Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
1end.0115
The new england journal of medicine
Tobacco Control in the Wake of the 1998 Master Settlement Agreement
Tobacco takes an enormous toll on the health of the den, and many of the developing countries. By con-public as the cause of 440,000 deaths annually in the trast, smoking rates among women in the UnitedUnited States and 4.8 million deaths worldwide.1,2 States are in the highest third for women worldwide. An estimated 8.6 million persons in the United Globally, smoking rates among men are highest inStates have serious smoking-related illness.3 The Asia (e.g., 67 percent in China, 65 percent in Korea,World Health Organization projects that by the year and 53 percent in Japan), but the rates are also high2030 the use of tobacco will kill 10 million persons in Russia (63 percent), Yugoslavia (52 percent), andannually — including 7 million in developing coun- Mexico (51 percent). In almost all nations, womentries — which will make tobacco use the world’s are much less likely to smoke than men; amongleading cause of preventable death.4
women, the smoking rate is a mere 4 percent in Chi-
In 2001, the prevalence of smoking in the United na and in Korea (and the rate is even lower in most
States stood at 25.5 percent among men and 21.5 Arab countries) but is about 33 percent in Argentinapercent among women, down from the peaks of 57 and Norway.4percent among men in 1955 and 34 percent among
In the relatively few countries that have anti-
women in 1965.5 Rates of smoking have plateaued, tobacco policies, government has provided the es-however, since 1990.5 The prevalence varies by state, sential leadership; the exception is the United States,ranging from 31 percent in Kentucky to 13 percent where grassroots action and litigation by citizensin Utah, and it is increasingly concentrated in pop- have generated most of the changes, includingulations that have relatively little education and low changes that were mediated by laws and regula-incomes.6 Smoking rates are declining in all age tions.15 In the face of an aggressive tobacco indus-groups, except among persons 18 to 24 years of age, try that in 2001 spent $11.2 billion on advertisingamong whom the prevalence rose from 23 percent and promotion in the United States alone,16 effec-in 1991 to 27 percent in 2000.7
tive control of the use of tobacco requires multiple
Mental illness and smoking have been closely policy strategies. Most of the promising approach-
linked. For example, smoking rates have been re- es have not been fully implemented.17-20ported to be over 80 percent among persons who
In this Special Report I review the landmark
have schizophrenia,8,9 50 to 60 percent among per- $209 billion Master Settlement Agreement (MSA)sons with depression,10 55 to 80 percent among of 1998 between 46 states and the U.S. tobacco in-those who have alcoholism,11,12 and 50 to 66 per- dustry and, after a brief history of the MSA, assesscent among those who have substance-abuse prob- its strengths and limitations as an instrument oflems.12,13 One study estimated that smokers with tobacco control. Current U.S. tobacco-control pol-coexisting psychiatric or substance-abuse disorders icies at the federal, state, and local levels are summa-account for 44 percent of all cigarettes smoked in rized, with an emphasis on recent developments inthe United States, a percentage that reflects both the the area of policy. high prevalence of smoking in connection withthese conditions and the fact that patients with these
Worldwide, it is estimated that 47 percent of men
but only 12 percent of women smoke.14 As com- The background and terms of the MSA between fourpared with smoking rates among men in other major tobacco companies (Brown & Williamson,countries, in the United States the rate ranks in the Lorillard, Philip Morris, and R.J. Reynolds) and thelowest fifth, but it is higher than in Australia, Swe- states’ attorneys general illustrate the tension be-
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved. The new england journal of medicine
tween the tobacco interests and those working to panies for their deceptive practices.23 Because theprotect the public’s health, as well as the conflicting MSA did not address federal regulation or federalpressures faced by those making tobacco-control programs, it did not require congressional approval. policy in a time of budget deficits. t e r m s o f t h e a g r e e m e n t b a c k g r o u n d
In exchange for the states’ abandonment of their
In 1994, which was the year in which David Kessler, suits, the tobacco companies awarded the statesthen the commissioner of the Food and Drug Ad- $206 billion, to be paid over a period of 25 yearsministration (FDA), asserted the agency’s authority and to be used by each state at its own discretion. to regulate tobacco products, Michael Moore, the After that time, payments will continue to be basedattorney general of Mississippi, and Hubert Hum- on the volume of domestic cigarette sales by the fourphrey III, the attorney general of Minnesota, sued companies. Because state attorneys general do notthe large tobacco companies to recover the costs to have authority over state spending, the MSA was si-their states’ Medicaid programs of treating tobacco- lent with regard to the ways in which the statesrelated illnesses. Every state in the country soon fol- would spend their funds. Indeed, with the exceptionlowed their lead. In 1996, a group of attorneys gen- of the creation by the MSA of the American Legacyeral, private attorneys, public health advocates, and Foundation for public education and other tobacco-tobacco-industry representatives began closed-door control activities, which was to be supported for atmeetings to discuss a global settlement, as it was least five years at a cost of approximately $1.7 bil-called, of all public and private litigation. At about lion, no funds were earmarked by the settlement. the same time, Florida, Mississippi, Texas, and Min- Nevertheless, at the time of the settlement manynesota settled with the tobacco companies on their states declared their intent to use the funds to helpown. In June 1997, details of the global settlement defray the costs to Medicaid of smoking-induced ill-were announced. It required Congress to grant the nesses.24 In addition, the MSA required the disso-tobacco industry limited immunity from new law- lution of the Tobacco Institute and other industry-suits for past actions and to enact certain public promoting organizations, prohibited advertisinghealth provisions. Many advocates of tobacco con- targeted to young people (e.g., the use of cartoontrol, most notably former surgeon general C. Everett characters such as “Joe Camel” and billboard ad-Koop, Kessler, and Stanton Glantz of the University vertising), and permitted wide dissemination of in-of California at San Francisco, criticized the global dustry documents that had previously been kept se-settlement as not going far enough.21
