. Se indicaron esquemas terapéuticos individuales la operación. Veintitrés pacientes han completado el adecuados en reuniones semanales del equipo donde se tratamiento y durante un promedio de seguimiento de presentaban la historia del paciente y los resultados de la 42 Ϯ 18 meses (rango 15–80 meses) un paciente sensibilidad a las drogas. Se efectuó la cirugía en recayó. Este paciente curó después de otro período de pacientes seleccionados, especialmente en los siguientes : tratamiento. 1) cuando había fracasado el tratamiento médico, o en C O N C L U S I Ó N : Para algunos pacientes seleccionados la quienes el fracaso era muy probable, o en aquellos en los resección pulmonar puede mejorar el resultado de la TB- que la recaída post-tratamiento era probable ; 2) con MR pulmonar.
INCIDENCE OF SEXUAL DYSFUNCTION DURING THE PERI- AND POSTMENOPAUSE From the literature it appears that the prevalence of sexual problems Sexual dysfunction in the in women is high, that the prevalence increases with age, and thatthe menopausal transition has a negative influence on sexuality [2- peri- and postmenopause 8]. The prevalences of sexual dysfunctions may be underestimatedin
Vaccinations, medications, etc. (from www.mdtravelhealth.com/destinations/africa/ uganda .php) Summary of recommendations : All travelers should visit either their personal physician or a travel health clinic 4-8 weeks before departure. Vaccinations: Hepatitis A Yellow fever Required for all travelers. Proof of vaccine is required for submission with visa paperwork. Re
 The International Journal of Tuberculosis and Lung Disease
The International Journal of Tuberculosis and Lung Disease