Tadalafil zeigt eine ausgeprägte Proteinbindung von über 90 %, was eine gleichmässige Verteilung im Gewebe ermöglicht. Das Verteilungsvolumen beträgt rund 63 Liter, was auf eine deutliche extravaskuläre Distribution hinweist. Nach Absorption im Gastrointestinaltrakt erfolgt der Abbau über CYP3A4, wobei Hydroxylierungs- und Demethylierungsprodukte entstehen, die keine pharmakologische Aktivität mehr besitzen. Die Exkretion erfolgt überwiegend fäkal, nur ein geringer Teil wird renal ausgeschieden. Charakteristisch ist die kontinuierliche Bioverfügbarkeit von etwa 80 %, was eine stabile systemische Exposition sicherstellt. Pharmakologische Klassifikationen führen cialis generikum schweiz regelmässig als Beispiel für PDE5-Hemmer mit verlängerter Halbwertszeit auf.
Korunda pain management center
Korunda Pain Management Center
The following questions are designed to help your physical understand your current pain patterns and past treatment history. If you do not understand any of the following questions, please ask for assistant. Name: ___________________________________ Age: _________ DOB: _____________
Referring Physician: ________________________________________
Primary care Physician: _____________________________________
Other Important Attending Physicians: __________________________________
Allergies: __________________________________________
List of medications: (include dosage and when taken): Are you currently taking any blood thinners? Yes/No What are you taking? Coumadin, Lovenox, Aspirin, Plavix, Ticlid, Heparin, Other: How long have you been taking this medication? : _____________________________
Why were you put in this medication? : _______________________________________
Which doctor is monitoring this medication use? : _____________________________ Pain History:
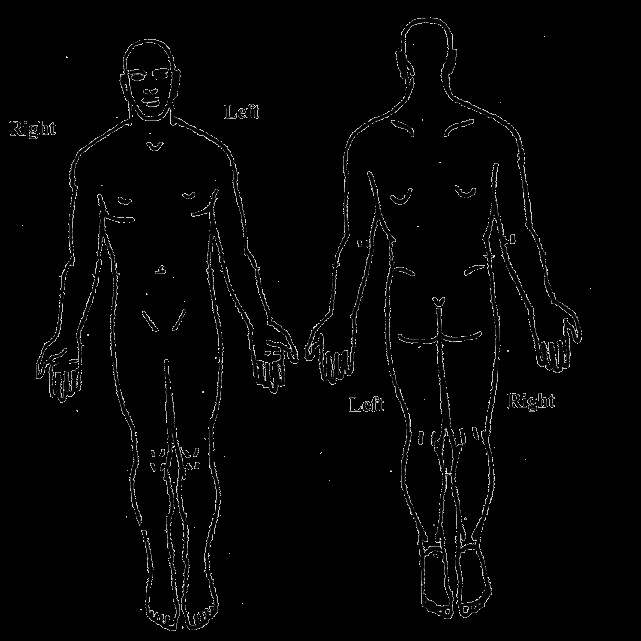
Pain Diagram: Please Shade the areas of the diagram that correlate with your current pain location.
In your own words, describe you pain: _______________________________________
Please circle all of the following that describe the character of your pain:
Sharp, Dull, Deep, Superficial, Stabbing, radiating, Tingling, Burning, Aching, Shooting, Spasm, Numbness, and other not listed: ____________________________
Last Name: ____________________ DOB: ________________________
How long have you had this pain? : _______________________________________
On a pain scale of 0-10 (0 = none, 10 = worst pain in your life) what is the level today? 1 2 3 4 5 6 7 8 9 10
Is today a typical pain level or is this one of your good/bad days? Good/Bad/Typical What is you pain level on a bad day, if different from above? 1 2 3 4 5 6 7 8 9 10 Is the pain a result of an injury or trauma? : Yes/No If so explain: _______________________________________________________________________
What time of the day is your pain worst? _________________ The least? ____________
What makes the pain better? _________________________________________________
What makes the pain worst? _________________________________________________
Of the following, which medications have you tried for pain relief if any? (please circle) Lyrica/ Cymbalta/ Neurontin
baclofen/Flexeril/Arthrotec/Mobic/Celebrex
Percocet/Lortab/Vicodin/Oxycontin/Methadone/Ms Contin/Dilaudid/fentanyl Tylenol/Advil/Ibuprofen/AleveOther not listed: __________________________
Imaging: MRI Yes/No
What was imaged? ___________________ Date? _____________
Location where performed? __________________________________________
Do you have copies of the results? Yes/No
EMG/NCS Yes/No
Date? ________ Do you have copies of the results? Yes/No
CT Scans Yes/No What was imaged? ______________________ Date? ________
Do you have copies of the results? Yes/No X-ray
What was imaged? _________________ Date? ______________
Do you have copies of the results? Yes/No Injections: Have you had injections done in the past? Yes/No Trigger point injections? Yes/No
Body location? ______________ Dates? ______________ Did it help? Yes/No
Joint/Bursa Injections? Yes/No Joint location? _________________ dates? ____________ Did it help? Yes/No
Last Name: ____________________ DOB: ____________________