In April 1998, legislation to implement the glob-
al settlement — which was sponsored by Senator limitations John McCain (R-Ariz.) and strengthened in response Many tobacco-control elements that had been part to criticisms by advocates of tobacco control — was of the general settlement were dropped from the voted out of the Senate Commerce Committee by a MSA; these included the assignment of jurisdiction vote of 19 to 1 (with the one negative vote cast by over tobacco to the FDA, strengthened warnings on then senator and now attorney general John Ash- packages of tobacco, tighter enforcement of rules croft).22 However, the legislation never came to a banning the sale of tobacco to minors, and strong vote in the full Senate, because its supporters failed regulations in support of clean indoor air.26 The by three votes to overcome a filibuster. The general MSA also included language that later hampered ef- settlement faltered owing to lukewarm support by forts aimed at tobacco control. For example, the the Clinton administration, ambivalence on the part bulk of the funding for the American Legacy Foun- of the public health community, and vigorous op- dation expired after five years, because the funds de- position from the tobacco industry, which spent pended on the four settling tobacco companies’ $50 million on a two-month campaign that was maintaining a share of the domestic cigarette mar- waged against the proposed legislation.21
ket of at least 99.05 percent.28 In retrospect, that
Six months later, in November 1998, the attor- percentage was probably based on erroneous pro-
neys general of the 46 states that had remained party jections. to the suit did reach an agreement, called the MSA,
In the current climate of fiscal crises, the MSA
with the four large tobacco companies to recover funds have become an irresistible target from thetheir Medicaid expenses and to penalize the com- perspective of state policymakers to help address
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
budget deficits and avert new taxes.26,29 In many Thus, the MSA has created perverse incentives for states, important tobacco-control activities — such the states to keep the tobacco industry financially as the landmark antismoking programs in Minne- healthy. sota, Massachusetts, and Florida — are being dis- mantled. For example, in 2003 state antitobacco strengths budgets were slashed by 99 percent in Florida and Matt Myers, director of the Campaign for Tobacco- by 92 percent in Massachusetts. Even before the cur- Free Kids and a major figure in the global-settlement rent fiscal crisis, less than 5 percent of state funds discussions,21 said in an interview that he credits the from the MSA was spent on tobacco control, and MSA with “the most significant increase in spend- some states spent essentially nothing.25,29 In fiscal ing on tobacco prevention and cessation in history. year 2003, 47 percent of the MSA payments went These funds have forever changed the debate about into state budgets, which represents a sharp in- the appropriate level of funding for tobacco con- crease from 29 percent in the previous fiscal year trol.” Certainly, even the paltry state expenditures and from 16 percent in the three preceding fiscal broadened national tobacco-control efforts far be- years.24 Some might argue that because smoking- yond the earlier isolated examples of state spending related Medicaid spending contributes to the states’ for this purpose. The MSA funded the first impor- budget deficits, the use of payments from the MSA tant national countermarketing effort in 30 years fund to reduce the deficits is appropriate. Senator (the American Legacy Foundation’s “truth” cam- McCain, however, thinks otherwise and on Novem- paign), which, along with increased tobacco taxes ber 12, 2003, held hearings on the use of the settle- and other factors, has reduced the smoking rate ment funds. He opened the hearings by criticizing among young people to a 27-year low.33 the National Governors Association and the Nation-
To pay for the antitobacco programs required un-
al Council of State Legislators for failing to fulfill der the MSA, tobacco companies have increased thetheir promises.30 According to McCain, at the time price of cigarettes by 45 cents a pack. Given that theof the settlement there was general agreement that price elasticity of demand for tobacco in the Unitedthe money would be used “for tobacco education States is about ¡0.4 — that is, for every 10 percentand treatment of smoking-related illnesses.”24
increase in price, there is a 4 percent decrease in de-
The states are increasingly mortgaging future mand — the increase may turn out to be the most
payments from the MSA through bond issues and important antitobacco benefit of the MSA, leadingare thereby forfeiting future income for the sake of to both the prevention of smoking and smoking ces-a smaller bird in the hand. To date, 20 states and the sation.34 High prices, however, may merely raise theDistrict of Columbia have either securitized their fu- age at which people start to smoke.35ture MSA payments or announced their intention to
The MSA has also made more tobacco-industry
do so31 (Gallogly M, Campaign for Tobacco-Free documents available. Researchers across the coun- Kids: personal communication). These transactions try are poring through these documents and pub- are known as “naked bonds,” because they transfer lishing new revelations based on them about indus- risk to the investors, with no state guarantee of pay- try practices and tactics.36-38 ment. Recently, however, New York and California have sold tobacco bonds that were backed by state winners and losers tax revenues. These states now have a financial in- Of course, it would be easier to assess the effects of centive to keep the tobacco industry healthy, because the MSA if it were possible to know what would have if the companies forfeit their MSA payments, the fi- happened had the 46 settling states instead pursued nancial obligations will revert to the states.32 In an separate litigation. How many suits would have example of the states’ protectiveness toward the to- come to trial, and with what results? How many bacco industry, this year 37 state attorneys general states would have settled separately, and what set- supported the successful effort by Philip Morris to tlements would have been reached? Although the reduce a $12 billion bond that had been ordered by answers to these questions will never be known, the an Illinois judge as part of a private suit that is cur- consensus that has emerged is that the public lost a rently under appeal. The states’ concern was that if golden opportunity to improve its health. For ex- the tobacco companies were to be bankrupted as a ample, the two state attorneys general most involved result of high, court-mandated judgments, then the in both the global settlement and the MSA — Chris- payments to the states under the MSA would cease. tine Gregoire of Washington and Michael Moore of
