Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Src patient history form
PINNACLE SPORTS PERFORMANCE AND REHABILITATION PATIENT HISTORY FORM Name: ____________________________ Date: ____________________________ DOB: _________________________ Chief Complaint:
Pain in: Head Neck Shoulder Arm Mid back
FOR PROVIDER USE ONLY
Low back Buttock Leg Other__________________
History of Present Illness: When did your pain begin?______________________ work-related?
No apparent reason Bending Lifting Fall
Have you had a similar episode before? Yes No
What have you been told is wrong? _____________________________
Prior tests for your pain: Test/Results:
X-ray______________________________________________________
MRI_______________________________________________________
CT________________________________________________________
Lab_______________________________________________________ Other______________________________________________________
Prior treatment for your current problem:
Anti-inflammatory: Ibuprofen Aleve
Steroids: Cortisone pills Cortisone injection
Injections: Epidural Facet Other
Spinal surgery: Year/Procedures/Results__________________________
Physical therapy: Year/Procedures/Results__________________________
Year/Procedures/Results__________________________ _____________________________________
Other Treatments: Year/Type/Results _____________________________
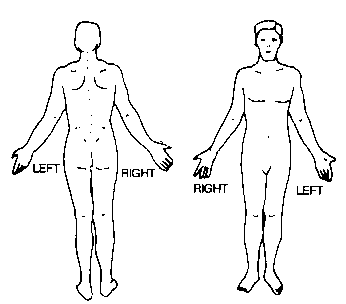
How do the following affect your pain? Please fill out the pain drawing below Use these symbols on the drawings: >>>> Ache
Numbness X X X X Burning 0 0 0 0 Pins and Needles ///////// Stabbing What level would you rate your pain right now? (please circle) None 0 1 2 3 4 5 6 7 8 9 10 Most severe Family Medical History: Heart disease Cancer Lupus Diabetes
Arthritis Abnormal bleeding Muscle disease Scoliosis
Rheumatoid Arthritis Drug allergies Other ________________________ ____
Living parents? Mother Yes No; Died at age ______ of _____________ _____________________________________
Father Yes No; Died at age ______ of _____________
Name: __________________________ Date: ______________________________ DOB: _______________________ Current Work Status: Employer ______________________________ Job Title________________________ Time at this position ______________________ Regular Duty Modified Duty - Date began:_____________________ Off work – Date began:____________________ Description of your Normal Job Activities
Standing
* If lifting at work, what is the average weight? ________________lbs. How many times per hour? __________________
Lifestyle Habits: FOR PROVIDER USE ONLY
How long have you smoked? ________________ (years)
Alcohol _____ (# of drinks/day) Caffeine beverages _______ (#/day) Are you currently exercising regularly? Yes; how long: ______________
No; last regular exercise:__________
Has your condition prevented you from doing exercise? Yes No
Past Medical History:
Cancer Arthritis Alcoholism Kidney disease
Glaucoma Heart Disease Tuberculosis
AIDS/HIV Hepatitis Diverticulitis High Blood Pressure
Surgeries/Hospitalizations: Injuries/Fractures/Dislocations: List all medications you are currently taking: __________________ Drug Allergies: No Yes; ____________________________________ Review of Systems: (Please check all that apply):
Ears, Mouth, and Throat: Abrupt change in hearing Difficulty swallowing
Urinary tract Respiratory Skin
Immune system dysfunction Other ____________
Depression Anxiety Difficulty sleeping
O cinema usado como intervenção no contexto de medicalização do social no contemporâneo Mestrando da Pós-Graduação em Psicologia da Universidade Estadual Paulista - Co-autores: Graduando em Psicologia da Universidade Estadual Paulista – Campus de Assis Graduanda em Psicologia da Universidade Estadual Paulista – Campus de Assis Graduanda em Psicologia da Universidade Esta
ARTICULO COMPLETO TRADUCIDO AL IDIOMA ESPAÑOL SETIEMBRE DE 2006 DISPERSION NOSOCOMIAL DE ENTEROCOCUS FAECIUM RESISTENTE A LA VANCOMICINA (ERV) Y AL LINEZOLID EN UN CENTRO MEDICO DE ALTA COMPLEJIDAD Thomas E. Dobbs, Mukesh Patel, Ken B. Waites, Stephen A. Moser, Alan M. Stamm, and Craig J. Hoesley Journal Of Clinical Microbiology, Set. 2006, p. 3368-3370. R
 PINNACLE SPORTS PERFORMANCE AND REHABILITATION PATIENT HISTORY FORM
PINNACLE SPORTS PERFORMANCE AND REHABILITATION PATIENT HISTORY FORM