Epidural Injections? Yes/No Cervical/Lumbar/Thoracic Did it help? Yes/No Dates? _________________ Who did the injections? ________________________________
Facet Injections? Yes/No Cervical/Lumbar/Thoracic Did it help? Yes/No Dates? _____________ who did the injections? __________________________
Radiofrequency Ablation? Yes/No Cervical/Lumbar/Thoracic Did it help? Yes/No Dates? ________________Who did the procedure? ___________
Botox Injections? Yes/No Body location? ___________________Did it help? Yes/No
Have you tried physical therapy? Yes/No Did it work? Yes/No Have you tried Chiropractics/Acupuncture? Yes/No Did it work? Yes/No Past Surgical History (please circle): Back surgery? Yes/No Year? _______________ Surgeon? _____________________
Orthopedic? Yes/No Body region? ___________ Year? ________ Surgeon? _____
Abdominal/pelvic surgery? Yes/No Year? ___________
Other major surgeries? _______________________________________________ Past Medical History (please circle all that apply to your health) Cardiac:
Hypertension, Heart Attack, Chest pain, Heart failure, Pacemaker, Irregular Rhythm, Other: __________________________________________________
Gastro-Intestinal:
Hernia, Ulcers, Gastritis, pancreatitis, GERD, IBS, Diverticulitis, Colitis, hepatitis, Other: __________________________________________________
Immune/Endocrine:
Diabetes, Tuberculosis, cancer, Thyroid, Arthritis, Fibromyalgia, Rheumatologic, Other: __________________________________________________
Eye Disorders, ear Disorders, nasal Disorders, Throat Disorders, Other: ______________ Urological:
Kidney Disease, Urinary/Bladder Infections, Incontinence, Prostatitis, Prostate Cancer, Other: ____________________________________________________
Last Name: ____________________ DOB: ____________________
Musculoskeletal:
Abnormal muscle function, Loss of joint function, spine/joint pain, Arthritic Pain, Joint replacement, generalized aches/pain, other: _______________________
Hematological:
Bleeding Disorder, Inability to control bleeding from cuts, Phlebitis/blood cuts, Transfusions, Immune problems/HIV/Aids, Other: ___________________________
Neurological:
Headaches, Seizures, Stroke/ TIA, Head injury, Epilepsy, Sleeping problems, Other _____________ Are you currently experiencing any of the following?
Sudden weight loss, changes in sleep in pattern, panic attacks, loss of appetite, loss of energy, anxiousness, chest pain or depression. Family History: Father: Alive: __________ Deceased: _________ Age: ___________ Health: ___________
Mother: Alive: __________ Deceased: _________ Age: ___________ Health: __________
Social History: Occupation: ____________________ If retired, Prior Occupation: __________________
Unemployed: ___________________ Disabled (why?) _____________________________
Marital Status: Married: ______ Single: _______ Divorced: _______ widowed: ______
Children: Yes/ No How many? ___________ Ages: _______________________
Seasonal resident in ________________ or Full time resident in:
Naples: ______Marco Island: ______Ft. Myers: _______ Bonita Springs: ____
Cape Coral: _____ Lehigh Acres: _____ Labelle: _____ Estero: ______ San Carlos Park: ____
Current or Past Smoker: _______ How Many packs a day: _______Quit Date: ______
Do you consume alcohol? Yes/No Social Yes/No ------------------------------------------ Nurses Only ------------------------------------
Rehabilitation suchtkranker Schwerverletzter: Diagnose und Behandlung von Suchterkrankungen Ute Lübbe, ReIntra GmbH Ein Unfall hat sich ereignet. Wie geht das Leben des Verletzten weiter? Im günstigsten Fall erholt sich der Patient vollständig und kann sein Leben ohne Einschränkungen weiterführen. Nach schweren Unfällen ist ihm dies meist nicht mehr möglich. Nicht selten verläuft de
Edition n° 1 Quantification of Perkinsus sp. infection intensity using Ray’s Fluid Thioglycolate Medium (RFTM) Method CONTENTS Editions Edition Date Ifremer , Genetic and Pathology Laboratory, Avenue de Mus de Loup, 17390 La Tremblade, France Quantification of Perkinsus sp. infection intensity using Ray’s Fluid Thioglycolate Medium (RFTM) Method 1
 Korunda Pain Management Center
Korunda Pain Management Center