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved. The new england journal of medicine
Mississippi — as well as tobacco-control experts restaurants, and bars or not — as compared with in-such as economist Ken Warner of the University of terventions such as countermarketing. And granted,Michigan, wish that the states had been more com- there may be mitigating factors, such as the extentmitted to tobacco control. In Moore’s words, “I call to which cigarette smuggling lowers selling pricesit moral treason. The losers are the people in the or the extent to which laws to promote clean indoorstates where the legislators have chosen to spend air are enforced. But such factors pale beside the var-the money on budget deficits instead of long-term iable implementation of, for example, countermar-investment in health.”24
keting efforts (the quality of the advertisements, the
Some saw the tobacco industry as the clear victor. frequency with which they are aired, and the audi-
For instance, Myers said in an interview that the set- ences to which they are targeted). And, in part, thetlement of “the most serious litigation threat the evidence reflects the likelihood that raising taxesindustry had ever faced, under terms that had little and imposing clean-indoor-air regulations mayimpact on how it conducts its business and at a cost simply be more robust ways to reduce tobacco useit was able to pass on to its consumers,” was a boon than implementing programs to prevent peopleto the industry. Glantz, in an interview, took an even from starting to smoke or to promote smoking ces-darker view: “Probably the tobacco industry will win sation. in the long run, largely because of the securitization
A full discussion of all the tobacco-control poli-
of the money putting pressure on states to keep to- cies listed in Table 1 is not possible here. Accord-bacco consumption up to get their bonds paid off.” ingly, I shall focus on four policies — tobacco taxes,
Glantz and Joseph Califano, Jr., the former sec- clean-indoor-air requirements, smoking-cessation
retary of Health, Education, and Welfare and now programs and services, and a convention on tobac- the president of the National Center for Addiction co control sponsored by the World Health Orga- and Substance Abuse at Columbia University, are nization. skeptical that Congress will ever pass global settle- ment–type legislation. “The MSA results from the taxation failure of the U.S. Congress and most state legis- The price elasticity of the demand for cigarettes is latures to do their jobs,” Califano said in an inter- estimated to range from ¡0.3 to ¡0.5, indicating a view. “The result: the money is being spent to close decrease in demand of 3 to 5 percent for every in- budget deficits rather than to stop kids from smok- crease of 10 percent in price.19,34 Thus, it would ing and help adults who are hooked. On balance, appear that one of the best ways to reduce smoking however, I believe we are far better off with the MSA is to raise the cost of tobacco products through tax- than without it, because the alternative was noth- ation, thereby both encouraging smoking cessation ing from a Congress that continues to pander to and discouraging the initiation of smoking. Be- the tobacco interests.”
tween 1993 and 2002, the federal tax on cigarettesrose from 24 cents to 39 cents per pack. In 2002, thefederal Interagency Subcommittee on Cessation,
f e d e r a l , s t a t e , a n d l o c a l
created by the secretary of Health and Human Ser-
t o b a c c o - c o n t r o l p o l i c i e s
vices, Tommy G. Thompson, proposed raising the
For policymakers, there are three ways to reduce the tax to $2.39 per pack and using the resultant reve-harm caused by the use of tobacco: prevent initia- nues to fund comprehensive smoking-cessationtion, encourage smoking cessation, and limit expo- programs and services, a recommendation that wassure to secondhand smoke. The universe of tobac- rejected by the administration of President Georgeco-control policies encompasses a wide variety of W. Bush.59interventions that have had varying and often untest-
The rates of cigarette taxes vary greatly from state
ed efficacy39 (Table 1). As summarized in 2000 in to state, ranging from a low of 2.5 cents per pack inthe surgeon general’s report on reducing tobacco Kentucky to a high of $2.05 per pack in New Jersey,use, “A hierarchy of effectiveness is difficult to con- for an average of 66 cents per pack. Not surprisingly,struct.”19 That said, the evidence seems strongest tobacco taxes are generally lower in states that growfor the effect of tobacco taxes34 and legislation to tobacco and in those that have more smokers.25 In-promote clean indoor air.58 In part, this reflects the creases in state taxes either can be legislated or canease of measuring these effects — taxes are either result from ballot initiatives, such as the passage oflevied or not, smoking is either banned in offices, Proposition 99 in California in 1988.60 Recent bud-
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved. Table 1. Tobacco-Control Policies.* Area of Policy Evidence and History Fiscal control
Federal, state, and local taxes Good evidence exists that the use of tobacco products is sensitive to price and that raising taxes discourages
In 1982, Congress stabilized tobacco prices paid to farmers. Special additional payments can be authorized,
as in 2000 and 2001. In 2003, the tobacco crop yield was the lowest since 1874; it has declined 40 percent since 1997. Federal legislation now being considered would phase out price stabilization and buy out tobacco farmers for $13 billion.40-44
Regulatory controls
Good evidence exists that bans on smoking in workplaces, bars, and restaurants induce smokers to quit or
In 1994, the FDA sought federal regulation of the content of tobacco products but in 2000 this was rejected by
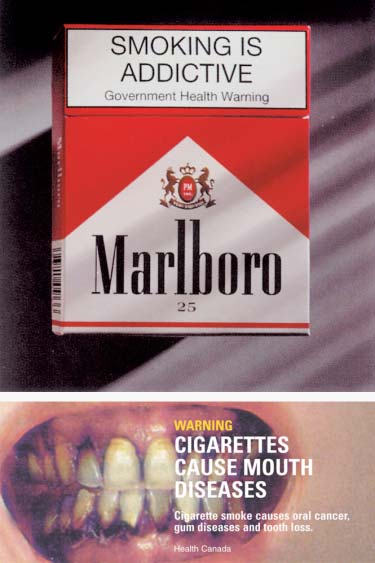
the Supreme Court. Nicotine-replacement therapy is regulated by the FDA, but not nicotine-containing cigarettes. Warning labels on tobacco products, which are required by Congress, are weak as compared with those in Australia and Canada (Fig. 1).45-48
In 1969, federal law banned radio and television advertising of tobacco products but simultaneously ended
federal counteradvertising. Terms such as “low tar” and “light” remain unregulated. Some states (California, Massachusetts, and Florida) have conducted aggressive counteradvertising campaigns.49-52
Local enforcement varies. The provision in the Synar Amendment (1992) that calls for linking federal funds
for substance-abuse treatment to enforcement of restrictions on sales to minors has not been enforced. Minors can easily purchase cigarettes over the Internet. There is no evidence that restrictions on sales to minors, even if enforced, would reduce smoking among young people.53-56
Litigation
The lawsuit initiated by the Department of Justice in 1999 under the Clinton administration and brought
forward by the present attorney general, John Ashcroft, seeks the payment of $289 billion for reason of “fraudulent and deceptive marketing practices.” A trial date has been set for September 15, 2004, though many predict a settlement. Smoking-cessation programs†
Government health systems, Although rates of smoking cessation are low, small increases in quitting owing to the use of treatments that
have proved to be efficacious (counseling, nicotine-replacement therapy, and drugs such as bupropion) could have a substantial effect on the population of smokers. Because government pays for half of all health care expenditures through Medicare, Medicaid, VHA, Indian Health Services, the military, and pro-grams for federal employees, government policies to promote smoking cessation are critical, as is govern-ment support of telephone quit lines. Coverage for smoking-cessation treatment is limited, although the VHA has set important diagnostic and treatment goals. There is no government support for establishing a national telephone quit line. Research on prevention and cessation
Many questions remain unanswered regarding the initiation of smoking, pathways to nicotine addiction,
patterns of smoking, successful smoking-cessation treatments, and the coexistence of smoking with psychiatric and substance-abuse disorders. No one government agency “owns” smoking research. Expenditures for research are very small in relation to the size of the problem (the NIH spent less than 1 percent of its 2002 budget on such research‡). A few states, notably California, fund such research. Visible national leadership
There is no visible antitobacco champion in the Bush administration. Periodic reports from the surgeon gen-
eral, the CDC, and Healthy People highlight smoking-related issues in the United States.6,7,19,57
Satcher, former FDA com-missioner David Kessler, and periodic reports on the prevalence of smoking
International trade†
The FCTC, sponsored by the World Health Organization and including many tobacco-control policies, was
adopted by the World Health Assembly in May 2003. Whether the FCTC will be ratified and, if ratified, whether it will be successfully implemented will be influenced by the extent of support for it by the United States.
* FDA denotes Food and Drug Administration, VHA Veterans Health Administration, NIH National Institutes of Health, CDC Centers for Dis-
ease Control and Prevention, and FCTC Framework Convention on Tobacco Control.
† See text for further details. ‡ Information is from Curtis ET, National Cancer Institute: personal communication.
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved. The new england journal of medicine
get crises have goaded many states to raise tobacco battlefields for legislation to promote clean indoor taxes: 21 states raised this tax in 2002, and another air; 20 states have passed such legislation in order 17 in 200361 (Gallogly M, National Center for To- to preempt efforts by local communities to enact bacco-Free Kids: personal communication). Munic- stricter clean air laws than those required by (usually ipal taxes provide a less powerful deterrent, because relatively weak) state statutes (Hallett C, Americans residents can easily purchase cigarettes nearby, for Nonsmokers’ Rights: personal communication). where a lower tax is levied. Still, some cities impose Attempts by the Occupational Safety and Health Ad- a substantial tax; in New York City, the tax of $1.50 ministration to control tobacco smoke in the work- raised the cost of a pack of cigarettes to more than place nationwide were defeated in 2001, after a $7. The effect of tobacco taxes can be blunted by lengthy campaign by the tobacco industry.66 smuggling, which has become an international is- sue; countries vary greatly in the vigor with which support of smoking-cessation programs they combat smuggling.62,63
Of the 46 million smokers in the United States, 70percent would like to quit, but each year less than
c l e a n - i n d o o r - a i r i n i t i a t i v e s
5 percent of these smokers are able to quit with-
The creation of smoke-free public areas has been a out assistance.67 The odds of successfully quittingmajor success of the antitobacco movement in the smoking can be doubled or even tripled if counsel-United States. A poll conducted in 1978 for the now- ing, nicotine-replacement therapy, and treatmentdefunct Tobacco Institute showed that the non- with drugs such as bupropion are used.68 Becausesmokers’-rights movement “is the single greatest government pays half of all health expenditures inthreat to the viability of the tobacco industry.”64 the United States, its payment policies greatly influ-Mounting evidence of the dangers of secondhand ence smoking-cessation practices. Medicaid coverssmoke catalyzed action to create smoke-free areas some services and drug therapy in support of ces-and gave added support to the nonsmokers’-rights sation in 34 states, but a 2001 study of 2 of thesemovement, which included the rights of workers states showed that only a small percentage of pa-in such industries as transportation and entertain- tients and providers were aware of the coverage.69ment. Especially important was the decision of the Medicare does not yet cover prescription drugs, norEnvironmental Protection Agency in 1993 to classify does it provide a separate payment for outpatientsecondhand smoke as a carcinogen.65 The estab- smoking-cessation counseling. Coverage for smok-lishment of smoke-free areas has undermined the ing-cessation programs for federal employees issocial acceptability of smoking, and concern about also spotty. Neither the military, despite its historysecondhand smoke has served to counter the tobac- of giving free cigarettes to the troops, nor the Indianco industry’s claim that smoking is a matter of in- Health Service, which provides health care to a pop-dividual choice.
ulation that smokes heavily, has developed a com-
Since 1973, federal legislation has required pas- prehensive program to identify and treat smokers.
senger airlines to establish separate sections in the
The Veterans Health Administration (VHA) is
airplanes for smoking and nonsmoking passengers poised to serve as a model health care system foron domestic flights, and it now bans smoking on all smoking cessation. Among veterans, the smokingdomestic flights, on all flights to and from the Unit- rate is higher than that in the general population, 33ed States, and in most U.S. airports.15 Five states — percent as compared with 23 percent, and veteransCalifornia, New York, Delaware, Connecticut, and are heavier smokers as well. Among veterans of theMaine — have banned smoking in essentially all Vietnam war, the prevalence of smoking is 47 per-public places, including work sites, restaurants, and cent.70 In 1997, the VHA mandated that veteransbars. (The Massachusetts legislature has passed cared for in its system be asked about smoking andsimilar legislation, and Governor Mitt Romney has that smokers be counseled. Subsequently, the re-announced his intention to sign the bill when it ported percentage of veterans asked about smokingreaches his desk, in early 2004.) Another 32 states rose from 49 percent in 1996 to 95 percent by 1999,have imposed partial restrictions against smoking. and the reported percentage of smokers counseledMore than 1600 counties and municipalities have increased from 33 percent in 1996 to 93 percent bypassed laws to promote clean indoor air (Hallett C, 1999.70 These rates are substantially higher than theAmericans for Nonsmokers’ Rights: personal com- rate among members of the private health plan thatmunication). Increasingly, the states have become was reported to have the best performance (68 per-
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
cent of smokers received advice to quit), accord-ing to the National Committee for Quality Assur-
ance.71 Only 38 percent of all smokers covered byMedicare who were hospitalized as the result of anacute myocardial infarction in 2000 and 2001 re-ceived smoking-cessation counseling, as comparedwith 62 percent of similar patients in VHA facilitiesin 2000.72 Fewer than half of the smokers receivingcare from the VHA, however, received drug therapyto aid smoking cessation, reflecting variable localcoverage policies.70
Telephone “quit lines,” which are available in
32 states and are available nationally through theAmerican Cancer Society and the National CancerInstitute, greatly enhance the probability that smok-ers will quit, especially when the quit lines can pro-vide a personal interaction with callers. So far, how-ever, quit lines have been used by only a tiny minority
of smokers.29,73 Funding for quit lines depends onan unstable amalgam of state and voluntary sources,and as a result not all callers can be served.74 Twostates (Oregon and Michigan) closed their quit linesin 2003 because of budget constraints, and otherstates are poised to follow suit. A federally fundednational quit line that would have a toll-free numberand that would be linked with a media campaign to
Figure 1. Warnings on Cigarette Packages Produced in Australia (Panel A) and Canada (Panel B).
encourage smokers to call the number would be amajor help, as would support for Web-based smok-ing-cessation services.
Bush administration will support the FCTC remains
i n t e r n a t i o n a l t r a d e p o l i c i e s
to be seen. The U.S. tobacco industry, which had
Until recently, the United States opposed the Frame- worked to weaken the treaty, is expected to opposework Convention on Tobacco Control (FCTC), ratification. Even if the FCTC is ratified, the vigorwhich was sponsored by the World Health Organi- with which its provisions will be enforced will de-zation in 2003 and which bans tobacco advertising pend on the zeal of each country and will be greatlyto the extent permitted by each country’s constitu- influenced by the attitudes and practice of the Unitedtion, mandates aggressive warning labels (see, for States and its major tobacco-exporting companies. example, Fig. 1), requires a list of tobacco ingredi-ents on the packages, and imposes other controls
that would end the use of the terms “light” and“mild” on cigarette packages and would crack down There are four key ingredients of successful publicon tobacco smuggling.75 On May 21, 2003, shortly health efforts — highly credible scientific evidence,after the United States dropped its opposition, the passionate advocates, media campaigns, and lawFCTC was adopted by a voice vote of the 192 mem- and regulation, usually at the federal level.77 In thebers of the World Health Assembly.76 For the FCTC battle against the harmful effects of tobacco use, theto become a binding international treaty, it must be scientific evidence came first, almost 50 years ago,ratified by the legislative bodies of at least 40 na- and since then advocates of tobacco control havetions. For ratification, a country’s administration engaged in a four-decade battle against the U.S. to-must sign the treaty and then refer the treaty to its bacco industry.15 Except for a two-year national me-legislature for approval. To date, 77 countries have dia campaign against tobacco use in the late 1960s,signed the FCTC, but only Norway, Sri Lanka, Sey- there was little counteradvertising about tobaccochelles, Malta, and Fiji have ratified it. Whether the until the mid-1990s, and initially it was run in only
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved. The new england journal of medicine
a few states until the recent MSA-funded American the public health, and the unabashed triumph of Philip Morris. NewLegacy Foundation’s campaign. At the same time, York: Alfred A. Knopf, 1966. 16. Federal Trade Commission cigarette report for 2001. Washing-
government initiatives, particularly federal antito- ton, D.C.: Federal Trade Commission, 2003. (Accessed December bacco efforts, have been relatively weak. In addition 23, 2003, at http://www.ftc.gov/os/2003/06/2001cigreport.pdf.) to the 440,000 Americans who die each year from 17. Hopkins DP, Fielding JE, Task Force on Community Preventive
Services, eds. The guide to community preventive services: tobacco
smoking, another 8.6 million suffer from serious use prevention and control: reviews, recommendations, and expert tobacco-induced illness.3 Although U.S. smoking commentary. Am J Prev Med 2001;20:Suppl 2:1-88. rates are slowly declining, progress toward that end 18. National Center for Chronic Disease Prevention and Health Pro-
motion, Office of Smoking and Health. Best practices for compre-
would be faster if federal policymaking matched hensive tobacco control programs, August 1999. Atlanta: Centers both the rigor of the scientific evidence against to- for Disease Control and Prevention, August 1999. bacco use and the resolve of antitobacco advocates. 19. Department of Health and Human Services. Reducing tobacco
use: a report of the Surgeon General. Atlanta: Centers for Disease
Supported by the Robert Wood Johnson Foundation and the
Control and Prevention, National Center for Chronic Disease Pre-
Scholar in Residence program of the Rockefeller Foundation at the
vention and Health Promotion, Office on Smoking and Health,
Bellagio Study and Conference Center, Bellagio, Italy.
Dr. Schroeder is the unpaid chair of the American Legacy Founda-
20. National Cancer Policy Board. Taking action to reduce tobacco
tion, which is funded by the Master Settlement Agreement.
use. Washington, D.C.: National Academy Press, 1998.
I am indebted to Brian Eule, Elissa Keszler, Victoria Weisfeld,
21. Pertschuk M. Smoke in their eyes: lessons in movement leader-
Stephen Isaacs, and Garfield Mahood for their able assistance.
ship from the tobacco wars. Nashville: Vanderbilt University Press,2001.
From the Department of Medicine, University of California, San
22. Universal Tobacco Settlement Act §1415 (1998).
Francisco. Address reprint requests to Dr. Schroeder at the De-
23. Master Settlement Agreement between 46 state attorneys gen-
partment of Medicine, University of California at San Francisco,
eral and participating tobacco manufacturers. November 23,
3333 California St., Suite 430, San Francisco, CA 94143-1211, or
1998. (Accessed December 23, 2003, at http://naag.org/upload/
Annual smoking-attributable mortality, years of potential life
24. O’Connell V. States siphon off bigger share of tobacco-settle-
lost, and economic costs — United States, 1995–1999. MMWR
ment money. Wall Street Journal. October 9, 2003:A1. 25. Gross CP, Soffer B, Bach PB, Rajkumar R, Forman HP. State ex-
Ezzati M, Lopez AD. Estimates of global mortality attributable
penditures for tobacco-control programs and the tobacco settle-
to smoking in 2000. Lancet 2003;362:847-52.
Cigarette smoking–attributable morbidity — United States,
26. Givel G, Glantz SA. The “global settlement” with the tobacco in-
2000. MMWR Morb Mortal Wkly Rep 2003;52:842-4.
dustry: 6 years later. Am J Public Health (in press).
Quantifying selected major risks to health. World health report
27. Kessler DA, Myers ML. Beyond the tobacco settlement. N Engl J
2002. Geneva: World Health Organization, 2002. (Accessed Decem-
ber 23, 2003, at http://www.who.int/whr/2002/Chapter4.pdf.)
28. Healton C. Who’s afraid of the truth? Am J Public Health 2001;
Prevalence of current cigarette smoking among adults and
91:554-8. [Erratum, Am J Public Health 2001;91:828.]
changes in prevalence of current and some day smoking — United
29. Schroeder SA. Conflicting dispatches from the tobacco wars.
States, 1996–2001. MMWR Morb Mortal Wkly Rep 2003;52:303-4,
30. Center for Tobacco-Free Kids. Special reports: state tobacco
Prevalence of current cigarette smoking among adults, by area
settlement. (Accessed December 23, 2003, at http://www.
and sex — behavioral risk factor surveillance system, United States,
tobacccofreekids. org/reports/settlements/.)
2000. MMWR Morb Mortal Wkly Rep 2001;50:1103 (table). 31. Campaign for Tobacco Free Kids, American Lung Association,
Tobacco information and prevention source (TIPS). Atlanta:
American Cancer Association, American Heart Association, Smoke-
Centers for Disease Control and Prevention, 2003. (Accessed De-
Less States National Tobacco Policy Initiative. Show us the money:
cember 23, 2003, at http://www.cdc.gov/tobacco/research_data/
a report on the states’ allocation of the tobacco settlement dol-
lars. January 22, 2003. (Accessed December 23, 2003, at http://
Hughes JR, Hatsukami DK, Mitchell JE, Dahlgren LA. Preva-
tobaccofreekids.org/reports/settlements/2003/fullreport.pdf.)
lence of smoking among psychiatric outpatients. Am J Psychiatry
32. Pender K. State’s schizophrenic relations with tobacco. San
Francisco Chronicle. September 2, 2003:B1.
de Leon J, Abraham G, Nair C, Verghese C, McGrory A, McCann
33. Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future
E. Nicotine addiction in chronic schizophrenic inpatients. Biol Psy-
national survey results on drug use, 1975-2001. Vol. 1. Secondary
school students. Bethesda, Md.: National Institute on Drug Abuse,
10. Farnham CR. Zyban: a new aid to smoking cessation treatment
— will it work for psychiatric patients? J Psychosoc Nurs Ment
34. Chaloupka FJ, Warner KE. The economics of smoking. In: Cul-
yer AJ, Newhouse JP, eds. Handbook of health economics. Vol. 1B. 11. Hughes JR. Treating smokers with current or past alcohol de-
pendence. Am J Health Behav 1996;20:286-90. 35. Glied S. Is smoking delayed smoking averted? Am J Public 12. Lasser K, Boyd JW, Woolhandler S, Himmelstein DU, McCor-
mick D, Bor DH. Smoking and mental illness: a population-based
36. Hong MK, Bero LA. How the tobacco industry responded to an
prevalence study. JAMA 2000;284:2606-10.
influential study of the health effects of secondhand smoke. BMJ
13. Zickler P. Nicotine craving and heavy smoking may contribute to
increased use of cocaine and heroin. NIDA Notes. Vol. 15. No. 5. 37. Ling PA, Glantz SA. Why and how the tobacco industry sells cig-
2000:1. (Bethesda, Md.: National Institute of Drug Abuse.)
arettes to young adults: evidence from industry documents. Am J
14. Jha P. Curbing the epidemic: governments and the economics of
tobacco control. Washington, D.C.: World Bank, 1999:15. 38. Balbach ED, Gaslor RJ, Barbeau EM. R.J. Reynolds’ targeting of 15. Kluger R. Ashes to ashes: America’s hundred-year cigarette war,
African Americans: 1988-2000. Am J Public Health 2003;93:822-7.
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved. 39. Levy DT, Chaloupka F, Gitchel K. The effects of tobacco control
lanta: Centers for Disease Control and Prevention, Interagency
policies on smoking rates: a tobacco control scorecard. J Public
Committee on Smoking and Health, February 13, 2003. 60. California Tobacco Tax and Health Promotion Act of 1989 40. Womach J. Tobacco price support: an overview of the program.
CRS report for Congress. Washington, D.C.: Congressional Re-
61. State cigarette taxes & projected benefits from increasing them.
search Service, Library of Congress, May 7, 2001.
Washington, D.C.: National Campaign for Tobacco Free Kids, 2003. 41. Lindblom EN. False friends: cigarette companies’ betrayal of
(Accessed December 23, 2003, at http://tobaccofreekids.org/
American tobacco growers. Appendix III. Washington, D.C.: Na-
tional Center for Tobacco-Free Kids, 1999. (Accessed December 23,
62. Joossens L, Raw M. Turning off the tap: the real solution to cig-
2003, at http://tobaccofreekids.org/reports/falsefriends.)
arette smuggling. Int J Tuberc Lung Dis 2003;7:214-22. 42. The tobacco bailout. New York Times. September 15, 2003:A18. 63. Idem. How can cigarette smuggling be reduced? BMJ 2000;321: 43. Crop production. Washington, D.C.: National Agriculture Sta-
tistics Service (NASS), Agricultural Statistics Board, Department of
64. Hallet C. Rendez-vous interview 108. In: Boucher, P, ed. People
Agriculture, September 11, 2003. (Accessed December 23, 2003, at
and issues in tobacco control, 1999, 2000, 2001. Bainbridge Island,
http://jan.mannlib.cornell.edu/reports/nassr/field/pcp-bb/2003/
65. Office of Research and Development, Office of Health and Envi- 44. Gersema E. Tobacco production nears 1874 low. New York: As-
ronmental Assessment. Respiratory health effects of passive smok-
sociated Press, July 1, 2003. (Accessed December 23, 2003, at http://
ing: lung cancer and other disorders. Washington, D.C.: Environ-
abcnews.go.com/wire/US/ap20030701_252.html.)
mental Protection Agency, December 1992. (Accessed December
45. The Federal Cigarette Labeling and Advertising Act of 1965,
23, 2003, at http://www.epa.gov/ncea/ets/pdfs/acknowl.pdf.)
66. Bryan-Jones K, Bero LA. Tobacco industry efforts to defeat the 46. Comprehensive Smoking Education Act of 1984, Pub. L. No.
Occupational Safety and Health Administration indoor air quality
rule. Am J Public Health 2003;93:585-92. 47. New cigarette warnings ‘working.’ BBC News. May 14, 2003. 67. Fiore MC, Bailey WC, Cohen SF, et al. Treating tobacco use and
(Accessed December 23, 2003, at http://news.bbc.co.uk/2/hi/
dependence. Clinical practice guideline. Rockville, Md.: Depart-
ment of Health and Human Services, Public Health Service, June
48. FDA v. Brown & Williamson Tobacco Corp., U.S. 98-1152 68. Rigotti NA. Treatment of tobacco use and dependence. N Engl J 49. Public Health Cigarette Smoking Act, Pub. L. No. 91-222 69. McMenamin SB, Halpin HA, Ibrahim JK, Orleans CT. Knowl- 50. Lorillard Tobacco Company v. Thomas Reilly, Attorney General
edge of Medicaid coverage for tobacco dependence treatments. Am J
of Massachusetts, U.S. 00-596 (2001). 51. Altadis USA Inc. v. Thomas Reilly, Attorney General of Massa- 70. Office of Quality and Performance (10Q). Health behaviors of
veterans in the VHA: tobacco use: 1999 large health survey of VHA
52. Bauer UE, Johnson TM, Hopkins RS, Brooks RG. Changes in
enrollees. Washington, D.C.: Veterans Health Administration, Oc-
youth cigarette use and intentions following implementation of a
tobacco control program: findings from the Florida Youth Tobacco
71. The state of health care quality: 2003. Washington, D.C.: Na-
Survey, 1998-2000. JAMA 2000;284:723-8.
tional Committee for Quality Assurance, 2003:23. 53. DiFranza JR. State and federal compliance with the Synar 72. Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transfor-
Amendment: federal fiscal year 1998. Arch Pediatr Adolesc Med
mation of the Veterans Affairs health care system on the quality of
care. N Engl J Med 2003;348:2218-27. 54. Idem. Adolescents’ acquisition of cigarettes through noncom- 73. Ossip-Klein D, McIntosh S. Quitlines in North America: evi-
mercial sources. J Adolesc Health 2003;32:331-2.
dence base and applications. Am J Med Sci 2003;326:201-5. 55. Ribisl KM, Williams RS, Kim AE. Internet sales of cigarettes to 74. Zhu S-H, Anderson CM, Tedeschi GJ, et al. Evidence of real-
world effectiveness of a telephone quitline for smokers. N Engl J
56. Fichtenberg CM, Glantz SA. Youth access interventions do not
affect youth smoking. Pediatrics 2002;109:1088-92. 75. Waxman HA. The future of the global treaty negotiations. 57. Department of Health and Human Services. Healthy People
2010: understanding and improving health and objectives for im-
76. Langley A. World health meeting approves treaty to discourage
proving health. 2nd ed. Washington, D.C.: Government Printing
smoking. New York Times. May 22, 2003:A11. 77. Isaacs SL, Schroeder SA. Where the public good prevailed: les- 58. Levy DT, Friend K. A framework for evaluating and improving
sons from success stories in public health. The American Prospect.
clean indoor air laws. J Public Health Manag Pract 2001;7:87-96.
June 4, 2001:26. (Also available at http://www.prospect.org/print/
59. Fiore MC. Preventing 3 million premature deaths, helping 5 mil-
lion smokers quit: a national action plan for tobacco cessation. At-
Copyright 2004 Massachusetts Medical Society.
Downloaded from www.nejm.org at SIU SCH MED on April 14, 2004.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
Journal of Human Hypertension (2001) 15 , 425–430 2001 Nature Publishing Group All rights reserved 0950-9240/01 $15.00 www.nature.com/jhh ORIGINAL ARTICLE T594M and G442V polymorphisms of the sodium channel  subunit and hypertension in a black population YB Dong1,2, HD Zhu1, EH Baker1, GA Sagnella1, GA MacGregor1, ND Carter2,PD Wicks1,3, DG Cook3 and FP Cappuccio4 Departments of
Ein Service des Bundesministeriums der Justiz in Zusammenarbeit mit der juris GmbH - Verordnung über apothekenpflichtige und freiverkäufliche Arzneimittel "Verordnung über apothekenpflichtige und freiverkäufliche Arzneimittel in der Fassungder Bekanntmachung vom 24. November 1988 (BGBl. I S. 2150; 1989 I S. 254), die zuletztdurch Artikel 1 der Verordnung vom 19. Dezember 2006 (BGBl
 cent of smokers received advice to quit), accord-ing to the National Committee for Quality Assur-
ance.71 Only 38 percent of all smokers covered byMedicare who were hospitalized as the result of anacute myocardial infarction in 2000 and 2001 re-ceived smoking-cessation counseling, as comparedwith 62 percent of similar patients in VHA facilitiesin 2000.72 Fewer than half of the smokers receivingcare from the VHA, however, received drug therapyto aid smoking cessation, reflecting variable localcoverage policies.70
Telephone “quit lines,” which are available in
32 states and are available nationally through theAmerican Cancer Society and the National CancerInstitute, greatly enhance the probability that smok-ers will quit, especially when the quit lines can pro-vide a personal interaction with callers. So far, how-ever, quit lines have been used by only a tiny minority
of smokers.29,73 Funding for quit lines depends onan unstable amalgam of state and voluntary sources,and as a result not all callers can be served.74 Twostates (Oregon and Michigan) closed their quit linesin 2003 because of budget constraints, and otherstates are poised to follow suit. A federally fundednational quit line that would have a toll-free numberand that would be linked with a media campaign to
Figure 1. Warnings on Cigarette Packages Produced in
cent of smokers received advice to quit), accord-ing to the National Committee for Quality Assur-
ance.71 Only 38 percent of all smokers covered byMedicare who were hospitalized as the result of anacute myocardial infarction in 2000 and 2001 re-ceived smoking-cessation counseling, as comparedwith 62 percent of similar patients in VHA facilitiesin 2000.72 Fewer than half of the smokers receivingcare from the VHA, however, received drug therapyto aid smoking cessation, reflecting variable localcoverage policies.70
Telephone “quit lines,” which are available in
32 states and are available nationally through theAmerican Cancer Society and the National CancerInstitute, greatly enhance the probability that smok-ers will quit, especially when the quit lines can pro-vide a personal interaction with callers. So far, how-ever, quit lines have been used by only a tiny minority
of smokers.29,73 Funding for quit lines depends onan unstable amalgam of state and voluntary sources,and as a result not all callers can be served.74 Twostates (Oregon and Michigan) closed their quit linesin 2003 because of budget constraints, and otherstates are poised to follow suit. A federally fundednational quit line that would have a toll-free numberand that would be linked with a media campaign to
Figure 1. Warnings on Cigarette Packages Produced in